
|
|
Evaluation of Muscle Tone Postural Tone and Balance Muscle Tone and the Stretch Reflex Dystonia Cerebral Palsy Hypotonicity Hypertonicity Muscle Weakness Psychomotor Responses Pathologic Weakness Muscle Fatigue Types of Paralysis Flaccid Paralysis Spastic Paralysis Muscle Soreness and Stiffness Muscle Cramps and Spasms Neuromechanisms Etiology Abdominal Cramps General Spasms Painful Splinting Fatigue Spasm Muscle Trauma Local Movement Disturbances Fibrillation Fasciculation Tics and Habit Spasms Myokymia Tremors Myoclonus 0 Chorea and Coreiform Movements Ballismus and Hemiballismus Athetosis Dystonic Movements Ataxic Movements Convulsions and Seizures Miscellaneous Types of Movement Disturbances Gait Disturbances Muscle Analysis During Gait Neurologic Gaits Paralytic Gaits Psychomotor Disorders Effects of Spinal Adjustments on Gait Reflexes General Types of Reflexes Somatosomatic Reflexes Somatovisceral Reflexes Psychosomatic Syndromes Evaluating the Motor System Examination Protocol Tendon and Periosteal Reflexes Muscle Strength Testing 0 Electrodiagnosis Electromyography Evaluating the Cerebellar System 0 Evaluating Cranial Nerve Motor Fibers BibliographyChapter 9:
Clinical Disorders and the Motor System
From R. C. Schafer, DC, PhD, FICC's best-selling book:
“Basic Principles of Chiropractic Neuroscience”
The following materials are provided as a service to our profession. There is no charge for individuals to copy and file these materials. However, they cannot be sold or used in any group or commercial venture without written permission from ACAPress.
All of Dr. Schafer's books are now available on CDs, with all proceeds being donated
to chiropractic research. Please review the complete list of available books.
Overview Basic Neuromuscular Activities Muscle and Joint Correlations Muscle Mass and AtrophyThe Determination of Atrophy Local Atrophy Types of Atrophy and Their Differentiation Muscle Tone
Chapter 9: Clinical Disorders and the Motor System
Such clinical features as fatigue, weakness, nervousness, pain, tenderness, paralysis, sensory loss, paresthesia, and abnormalities of muscle mass or tone are the most common signs and symptoms noted in neural disorders. Fatigue, weakness, and nervousness are frequently presented together. This triune can usually be attributed to a functional disorder or appear as a complication in organic disease.
(1) impaired movements,
Common types of motor lesions are shown in Table 9.1.
This chapter describes the clinical implications of abnormal muscle mass, tone, and weakness. The primary features of muscle pain, stiffness, cramps, spasms, movement disturbances, and paralysis are described. The chapter concludes with a description of motor reflexes and the neurologic basis for the evaluation of the somatic motor system, including the cerebellar system and the cranial nerves.
OVERVIEW
Abnormal striated muscle function has its origin in diseases of the brain, spinal cord, peripheral nerves, or muscle tissue itself. Dysfunction occurs in a variety of symptoms and signs such as
(2) spontaneous movements,
(3) coordination defects,
(4) abnormal reflexes,
(5) distortions of muscle tone, and
(6) postural and movement distortions. Weakness, wasting, and sometimes paralysis are represented in these conditions.
Table 9.1. Common Types of Motor Lesions
UPPER MOTOR NEURON LESIONS Motor Cortex Brain Stem Cerebral palsy (birth Inflammation injuries, etc) Multiple sclerosis Inflammation Neoplasm Neoplasm Trauma Skull fracture Vascular lesions Internal Capsule Spinal Cord Embolism Combined sclerosis Hemorrhage Inflammation Inflammation Lateral sclerosis Neoplasm Multiple sclerosis Stroke Neoplasm Thrombosis Trauma LOWER MOTOR NEURON LESIONS Anterior Horn Peripheral Nerve Amyotrophic and other Demyelination disease combined conditions Entrapment Poliomyelitis Inflammation Progressive muscular Trauma atrophy Spinal Root and Nerve Muscle Inflammation Amyotonia congenita IVD protrusion Muscular dystrophy Osteophyte Myasthenia gravis Subluxation complex Myotonia congenita
Basic Neuromuscular Activities
The strength of healthy muscle is generally proportional to its size (bulk). The term atrophy refers to the loss of muscle bulk as the result of disease. Atrophy is especially difficult to evaluate in the aged or malnourished individual.
A healthy muscle has a small amount of tension even at complete rest. It feels resilient rather than flabby. Palpable muscle firmness is normally the result of a slight sustained flow of low-frequency asynchronous impulses from the spinal cord generating slight contractions of a small fraction of skeletal muscle fibers plus any degree of active tension. Flexion dystonia, exhibiting a sustained four-limb flexion posture (pallidal syndrome).
Hemiplegic dystonia, characterized by flexed upper extremities and extended lower extremities, without spasticity. Athetosis is often associated.
Spastic dystonia, featuring the same picture as hemiplegic dystonia except the spasticity is overt.
Torsion dystonia, portraying an attitude of decerebrate rigidity.
The differentiation of various types of dystonia is shown in Table 9.2.
The characteristics of various types of rigidity are as follows: Cogwheel (ratchet) rigidity: extrapyramidal rigidity alternating with releases in muscle tension. It is commonly associated with parkinsonism.
Decerebrate rigidity: constant contraction of all antigravity extensors, which is caused by a lesion between the vestibular nuclei and the superior colliculus.
Decorticate rigidity: constant contraction of upper-extremity flexors and lower-extremity extensors, which is the result of a lesion above the superior colliculus.
Paratonic rigidity (Gegenhalten) involuntary stiffening of a limb against the direction of passive movement. Reverse Gegenhalten refers to the involuntary movement of a limb toward the direction of passive movement. Both types are commonly associated with frontal-lobe lesions and their related behavioral disturbances.
Terminology is often confusing when strength is described. The phrase "isometric strength" (equal in length) refers to muscle activity occurring without muscle shortening. "Isotonic strength" (equal in tone) means muscle activity with shortening of the muscle. Both of these general terms are physiologic misnomers in that there is a degree of length change in isometrics due to tendon stretching; and in isotonics, normal tone is influenced by the altered mechanical advantage and resistance. Strength is also described in terms of dynamic (isotonic), explosive, and static (isometric) types.
Involvement of the Corticospinal Pathway. The stretch reflexes are hyperactive, and there is increased resistance to passive motion and abnormal sensory perceptions. Weakness is usually more pronounced than atrophy..
Disorders with a Fast Rate of Progression. Examples include the muscular dystrophies, inflammatory myopathies, toxic myopathies, periodic paralysis, myasthenic syndromes, muscle tumors, a large variety of atrophies and neuropathies, amyotrophic lateral sclerosis, syringomyelia, and poliomyelitis.
When physical activity is conducted under highly warm-humid conditions, precautions must be taken to avoid dehydration fatigue, heat cramps, exhaustion, and stroke. Under such conditions, muscle cramps result from electrolytic depletion and are temporarily disabling.
True paralysis refers to the complete loss of sensation, muscle function, or the inability to control a muscle or group of muscles. It may be either temporary or permanent.
Weakness is especially pronounced in the musculature of the limbs, and there is great difficulty with movements of the hands. However, incoordination is the more common complaint rather than weakness. Besides the neurologic deficit, incoordination results from the varying degrees of strength between the prime movers and antagonists. Deformity by flexion contraction results when the flexors of a part remain strong while the extensors become weak.
Tender muscles may occur shortly after activity and pass quickly, or they may not appear until up to 48 hours after exercise and persist for several days. Stiffness, a sign of poor physical fitness in the weekend athlete or of unusual stress in the trained athlete, may be confused with minor strain, as both stiffness and strain produce pain due to increased intramuscular pressure. The stiffness syndrome features gradually increasing pain, swelling, and restricted motion.
It has been estimated that from 50% to 60% of the pains and discomforts that the average ambulatory patient has are the direct or indirect result of involuntary muscle contraction. Thus, the physician is compelled to consider the relationship of muscle contraction to pain symptoms in both diagnosis and therapy.
Neuromechanisms
Muscles are often injured by strain, contusion, laceration, indirect trauma, rupture, hernia, and less frequently by disease.
Extrapyramidal disorders produce abnormal tone, movement disturbances, and there may be decreased associated movements and pauses in motion. Such neuromuscular disorders as fibrillation, tics, tremors, convulsions, and spasms can be generally classified as local movement disorders. The early stage of such disturbances is easy to miss if not observed under good lighting. In the late stages, spontaneous movements can often be noticed while taking the history.
Cerebellar tremor. When the tremor is not present at rest or during sustentation but only when an act is being performed, it is called an intention tremor. The tremor of cerebellar dysfunction is invariably an intention tremor, and it is worse at the end of movement. The tremor is at right angles to the direction of movement (eg, from side to side). The muscles involved are hypotonic and other signs of cerebellar disease will be present. In chronic alcoholism, the intention tremor is slow, irregular, and unsteady.
Muscle Analysis During Gait
There are two fundamental types of neuromuscular activity. One type consists of reflex postural contractions, which are the basis of posture and physical attitudes and maintain muscle tone. The other type consists of phasic contractions, which produce movement. Phasic contractions may be either reflex or volitional in origin. While reflex actions are always purposeful, predictable, and involuntary, cortical activity is not.
Neurons carrying phasic and tonic impulses have distinctive characteristics. Phasic motor neurons are large, have a rapid conduction velocity, have a high threshold of physiologic excitability, present large impulses of short duration, and are electrically silent during rest. In contrast, tonic motor neurons are smaller, have a slower conduction velocity, have a lower threshold of physiologic excitability, present smaller impulses of longer duration, and are electrically active during rest.
Muscle and Joint Correlations
Functional and degenerative lesions of joints are principally the result not only of a pathologic process in a joint but of altered function of the motor system as a whole, according to the findings of Janda. Because of their physiologic properties, he believes that the muscles, which represent the most liable link of the motor system, respond early and distinctly in most clinical pictures of functional and degenerative joint disease. However, the muscular reaction is not of the same quality in all muscles: muscles with predominantly postural function tighten and muscles with predominantly phasic function weaken.
To understand the fine control of motion, the separate activity of individual muscles is not as important as their coordinated activity within different movement patterns. Understanding this, states Janda, seems to be the best basis for rational treatment and good long-term therapeutic results.
MUSCLE MASS AND ATROPHY
The Determination of Atrophy
Palpation and mensuration are used to determine muscle volume. Upon palpation, there should be a mass that is symmetrical bilaterally. Measurements should be made with a flexible tape from a bony prominence to the belly of a suspected muscle and the point marked with a skin pencil. This distance should be recorded for future reference, then the circumference at that point is measured.
The same procedure is then conducted on the opposite side. The two sides should be approximately the same circumference unless there is a large degree of unilateral occupational activity. A decrease in size (eg, midcalf or thigh) indicates atrophy and is usually associated with some degree of hypotonicity and a decrease in strength.
Local Atrophy
General emaciation should not be confused with local atrophy. Local muscle atrophy occurs as a result of a peripheral nerve lesion, poliomyelitis, neuritis, or trauma to a spinal nerve. The affected muscle becomes shrunken, poor in tone, and weak in strength. Age, sex, occupation, and right- and left-handedness must be considered.
Weakness, flaccidity, and atrophy occur in the face, tongue, and pharyngeal muscles with disease of the lower motor neurons of the brain stem. The result is described by Daube/Sandok as a breathy, imprecise, nasal speech called flaccid dysarthria.
Types of Atrophy and Their Differentiation
When signs of atrophy are found, it is important to keep in mind those features that distinguish disuse atrophy from denervation atrophy.
Disuse Atrophy
Disuse atrophy occurs with a loss of use. With the possible exception of noxious spinal influences, disuse atrophy is the most common cause of local muscle weakness. It may be the result of immobilization, an occupational lack of use of a particular muscle group, or disuse as a result of painful injury, nerve disease, or muscle disease.
The features of disuse atrophy include moderate reduction in visible muscle size, from mild to moderate diminished muscle strength (with paralysis in upper motor neuron lesions), normal tendon reflexes (hyperactive after initial shock in cases of upper motor neuron lesions), normal response to direct muscle stimulation, and mild slowly progressing atrophy. Pottenger observed that visceral malfunction also can produce these symptoms. In disuse atrophy, the weakness exhibited is proportional to the muscle's bulk.
Denervation Atrophy
Neurogenic atrophy occurs with a loss of innervation. Rapid reduction in visible muscle size, zero voluntary muscle strength, absent tendon reflexes, no response to brief direct muscle stimulation, and rapidly progressing atrophy are characteristic of denervation atrophy. The weakness exhibited is disproportional to the muscle's bulk.
MUSCLE TONE
If the function of the ventral roots is impaired, a muscle loses its basic tone immediately; and the same is true if the dorsal roots containing sensory fibers from the muscle are damaged. Thus, tone must be considered not a property of muscle itself, but of reflex activity.
Evaluation of Muscle Tone
The typical feeling of a normal muscle upon palpation is one of resilience. An increased perception of tone by the examiner denotes a hypertonic muscle; decreased tone, a hypotonic muscle. Tone, age, sex, body structure, occupation, physical avocations, and nutritional status of the patient must be considered in evaluating muscle health.
During passive manipulation of a joint, a slight degree of resistance is encountered in the muscle that is not part of conscious effort by the patient. Thus, it can be said that the chief characteristics of normal muscle tone are (1) subdued activity during relaxation and (2) an involuntary reaction opposing mechanical stretch.
Postural Tone and Balance
Postural tonus refers to the sustained contraction of muscles supporting the upright position. The stimuli producing the volley of nerve impulses that continually excite the postural muscles can arise from every sense organ of the body. For example, postural tone is increased by loud noises, bright lights, strong odors, and jarring shocks. When such stimuli are absent, postural tone diminishes.
The stretch reflex is responsible for regulating tension within various muscle groups that provides the basis of postural muscle tone. Stretch (myotatic) reflexes are tested clinically by testing tendon reflexes.
Muscle Tone and the Stretch Reflex
Muscle tone is sustained by the stretch reflex. Gravity pulls all antigravity muscles, and this stretch elicits muscle tone that reflexively helps maintain the body erect. It is on the foundation of postural muscle tone that all voluntary movements are superimposed.
As explained previously, the stretch reflex is a major component of maintaining muscle tone and is well developed in the antigravity muscles to control body posture. However, although basic muscle tone and postural patterns involve local cord reflexes, they are under brain control (eg, the cerebral cortex, cerebellum, inner-ear proprioceptors). In states of unconsciousness, the body quickly gives in to the force of gravity.
Dystonia
Dystonia means a state of impaired or disordered tonicity. It is a general term that may be applied to either muscular hypertonicity or hypotonicity, or to an imbalance within the autonomic nervous system. Clinically, the term dystonia is often used to describe an abnormal limb position: an alpha-type rigidity from sustained contraction of EMG-normal motor units.
There are four major types of muscular dystonia:
Table 9.2. Types of Dystonia and Typical Causes
FLEXION Degenerative Disorders Toxic Disorders
DYSTONIA Amyotrophic lateral sclerosis Carbon monoxide
Hallevorden-Spatz syndrome Carbon disulfide
Hunt's pallidal degeneration Cyanide
Idiopathic parkinsonism Kernicterus
Olivopontocerebellar atrophy Lead
Pick's disease Manganese
Wilson's disease (late) Nitrous oxide
Alzheimer's disease (late) Phenothiazines
Huntington's chorea (late)
Traumatic Disorders
Infectious Disorders Injury to cortex or globus
Encephalitis pallidus connections
Jakob-Creutzfeldt disease
Meningitis Vascular Disorders
Postencephalitic parkinsonism Diffuse arterial disorders
Syphilis
Tuberculosis
Metabolic Disorders
Anoxia
Fahr's disease
Hypoparathyroidism
Pseudohypoparathyroidism
HEMIPLEGIC Degenerative Disorders Metabolic Disorders
DYSTONIA Dystonia musculorum deformans Anoxia
Huntington's chorea Hepatic encephalopathy
Olivopontocerebellar atrophy
Parkinsonism (some forms) Toxic Disorders
Shy-Drager syndrome Manganese
Striatonigral degeneration Methanol
Wilson's disease (juvenile) Phenothiazines
Infectious Disorders Traumatic Disorders
Jakob-Creutzfeldt disease Birth trauma
Postencephalic parkinsonism Skull trauma
SPASTIC Degenerative Disorders Vascular Disorders
DYSTONIA Familial spastic paraplegia Embolus
Stroke
Metabolic Disorders Thrombosis
Anoxia Vasculitis
Hypoglycemia
TORSIONAL Dystonia musculorum deformans Tentorial herniation
DYSTONIA
Cerebral Palsy Hypotonicity
The general term cerebral palsy refers to any upper motor neuron deficit that has its origin in a perinatal insult. The muscle hypotonia exhibited may be temporary or permanent.
The various types of cerebral palsy are shown in Table 9.3.
Table 9.3. Types of Cerebral Palsy
Type Features
Ataxic palsy The major features are trunk and extremity ataxia,
dysdiadochokinesia, dyssynergia, dysmetria, and
mental retardation.
Atonic diplegia Pronounced hypotonic quadriparesis in the lower
extremities with less weakness in the upper
extremities. There are also inadequate trunk control,
hyperreflexia, and mental retardation. The involved
muscles become spastic after a few years.
Dyskinetic palsy Spontaneous involuntary trunk movements at rest
and after effort. There is mental retardation and
often deafness.
Spastic diplegia The lower limbs are weaker and more spastic than the
upper limbs. There are also pathologic reflexes,
hyper reflexia and mental retardation.
Spastic hemiplegia Unilateral involvement, usually sparing the face.
Other major signs include upper extremity spastic
distally, lower extremity weak proximally,
pathologic reflexes, and hyperreflexia. Retardation
is not present.
Spastic monoplegia One limb is weaker and more spastic than its partner.
Retardation is not present.
Spastic quadriplegia Four limbs are weak and spastic. There are also
inadequate trunk control, pathologic reflexes,
hyperreflexia, and profound mental retardation.
Spastic triplegia Three limbs are weak, spastic, and exhibit increased
deep tendon reflexes and pathologic reflexes.
Retardation is present.
Mixed forms Any combination of the above.
Hypertonicity
With few exceptions, states Chusid, hypertonic and hyperkinetic states are invariably the result of involvement of the extrapyramidal system. There are three major types of hypertonicity: rigidity, spasticity, and flexor spasms.
Rigidity and spasticity are differentiated in Table 9.4.
Table 9.4. Hypertonicity: Differentiation of Rigidity and Spasticity
Feature Rigidity Spasticity
Description Increased tone in opposing Increased tension in a muscle
muscles produces steady muscle dependent on the speed of
resistance to passive speed of passive stretch.
stretch throughout range of
motion.
Release after Slow Rapid, clasp-knife response
shortening
response
Stretch reflex Slow Exaggerated
velocity
Typical cause Lower motor neuron lesion Upper motor neuron lesion
MUSCLE WEAKNESS
Weakness is characterized by feelings of lassitude, tiredness, weariness, depletion, exhaustion, malaise, loss of energy and motivation. Its cause may be general or local. If local, the weakness may be described in lower or upper extremities, either distal or proximal. It may be localized in the trunk, head, or in respiration. A rule of thumb is that proximal weakness is the result of a myopathy, while a distal weakness is caused by a neuropathy.
It is important to analyze weakness in terms of body segments because weakness almost always follows a neuroanatomical distribution in organic disease.
Psychomotor Responses
Weakness without related symptoms or signs suggests an emotional problem (eg, depression). These responses refer to the reaction of musculature to emotional effects on the nervous system as the body depicts its psychologic stresses. They may be environmentally, socially, or intrinsically initiated.
Pathologic Weakness
Inequality in muscle balance has many causes. It may be initiated by trauma, postural distortion phenomena, biochemical reactions, psychomotor responses, paralytic effects, or somatic and visceral responses. Weakness may be the only symptom of an early systemic disease such as Guillain-Barr syndrome.
Primary disease of the neuromuscular system itself (eg, paralytic diseases) affects musculoskeletal tone and strength, thus affecting position and quality of motion. Typical causes of pathologic muscle weakness and spasm are atrophy, muscle rupture, spastic paralysis, flaccid paralysis, myopathy, myasthenia gravis, periodic paralysis, root or nerve disease, upper and lower motor neuron syndromes, parkinsonism, and cerebellar disease.
In weakness or paralysis due to final common pathway disease, there is an inability to obtain voluntary contraction, a loss of involuntary movements, and a loss of reflex contraction of the involved muscles. This weakness is either the result of failure of the action potential to be transmitted to the muscle because of a neural block (eg, impingement, disease process) or the result of diseased muscle fibers that cannot respond to the action potentials of their lower motor neurons.
A thorough evaluation of weakness should consider its site, anatomical origin, and rate of progression.
Weakness Evaluated by Its Site
The site of weakness may be symmetrical, asymmetrical, distal, proximal, or general in distribution. Regardless, the fault may be in the anterior horn cells, myoneural junction, muscles, or be of unknown origin.
In generalized weakness, there is little or no wasting with periodic paralysis, myasthenia gravis, myasthenic syndrome, steroid myopathy, or hyperthyroidism. Wasting will be associated with generalized myositis ossificans, congenital dystrophy with arthrogryposis, and the congenital myopathies.
Weakness Evaluated by Its Anatomical Origin
Weakness originating from a lesion at a particular anatomical location offers characteristic clinical findings.
Involvement of the Anterior Horn Cells. The stretch reflexes are absent or hypoactive. The weakness is generalized, but occasionally distal only. Weakness parallels the atrophy present.
Involvement of the Peripheral Nerves. The stretch reflexes are absent or hypoactive. Weakness is usually distal but sometimes generally distributed. Weakness parallels the atrophy present. Muscle fasciculation is sometimes seen, and paresthesia and sensory changes are usually present.
Involvement of the Myoneural Junction. Stretch reflexes are normal. Fatigue is greater than the weakness, and strength returns quickly with rest after exertion. Muscle fasciculation is rarely present. The disorder is usually seen first in the extraocular muscles, progressing in a variable, fluctuating course.
Involvement of the Muscle Fibers. Stretch reflexes are absent or hypoactive, but the distal reflexes are usually normal. Weakness is proximal and parallels the atrophy present. Muscle fasciculation is rarely present.
Involvement of Function. Stretch reflexes are normal, and there is no fasciculation or atrophy. Cogwheel responses and slowness of motion are present. There is a distinct activity overflow and inconsistency in responses.
Weakness or Paralysis Evaluated by Its Rate of Progression
Weakness or paralysis may have a fast, variable, or slow rate of progression and thus point toward specific conditions.
Disorders with a Variable Rate of Progression. The myoglobinuric myopathies, amyloid myopathy, sarcoidosis, infantile spinal muscular atrophy, myositis ossificans, and myasthenia gravis are examples.
Disorders with a Slow or Static Rate of Progression. Examples include the congenital myopathies, endocrine myopathies, and glycogen storage diseases.
MUSCLE FATIGUE
An excised rested muscle tests alkaline with litmus paper, while a fatigued muscle proves acid because muscle contraction consumes nutrients and oxygen and produces acids as well as the body's major source of heat. Acids accumulating as a result of continued activity apparently tend to contribute to fatigue.
Fatigue may be the only early symptom of myopathy. Either progressing central or local fatigue adversely affects skill: diminished skill is commonly associated with approaching exhaustion. As muscle perfusion is greater in a strong muscle as contrasted with that of a weak muscle, fatigue can be the result of inadequate perfusion. However, the overt signs of pallor and the energy-wasting malcoordination, confusion, and staggering gait are usually blamed on inadequate blood flow to the posture-regulating center. Strength also has an influence on recovery because strength tends to minimize the microtrauma secondary to oxygen lack and local weakness.
TYPES OF PARALYSIS
Spastic paralysis is commonly seen in lesions of upper motor neurons. Flaccid paralysis occurs in the peripheral type of nerve lesions involving the lower motor neurons of the anterior horn cells.
Peripheral nerve paralyses are especially apt to be accompanied by sensory symptoms, electrical changes, and wasting. Brain-originating paralyses have few sensory symptoms (sometimes paresthesias), and slight wasting, mental changes, coma, or convulsions often precede or follow the attack. Cord paralyses may or may not show these associations, but they are often accompanied by disorders of the bladder and rectum.
Flaccid Paralysis
A flaccid type of paralysis exhibits if there is no or extremely poor regeneration after injury. It manifests in the peripheral type of nerve lesions affecting the anterior horn cells, nerve roots, peripheral motor neurons, or myoneural junction. The cause can be anything that will block the flow of peripheral impulses (eg, cord tumor or disease process, root compression, nerve laceration or block, junction deficit).
Muscle tone no longer exists because the nerve is unable to maintain it. The muscles become limp and feel small and flabby. Local reflexes are decreased, strength is diminished, and the muscles involved eventually shrink and possibly become replaced by connective and adipose tissues. Deformity results because normal antagonistic muscles overcome the weakened agonists. Weakness with some paralysis in one longitudinal half of the body is called hemiparesis.
Spastic Paralysis
Spastic paralysis is the clinical opposite of flaccid paralysis. It is seen with lesions of upper motor neurons (Table 9.5). A spastic type of paralysis occurs on the opposite side of the body and below the level of the lesion if it is at or above the medullary pyramid. Increased muscle tone is felt as firmness and stiffness, especially in the arm flexors and the leg extensors. Although the muscles involved show weakness on resistance, they palpate tight and tense at rest.
Table 9.5. Differentiation of Upper and Lower Motor Neuron Lesions
Consideration Upper Motor Neuron Lesion Lower Motor Neuron Lesion
Site Cerebral cortex or Anterior horn or peripheral
pyramidal tract motor neuron
Distribution Diffuse or patchy Segmental (number)
Reflexes
Superficial Absent Absent
Deep Exaggerated Absent or hypotonic
Atrophy Disuse, not prominent Rapid extension, trophic
Trophic lesions Minimal Intense and extensive
Pathologic signs Present Absent
and reflexes
Fasciculations Not present Present
Paralysis
Type Spastic and rigid Flaccid
Location Contralateral hemiparesis Paresis limited to specific
muscles
In some cases, lesions in the brain stem can involve both upper and lower motor neurons. This results in an alternating hemiplegia.
Tran states that the extent of the symptomatology frequently offers the examiner a clue to the location of the disorder. In most chronic pyramidal tract lesions, especially when the trauma has been sudden but not insidious, a partial recovery of control is expected. This occurs mostly in the large proximal muscles of the shoulder and hip. Disorders of the pyramidal tract commonly produce defects that are more conspicuous in the upper limb. This is possibly because highly skilled movements are more prevalent there in comparison to necessary mass contractions.
MUSCLE SORENESS AND STIFFNESS
Most authorities now believe that muscle stiffness is not the result of local accumulation of lactic acid produced by activity. Rather, the stiffness is thought to result from the accumulation of extracellular muscle fluid due to increased capillary filtration pressure in an unconditioned muscle area where the vascular bed is unable to keep up with the necessary vascular return. The dispersal of the accumulating extracellular fluid is also delayed because of the lack of lymphatics within voluntary muscle.
MUSCLE CRAMPS AND SPASMS
Musculoskeletal and peripheral vascular disorders are characterized by associated muscle cramps or spasms. These spasms are powerful involuntary muscular contractions shortening the flexor muscles. The result is extreme, often incapacitating, pains initiated by ischemia and hypoxia of muscle tissue. Such spasms are commonly associated with myositic, fibrositic, and articular disorders.
Hypertrophy and spasm must be differentiated from the muscular enlargement that follows exercise. The increase in muscle bulk following exercise is caused by two factors: (1) the opening of capillaries during activity that are closed during rest; and (2) prolonged activity (months), which appears to increase the size of individual muscle fibers.
The general points of differentiation when restricted motion is found are shown in Table 9.6.
Table 9.6. General Interpretation of Resisted Motion Signs
Response Probable Cause
Strong with excessive range of motion Capsule laxity,
ligamentous instability.
Strong and painful in a specific direction Minor musculotendinous lesion.
Strong and painful in all directions Neurosis, malingering.
Strong with pain on repetitive resisted Arterial flow deficit.
movements
Strong and unchanged pain in all Referred pain syndrome.
directions
Strong, painful, and hypomobile Guarded joint for some reason.
Strong, painless, and hypomobile Contracture, adhesion.
Weak and sharply painful Fracture, dislocation, rupture,
gross pathology.
Weak without aggravation of pain (pain- Neurogenic disorder, muscle or
less or unchanged constant pain) tendon rupture.
Weak and painless in all directions Nonmusculotendinous lesion,
probable neurogenic lesion.
Pain only at specific point of arc Functional entrapment, lax joint,
dislocated tendon.
Pain at one range extreme Subluxation, tissue entrapment,
eroded cartilage.
Painful with gross hypermobility Severe sprain.
Painless with gross hypermobility Ruptured tissues with interrupted
sensory path.
Many motor units normally rest while others are firing; but in the cramp phenomenon, all motor units fire and cause the spasm. Why this happens is not clear, but impaired fluid intake, electrolytic balance, and blood flow are often involved. Cramps are characterized by spontaneous, prolonged, painful muscle contraction, usually occurring in voluntary weight-bearing flexor muscles. They often develop during sleep or soon after violent exertion and may vary from slight contractions to violent spasms.
Muscle spasm is an involuntary and aberrant contraction of a muscle part or whole as a result of some excessive motor fiber stimulation such as irritation of (1) the anterior horn cells by the toxic elements of catabolic debris, accumulations consequent to faulty elimination, and circulatory disturbances; (2) an encroached nerve root from subluxation, paraforaminal congestion, herniated disc, and/or ligamentous thickening; (3) a nerve trunk or plexus; eg, piriformis, psoas major, scalenus anticus contraction; (4) peripheral nerve branches; eg, common peroneus by contracted tensor fascia lata or occipital nerve by suboccipital spasm. Spasm may also occur as splinting secondary to injury as in sprain, avulsion fracture, and compression; within a muscle as the result of direct injury or irritation, often resulting from toxic accumulations; eg, toxic lumbago; or consequent to psychic stress.
Etiology
The primary causes of muscle spasm (from minor to severe) are postural and occupational fatigue, electrolyte imbalance, stress, trauma, emotional tension, psychic conversion syndromes, referred irritation from visceral involvement, and nerve root irritations associated with interosseous derangements.
When a synovial articulation is subjected to excessive stresses or toxic insult, the muscles that move the joint are reflexly provoked into spasm because of the irritation of the articular sensory bed. This spasm, often asymmetrical, will frequently force the joint into greater derangement or compression and thus set up the inimical phenomenon of circulus vitiosus.
With pathologic spasm, the patient's history may show that muscles in painful spasm may be relaxed at times if the muscles are provided a position of physiologic rest and an appropriate therapy is applied.
Heat Cramps. Heat cramps also can cause muscle soreness and stiffness. These cramps are often caused by excessive salt loss. However, other factors may be involved such as muscle anoxia, a blow or strain, or for some yet unexplained reason. Violent exercise too soon after a meal increases the danger of active-extremity cramps because much of the general circulation is diverted to the abdomen for absorption purposes. Hormonal factors may be involved in the female, especially during the menstrual period. Cramps frequently follow drinking ice water or other cold drinks too quickly or in too large a quantity after exercise.
Abdominal Cramps
Abdominal cramps are common and frequently associated with gastralgia and enteralgia in which there is contraction of the muscles of the stomach, intestines, and sometimes of the abdominal wall. Windedness is an acute cause of abdominal pain and is associated with a diaphragmatic cramp.
General Spasms
General myospasm guarding joint motion can be grossly evaluated by watching the body attitude (eg, stiff carriage) and by efforts to bend the joint forward, backward, and to the sides. If the examiner is familiar with the average range of mobility in each direction at different ages and physical condition, this test is usually easy and rapid. Care should be taken to differentiate phasic spasm (usually antalgic) from frequently exhibited reflex hypertonicity.
It is one thing to find muscle spasm present and another to determine if it is protective, compensatory, hysterical, or a causative factor. Careful analysis of the dynamic motion of the involved joint is an important method of gaining differential clues. Limitations of motion due to spasm are seen with special frequency in joint pathology and subluxation-fixations, but they may occur in almost any form of joint trouble, particularly in the larger joints.
Painful Splinting
Striated muscles, especially the erectors, become painfully splinted (intrinsically immobilized) by spasm, active or involuntary, when they are fatigued. If this is prolonged, trophic changes occur and tone is lost. Splinting differs from ordinary spasm in that relaxation of the affected muscles occurs at rest.
Prolonged pain from bone, muscle, tendon, and joint lesions with resultant long-term splinting or pseudoparalysis may lead to eventual osteoporosis in the involved bones. Joint contractures also can develop. This is another example, similar to a psychic conversion symptom, where a sensory symptom may lead to definite structural changes.
Fatigue Spasm
More neuromuscular energy is expended in human postural, locomotive, occupational, and recreational efforts than in any other vertebrate. Fatigue therefore intrudes itself upon most clinical profiles. A characteristic of all erector muscles of the axial skeleton is that when they experience postural stress fatigue, they go into a splinting-type painful spasm. When such a provoked muscle tires and goes into fatigue spasm as a compensatory necessity, the muscle becomes painful because the spasm impinges upon the neurotendinous and neuromuscular receptors, and trigger mechanisms are created. This pain is usually asymmetrical and of a distorting, compressing nature.
If there is a pre-existing defect, the asymmetrical fatigue spasm may be the burden that triggers a subliminal situation into an acute syndrome or may become the provocative factor in a nagging chronic discomfort that is stubborn to relieve. On the other hand, muscles get stronger with use. The only time a used muscle gets weaker is when its nutrition is absent or reduced. This can be the product of noxious neurologic reflexes of inhibition.
MUSCLE TRAUMA
Frank trauma may cause inflammation, degeneration, etc, and particularly the muscular splinting reaction that muscles make when their surrounding tissues are injured. This alters the position and motion of the structural tissues that are related. Sustained microtrauma, although of a less acute nature, may cause a slow continual irritation and eventually create degenerative changes that similarly alter muscular reaction.
The obvious trauma of a fall or blow that surprises a joint with the intrinsic muscles unprepared will cause a joint sprain with ligament injury, and a sudden slip during a lift is equally damaging to the unprepared muscles or a weak joint. However, the slower trauma of occupational strain is not as easy to visualize. Holding a baseball bat at arm's length to the side for 2 minutes will cause the shoulder to ache within 1 minute; but the big "catch" will be at the lumbosacral level in ensuing hours and days.
A muscle in pronounced traumatic or reflex spasm becomes inflamed. This is likely to produce some degree of transudation precipitation of fibrin, collagen, and mineral salt deposition, and, if extended, this state can easily result in chronic myositis and myofibrosis. The myofascial planes usually become inflamed at the points of major stress, wherein transudation and fibrin formation produce myofascial plane adhesions. Some authorities feel that this process encourages or is the cause of the development of trigger points.
LOCAL MOVEMENT DISTURBANCES
Fibrillation
Fibrillation is a spontaneous, rhythmic episode of irregular twitching contractions of individual muscle fibers or small groups of muscles. The movements are fine, minute, vermicular waves that can rarely be seen or palpated in muscle except possibly under extremely thin skin such as of the tongue and hands. They are best seen on the tongue when the tongue is resting on the floor of the mouth. Fibrillation is usually only discernible by EMG studies. The minute twitching occurs during muscle atrophy or in the presence of a biochemical impairment of the lower motor neurons. The causative lesion may occur at the cord, root, or peripheral nerve level.
Fasciculation
Fasciculation is a spontaneous, isolated contraction (twitch) of individual motor units. The contractions are usually brief, and the quantity of the reactions depends on the size of the muscle involved (extra-ocular vs trapezius). Light percussion of affected muscles usually activates fasciculation.
Fasciculation is a primary sign of anterior horn disease, root disease, or diffuse motor neuron disease (eg, amyotrophic lateral sclerosis), but rarely are the twitches a complaint. The sign is also associated with electrolytic disturbances, myasthenia gravis, and early poliomyelitis (inflammatory stage) or in chronic cord damage (eg, neoplasm, scar, compression).
Fasciculation is more often seen with nerve root compression than it is with more distal peripheral nerve compression. It may be generalized in myokymia, but it usually appears first in the calf muscles. Generalized fasciculation is often described as a "slow shiver." Transient psychomotor benign fasciculation is often seen in normal subjects under stress and offers no clinical significance.
Spontaneous fasciculations persist even during rest. However, contraction fasciculations (nonspontaneous) disappear when the involved muscles are relaxed. Contraction fasciculations may occur during weak muscle contractions and are usually witnessed in the tense patient who has difficulty in relaxing. They are also associated with amyotrophic lateral sclerosis and poliomyelitis.
Tics and Habit Spasms
Tics are brief, recurrent, inappropriate, involuntary twitching movements repeated in the same pattern (stereotyped). The more common tics are twitchings of the eye, side of the face, lips, or arm and shoulder. Tics are commonly the result of habit, encephalitis, or idiopathic extrapyramidal neuropathy. Idiopathic tics usually begin in childhood and diminish in later life. Episodes are frequently precipitated by emotional stress. Tics may be briefly controlled voluntarily, but such control is likely to be followed by an intense episode of contractions.
Gilles de la Tourette syndrome is a disorder of youth characterized by bizarre tics, coprolalia, imitative gestures, and severe behavior changes. Differential diagnosis should give priority consideration to early parkinsonism, chorea, basal ganglia disease, cerebellar lesion, and Wilson's disease.
Myokymia
Myokymia is a benign form of muscle twitching. It is characterized by brief, spontaneous, tetanus contractions of muscles or fiber groups. Sometimes a continual undulation of muscle surface is produced. The muscle movements are slower and more prolonged in myokymia than they are in fasciculation or tics. Myokymia usually occurs without apparent cause but sometimes is associated with metabolic and infectious disorders.
Tremors
Tremors are rapid, oscillating, involuntary movements that usually involve the tongue or hands. There is a state of continuous contraction of individual muscles with a varying pattern of rhythm. A tremor may occur only during rest, only during volitional motion, during postural sustentation (ie, maintaining a specific posture), or during various combinations of these acts.
Tremors may result from fatigue, alcoholism, drug addiction, thyrotoxicosis, anxiety, multiple sclerosis (intention tremor), or Parkinson's disease (rest tremor). The tremor of anxiety, hyperthyroidism, idiopathic dementia, alcoholism, and toxicosis is most evident in the outstretched hands.
To screen for tremor, Olson and associates recommend that the patient be instructed to point closely at (but not touch) the index fingers of each hand. This may bring out a proximal tremor. A patient with essential tremor will show the tremor throughout the range of motion during a finger-to-finger test.
Basic Classes
Essential tremor. An essential tremor is present during intention movements and sustentation but not during rest. It is common to a number of senile, benign, and inherited disorders. The tremor appears in the direction of movement. A staggering gait (titubation) is usually associated.
Metabolic tremor. This type of fine tremor is present with intention and sustentation. It may increase or decrease during rest. Mild pyrexia and tachycardia are often associated.
Rubral tremor. This is a constant tremor. It never disappears and may worsen with intentional activity. The involved muscles are hypotonic, and mesencephalic signs will invariably be present.
Parkinson's tremor. A static tremor at rest that is absent during action or sustentation is characteristic of parkinsonism. It is most noticeable in the upper extremities. Plastic or cogwheel rigidity and hypokinesia are often associated. Anxiety and senile tremors and those associated with early Wilson's disease often resemble parkinsonism, but they are coarser in character.
Parkinson's Disease
Parkinson's disease (paralysis agitans) is a primary or secondary degenerative disease process where deep reflexes are normal and muscle tone is increased to rigidity, especially in the upper flexors and lower extensors. It affects 1.5% of the population over the age of 65, and has four cardinal clinical features: bradykinesia, rigidity, tremor, and a characteristic disorder of posture and gait. The syndrome of bradykinesia and rigidity is called parkinsonism.
One of the most early signs of Parkinson's disease is that the patient rarely blinks his eyes, and this can occur from 5 to 7 years before all symptoms develop. Later, there is a characteristic resting "pill-rolling" tremor in the fingers and a fixed facial expression (Parkinson's mask). Passive extremity flexion and extension result in increasing resistance that collapses and gives way to alternating, jerky, cogwheel motions. While erect, the head and shoulders are stooped. The gait is short, shuffling, and the arms (held at the side) do not swing in rhythm with the legs. The gait is the progressive type. Hyperthyroidism, Wilson's disease, and drug toxicosis should be ruled out early.
Myoclonus
Myoclonus is a state of involuntary, short, rapid, rhythmic bursts of muscle contractions involving individual muscles, groups of muscles, or entire limbs. It may be either generalized or segmental. A sudden jerk or series of jerks may occur with rates as fast as 50—60 per minute or as slow as 5—10 per minute. The disorder is commonly associated with diffuse neuron disease and childhood convulsions.
Myoclonic jerks are likely to occur in the muscles of the limbs, face, and oral cavity, and disappear during sleep. If large groups of muscles are affected, states Chusid, they produce joint movements that may be of sufficient violence to jar patients or throw them to the ground. Palatial myoclonus usually results from lesions in the pathways connecting the red nucleus, the olivary bodies of the medulla, and the dentate nucleus of the cerebellum.
Chorea and Choreiform Movements
Chorea is a disease that results from basal ganglia damage. It is characterized by sudden, spontaneous, irregular, highly variable, purposeless muscle movements, resembling a dancing part. Huntington's chorea is an inherited variety associated with cerebral cortex defects. It is progressive and leads to severe mental deterioration. Sydenham's chorea occurs in children as a result of rheumatic fever, frequently presenting rapid recovery without complications. The direct cause of chorea is sequential firing of agonists and antagonists, resulting in quick jerky motions.
With chorea, the muscles are not as rigid as in paralysis agitans. The condition may occur hemilaterally as a result of a vascular lesion. Grimaces may occur on the face or aberrations may be present in other parts of the body, but, like athetosis, chorea has a predilection for distal involvement. The features are most noticeable in the hands, fingers, face, tongue, and lower extremities.
In the early stages, slight twitching and digit flicking are noticed. In advanced cases, whole extremities are involved.
Choreiform movements are usually the result of a fault in the basal ganglia, their distribution is highly variable, and they may occur during sleep. They begin suddenly and are without rhythm and are generally purposeless, coarse, rapid, and jerky in character.
Ballismus and Hemiballismus
Ballismus (ballism), resembling Huntington's chorea, is exhibited as violent flinging of the extremities by vigorous involvement of the proximal muscles, often to the point of self-injury. The condition represents an extreme lack of inhibitory control. Between episodes, purposeful movements can be conducted. A pathologic substrate of subthalamic involvement is usually associated (eg, a small infarct). In differential diagnosis, chorea, focal seizures, and drug dyskinesia must be excluded.
Hemiballismus (hemiballism) is a rare sign that involves one side of the body and is usually marked in an upper limb. It is characterized by continual malcoordinated activity of the axial and proximal extremity musculature, sometimes insofar as the limb thrashes about and resembles hemichorea. The face is often spared. The onset is usually sudden. In most cases, the cause is a lesion (eg, hemorrhagic softening) of the contralateral subthalamic nucleus.
Athetosis
Athetosis is a disease of the corpus striatum that is characterized by involuntary slow, twisting, repetitive, worm-like movements in the extremities, especially prominent in the wrists, fingers, tongue, lips, jaw, neck, or feet. It is the result of simultaneous firing of agonists and antagonists, which produces continuously writhing snake-like movements. While variable, the clinical picture is always the same in the same patient and ceases only when the patient is asleep.
Athetosis is often noted in spastic paralysis of infants with brain damage that occurred before or at delivery. Pseudoathetosis is the result of severe proprioception loss from whatever cause.
Dystonic Movements
Dystonia usually refers to mobile spasms of the axial and proximal muscles of the extremities. Dystonic movements tend to involve the large portions of the body and have an undulant, sinuous character that may produce grotesque posturing and bizarre writhing, twisting movements of the trunk and body as a whole, with some of the muscles being hypertonic. Torsion spasm (eg, spasmodic torticollis), with resulting twisting or turning movements, is considered a form of dystonia.
Ataxic Movements
Ataxia means a failure or irregularity of muscular activity or coordination. With few exceptions, it especially manifests when volitional motions are attempted. In gait ataxia, the affected individual staggers while walking on a wide base in a manner similar to a drunken gait (unable to stand with the feet together), and usually sways to the side of the unilateral lesion.
The loss of equilibrium is the result of a lack of muscle synergy and not of a defect in the proprioceptive pathway. Closing the eyes in the Romberg station has little worsening effect in cerebellar ataxia. Lesions in the midline of the cerebellum cause a difficulty in maintaining an upright stance.
Convulsions and Seizures
Convulsions and seizures are sudden, violent, involuntary muscular contractions of all muscles or large groups of muscles due to a large variety of intracranial lesions. They may vary in intensity from a momentary lapse in consciousness (petit mal) to prolonged violent convulsions (grand mal).
Tonic vs Clonic Spasms
Convulsions and spasms may be either tonic or clonic. A tonic spasm is a continuous contraction of a muscle or muscles as in trismus. A clonic spasm is marked by alternating contractions and relaxations of the involved muscles such as seen in spasmodic torticollis. Convulsions are common in epilepsy, hysteria, tetanus, uremia, strychnine poisoning, eclampsia, hydrophobia, and lesions of the brain.
Epileptic Seizures
Epilepsy presents a good example of both tonic and clonic convulsions. The seizure is divided into two parts: the first being brief and of the tonic type, the second of the clonic type. Immediately preceding the attack, the patient may have a premonitory symptom of an aura that may vary in different individuals but usually consists of an imaginary vapor arising from the region of the knees toward the head. When the vapor reaches the level of the head, the patient gives a scream, the head and eyes are turned to one side, and the patient passes into the tonic convulsion. This tonic condition may last about a minute, then there is relaxation, after which contractions and relaxations alternate.
In the clonic part of the convulsion, the muscles of the face, eyes, and jaw work convulsively. The head and extremities jerk rhythmically. The action of the jaws may be such as to bite the tongue, causing the foam forming in the mouth to be bloodstained. There may be incontinence of urine and involuntary movements of the bowels. After a duration of 2—3 minutes, the patient passes into the deep epileptic coma. Although tonic and clonic convulsions may occur in other diseases, the mode and manner of onset and the course of the convulsion will differ according to the disease in which it is present.
As described above, grand mal is often preceded by a sensory aura and mild motor disturbances leading to violent convulsions and unconsciousness. The specific pattern of a seizure depends on the specific site of the lesion. A prodromal twitching of a limb or side of the face usually indicates a lesion in the motor area. The perception of a peculiar odor points toward a lesion in the temporal lobe. Perception of flashes of light and other visual phenomena indicates a lesion in the occipital area. A parietal area lesion usually exhibits numbness, tingling, and odd crawling sensations.
Miscellaneous Types of Movement Disturbances
Other forms of involuntary movements may be witnessed. Clonic convulsive movements are focal seizures sudden, brief, rhythmic or irregular, involuntary that usually involve the great toe, thumb and fingers, or perioral area.
Initial localized clonic jerks may progress to prolonged and generalized tonic contractions. Oculogyric crises are involuntary, tonic, upward eye movements that last from a few minutes to several hours and are presumed to be the result of a psychogenic problem, upper brain stem dysfunction, or basal ganglia lesion.
GAIT DISTURBANCES
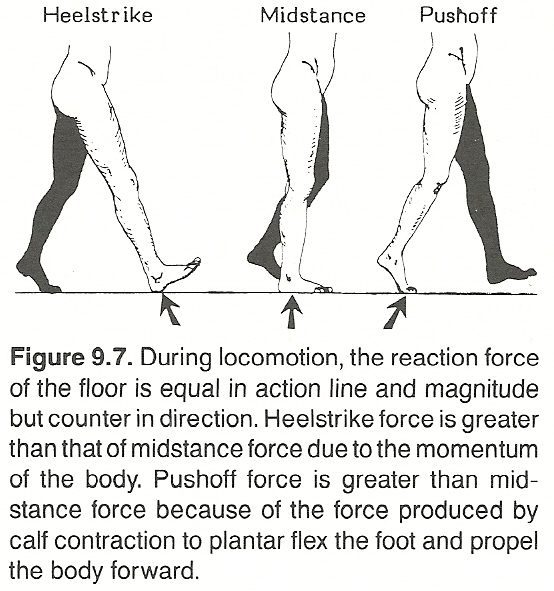
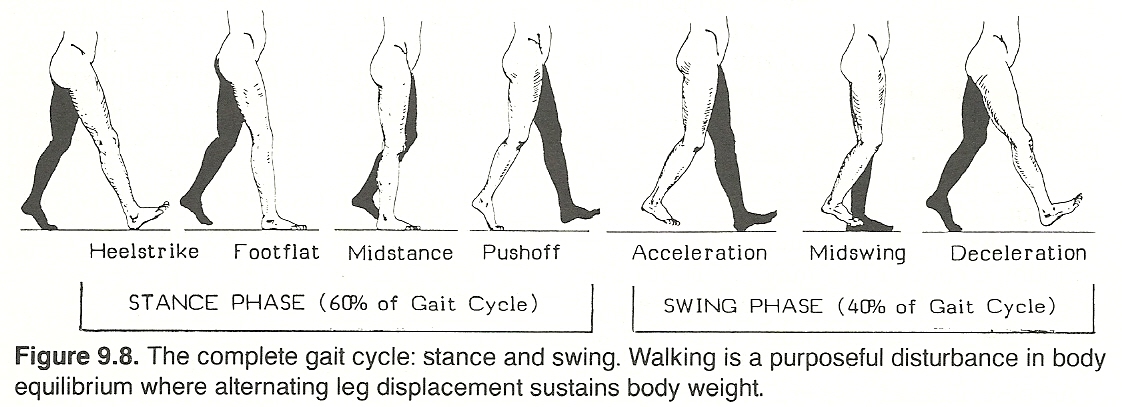
|
In walking, most of these muscles are most active during the beginning and end of the stance and swing phases to accelerate and decelerate the angular moments of the lower extremities. This point is important diagnostically, as it is at these periods of gait that specific muscular disorders will become most apparent. Activity is minimal during midstance and midswing, though this is the period of most obvious movement.
Stance Actions
Immediately after heelstrike, the gluteus maximus is first elongated before its maximal contraction to assure the development of considerable tensile force to the hip. Also during early stance at a moderate speed, the quadriceps becomes elongated and active when the knee is flexed, to smooth flexion up to the point that the center of mass moves anteriorly to the knee. During rapid gait, the quadriceps contract to inhibit knee flexion and begin extension after toeoff.
During the stance phase, the gluteus medius and minimus (hip abductors) are in active lengthening contraction when the pelvis is dropping on the swing side and the femur is being slightly adducted. This helps to stabilize the pelvis. The tibialis anterior and toe extensors rest during midstance, but just after heelstrike, they elongate and achieve their maximum contraction to dorsiflex the foot. At the end of stance, the iliacus is elongated as the hip extends and shortens as the swing phase begins to start hip flexion.
At the time of toeoff, there is slight action by the elongated hamstrings, which increases with walking speed, to increase knee flexion. The initially stretched triceps surae contract when the ankle is in 0ş flexion, just long enough to achieve heel flexion.
Swing Actions
The tensor fascia lata contracts twice during a single cycle: (1) Its maximum contraction occurs when the swing phase is initiated, simultaneous with iliopsoas contraction, as an aid in hip flexion. At this point in gait, the band is elongated before activation. (2) It also contracts at the end of swing and at the start of stance. This is simultaneous with gluteus maximus contraction and resists posterior dislocation of the iliotibial tract where much of the gluteus maximus is inserted.
The thigh adductors are in a state of lengthening contraction at the beginning and during the end of the swing phase. At the end of the swing phase, the hamstrings become elongated and active into early stance to aid hip extension by the gluteus maximus.
Neurologic Gaits
Neurologic gaits are usually the result of unilateral flexor or extensor spasticity. The clinical picture is the result of exaggerated stretch reflexes, reflex impairment of the antagonists, and poor flexor-extensor coordination. Most all spastic gaits exhibit a slow cadence and a repetitive pattern during each cycle.
Unilateral Flexor Spasticity
This gait is characterized by a distinct forward lurch of the trunk, a narrow base of support, a decreased stride length, and an absent heelstrike. Adductor tone is usually normal.
Unilateral Extensor Spasticity
A spastic gait is common in upper motor neuron diseases that have a spastic paralysis of the extensor muscles. It is a feature of spinal paralysis, lateral sclerosis, and some other forms of myelitis and anterior tract or brain damage. The upper body is flexed while the lower extremity is extended.
The locomotion pattern is characterized by a short stride length, a narrow base of support, and pelvic elevation during swing so that the foot will clear the floor. The legs are firmly extended, the back foot is dragged along in a shuffling manner with the toes scraping on the ground to permit one foot to pass the other. There is little knee flexion during the swing phase if the quadriceps are spastic. Heelstrike is absent and the knee is hyperextended in midstance if the plantar flexors are spastic or if the ankle dorsiflexors are weak. Adductor tone is usually normal.
Adductor Spasticity
In some cases of this condition, the adductors become bilaterally spastic to cause the legs to cross (scissors gait) and the knees often scrape each other in passing (eg, Little's disease). The steps are short and progression is slow. The lower limbs are thrust forward in a stiff, jerky manner, which is often associated by pronounced compensatory motions of the trunk and upper extremities.
Mowing (Hemiplegic) Gait
In spastic hemiplegia, as in unilateral extensor spasticity described above, there is a unilateral spastic gait in which the pelvis is tilted and the affected leg is swung around in a semicircle in front of the other with the toes often scraping the ground. The patient leans to the affected side and the ipsilateral arm is held in a rigid, semiflexed position. The spastic limb is thrown forward with difficulty because of the impaired joint mobility.
The hemiplegic limb hangs so that abduction and circumduction of the limb are necessary to move it forward. The most common cause of a mowing gait is hemiplegia due to cerebrovascular disease, but any condition that would result in an upper motor neuron lesion can produce such a gait. On first notice, this paralytic gait can be easily confused with any musculoskeletal disorder restricting the action of a hip or knee.
Proprioception Impairment: Ataxic and Tabeticits
This gait is characteristic of posterior column disease and frequently called an ataxic gait because it occurs in locomotor ataxia. The patient walks in a clumsy, uncertain manner on a wide base in a stooped posture. Each foot is raised unusually high, thrown forward with force, and brought to the ground flat-footedly with a stamp to increase sensory awareness. While in the air and before being lowered, the foot wavers as if there is a degree of uncertainty in bringing it down.
The patient walks with the feet wide apart and is constantly looking at them. This is done to supplement the loss of proprioception. To maintain a large area of foot contact throughout weight bearing, heelstrike is usually eliminated.
An ataxic gait is sometimes called a tabetic gait when it is characteristic of a lesion in the dorsal ganglia, dorsal roots, or posterior column of the cord rarely in higher levels. The ataxia is increased when the eyes are closed or when the patient must walk in a darkened room. This gait is typical of tabes dorsalis but also seen in pernicious anemia and other disorders involving proprioceptive pathways.
Basal Ganglia Dysfunction
This gait is characteristic of paralysis agitans or Parkinson's disease. In these conditions, it is called a propulsive gait or festination (increasing speed). However, an identical gait is also characteristic of drug poisoning, multiple neuritis or sclerosis, brain tumor, and general paresis.
The hurried walk of parkinsonism is the result of the forward tilt of the trunk (in the attitude of a stoop) and the attempt of the patient to maintain balance. As the center of mass is anterior to the base of support, the patient appears to be chasing his center of gravity (marche a petis pas). Almost all joint motion is restricted, as is arm swing, pelvic tilt, pelvic rotation, and knee flexion.
The body and head lean far forward. The trunk, hips, knees, and ankles are flexed to some degree, and the subject walks with short, hurried, shuffling steps, which makes it appear as if the patient is being pushed from the rear and about to fall. Heelstrike is absent, and toes drag during the swing phase. It is difficult for a person with this gait to stop suddenly or to turn a corner. Thus, falls are frequent. Progression is slow at first and then increases rapidly with minimal voluntary control.
Cerebellar Dysfunction
This gait, a sign of cerebellar ataxia, resembles the actions of an intoxicated person. The patient walks with the feet wide apart, takes short steps, and irregularly sways to and fro to such an extent that progression in a straight line is almost impossible. Unsteadiness and a tendency to reel to one side are associated. The lower extremities appear loose. Movement of the advancing limb starts slowly, but the limb appears to be unexpectantly, erratically, and vigorously flung forward to land with a stamp on the floor. Staggering often occurs on turning. The gait resembles that of a person trying to walk on a rolling ship, constantly trying to maintain equilibrium with little success.
This gait is found with tumor of the cerebellum and diseases of the semicircular canals. Cerebellar lesions are invariably associated with vertigo. It may indicate of long-term use of alcohol or other drugs (Jake legs) or high CNS neurosyphilis. If the causative factor is unilateral, deviation is to the involved side because of hypotonia.
Paralytic Gaits
Paralytic or paretic gaits with varying patterns are the result of spinal root lesions, brain lesions, nerve compression syndromes, peripheral mononeuritis, abnormal reflexes, and trauma.
General Considerations
If the quadriceps are extremely weak, locomotion is usually impossible as the knee is too unstable during stance. If knee flexion and plantar flexion are weak during swing, compensation is made by hip elevation. The two typical patterns are referred to as the steppage gait and the waddling gait.
Steppage Gait. This gait is also called the prancing, high-stepping, or foot-drop gait. It resembles that of a person walking in tall grass, hence its name. The flexor muscles of the foot are subject of a flaccid paralysis so that the toes hang downward when the foot is raised from the floor. To prevent the toes dragging on the floor or catching upon objects, the foot is raised high and brought to the floor forcibly before the toes can drop. Thus, the foot strikes the floor heel first or flat-footed. With bilateral footdrop, the gait often resembles that of a high-stepping horse. This gait, the result of paralysis of the anterior tibialis group of muscles, points to tertiary syphilis, alcoholic neuritis, peroneal nerve injury, poliomyelitis, progressive muscular atrophy, multiple neuritis, and arsenic poisoning.
Waddling Gait. This occurs when there is extreme muscular weakness in the thigh and hip muscles as commonly found in pseudohypertrophic muscular paralysis and muscular atrophy or dystrophy where the trunk muscles must be strongly utilized. The shoulders are thrown back, the lower section of the spine is lordotic, the pelvis is severely tilted, and while in this state, the leg is brought around and placed on the floor.
The "waddle" results from difficulty in maintaining the pelvis at an adequate level to the weight-bearing extremity, with slump of the pelvis toward the nonweight-bearing side, which, in turn, produces an exaggerated compensatory trunk sway toward the weight-bearing side.
When walking, the subject swings from side to side in a very noticeable manner, thus it is often called a goose gait. Such a "clumsy" gait is also seen in bilateral hip dislocation. In gaits involving muscle weakness, the compensatory pattern is largely the result of the patient's attempt to alter the center of gravity about the base of support.
Hip Weakness
Extension Weakness. During extension paralysis, the gait is grossly altered in weight bearing after heelstrike when the extensors normally contract. Because of the weakness, the trunk is thrown backward to maintain balance by keeping the center of gravity behind the axis of the hip.
Flexion Weakness. Weak hip flexors affect acceleration during swing, the pelvis is usually elevated, the trunk is thrown backward toward the unaffected side in compensation, but stance is rarely involved. The stride is usually short on the involved side.
Abductor Weakness. In upper motor neuron weakness of the hip abductors, the trunk is thrown toward the affected side during weight bearing. If uncompensated, the pelvis distinctly lunges laterally toward the involved side and dips on the side of swing. At midswing, hip and knee flexion is exaggerated on the unaffected side. In less severe cases, there is little sideward lunging because of trunk compensation. Use of a cane on the contralateral side of involvement also eliminates this lateral lurch.
Knee Weakness
Extensor Weakness. This pattern is often difficult to see. In stance, the knee is normally fully extended. The features of the weakness are most prominent after heelstrike when the quadriceps normally contract and the knee flexes. Signs of excessive heel lift during gait and excessive knee flexion during the swing phase should be sought. Knee extension is maintained at heelstrike and throughout stance by hip extension (eg, the gluteus maximus via the iliotibial tract) and plantar flexion. This is helped by throwing the trunk forward at heelstrike to move the center of gravity anterior to the axis of the knee. In pronounced cases, the patient will push the affected thigh backward with the hand to aid extension.
Flexor Weakness. Weak hamstrings allow full knee extension and inhibit deceleration as heelstrike approaches. This produces a hard heelstrike, often called an "overshot." Near the end of the stance phase, the knee fails to flex until pushoff. In prolonged conditions, the result is often the development of distinct knee hyperextension (genu recurvatum).
Ankle Weakness
Plantar Flexion Weakness. If these muscles are weak, propulsion is inhibited because heeloff is impaired. The foot leaves the floor as a unit, the knee is fully extended, and the hip flexes at pushoff to begin the swing phase. Because pushoff is controlled primarily by foot plantar flexion, triceps surae paralysis or Achilles tendon trauma will force some compensation by the gluteus maximus and posterior hamstrings.
Dorsiflexion Weakness. When the ankle dorsiflexors are mildly weak, it is possible to lift the foot from the floor, but during the swing phase, relaxation occurs, which causes the foot to be slapped down during flatfoot. In severe weakness, toestrike replaces heelstrike. This requires a compensatory increase in hip and knee flexion during the swing phase so that the foot clears the floor (steppage gait).
Psychomotor Disorders
Besides the gaits described, locomotion may be restricted by various types of psychomotor disorders. The two major types are those due to hysteria or central apraxia.
Hysteria
A hysterical gait can simulate almost any type of pronounced paralysis, except during emergencies. The gait is usually bizarre and features exaggerated balancing motions, irregular bobbing movements, lurching, and wild weaving or excessively slow, hesitant steps.
These gaits rarely have a repetitive pattern. It is difficult to match gait signs with neurologic and musculoskeletal findings. Tremor usually appears during observed active exercise, and strength rapidly fades when passive movements are resisted by the patient. Although the motions are gross and unpredictable, falling is rare. If falling occurs, it is well protected. In some chronic cases, the pattern is repetitive. This is usually the result of a "gait habit" that persists long after the cause of malfunction has been eliminated. The clinical picture is often confusing because persistent atrophy, boggy tissues, possible edema, and vasomotor instability may be solely the result of disuse.
Astasia-Abasia
This is a type of hysterical ataxia that features bizarre incoordination to the degree that the patient is unable to stand or walk, yet all movements can be performed normally when the patient is in the sitting or recumbent position.
Gait Apraxia
In this condition, motor power is present but the memory of how to use the power is lacking or diminished. Steps are small, slow, and uncertain, and the patient must be urged or assisted to initiate progress. This gait is characteristic of frontal lobe lesions or bilateral lesions of the corticospinal tract in the internal capsule, cerebral peduncles, or high brainstem. It is often seen immediately following prolonged bed confinement; but in this situation, it is soon overcome with practice.
Effects of Spinal Adjustments on Gait
A surface electromyographic study conducted by Hibbard found that significant amplitude changes occurred in the electrical activity of gait muscles following manipulation of the lower extremity articulations to reduce malposition, while the electrical activity of control subjects decreased only slightly. Hibbard cites the work of Rebechini-Zasadny and associates that had earlier found a significant difference in the electrical activity of peripheral muscle following manipulation of just the cervical spine.
REFLEXES
The human body exhibits an astonishingly complex array of neural circuitry. While the study of reflex communication between tissues under "voluntary" control and tissues under "autonomic" control (and their excitatory and inhibitory effect on one another) is still in its infancy, the answers to why so many visceral disorders mimic musculoskeletal disorders and why so many musculoskeletal disorders parody visceral disorders appear to be on the horizon.
General Types of Reflexes
The reflexes of most concern clinically can be classified into three broad categories.
Somatic reflexes: (1) Reflexes communicating from a site on the body wall, cranium, or limb to another site on the body wall, cranium, or a limb (somatosomatic reflex). (2) Reflexes communicating from a site on the body wall, cranium, or a limb (cutaneous, subcutaneous, musculoskeletal) to an internal organ or gland (somatovisceral reflex).
Autonomic reflexes:. (1) Reflexes communicating from an internal organ or gland to a site on the body wall, cranium, or a limb (viscerosomatic reflex). (2) Reflexes communicating from an internal organ or gland to another internal organ or gland (viscerovisceral reflex).
Psychic reflexes: (1) Reflexes communicating from a site within the higher CNS centers to the body wall, cranium, or a limb (psychosomatic reflex). (2) Reflexes communicating from a site on the body wall, cranium, or a limb to the higher CNS centers (somatopsychic reflex).
All three types of reflexes usually have segmental, propriospinal, and/or suprasegmental implications. Autonomic reflexes will be described in Chapter 10.
Inasmuch as many reflexes are modulated within the spinal cord, their potential interrelationship with a subluxation complex, and vice versa, cannot be ignored when we consider that a vertebral lesion can be a focus for either neuronal hyperexcitability or hypoexcitability. Thus, all afferent fibers entering the IVF and all structures receiving efferent fibers via the IVF are potentially exposed to excessive stimulation or inhibition by some factor producing irritation, pressure, or tension at this vulnerable gateway.
Somatosomatic Reflexes
A somatosomatic reflex develops when a sensory receptor in the skin, subcutaneous tissue, fascia, striated muscle, a tendon, a ligament, or a joint is stimulated to trigger a volley of reflex impulses to another anatomical location of this type via efferent sensory, motor, or autonomic fibers. These reflexes are commonly evoked by gross manipulation, dynamic adjustments, light touch techniques, superficial heat or cold, electrotherapy, meridian therapy, hydrotherapy, traction, compression, vibration, percussion, and massage during case management.
Korr has shown that muscle spindles in which the "gain" has been turned up by intensified activity in their gamma motor innervation may, with other sensory inputs, account for many motion characteristics and palpatory features of a spinal subluxation complex. "Turning down" the gain seems a common denominator in a variety of manipulative procedures.
Somatovisceral Reflexes
A somatovisceral reflex is initiated when a sensory receptor in the skin, subcutaneous tissue, fascia, striated muscle, a tendon, a ligament, or a joint is stimulated to trigger a volley of reflex impulses to viscera. Body wall stimulation produces both segmental organ responses and suprasegmental responses. Different forms of stimulation may produce similar organ responses and may produce different brain center responses that affect the body. The type of response, prolonged beyond stimulus termination, depends on the state of the organ and the body as a whole (ie, active, resting). These reflexes are commonly evoked therapeutically by manipulation, superficial heat or cold, electrotherapy, meridian therapy (possibly), hydrotherapy, traction, compression, vibration, percussion, and massage.
Psychosomatic Syndromes
A clinical appreciation of the psychologic factors involved in backache cases is enhanced by recognizing the most pertinent psychiatric syndromes involved in conversion hysteria.
Spinal-Related Psychiatric Syndromes
A large variety of psychologic disturbances may be associated with backache and other musculoskeletal complaints, either as aggravating factors or as a result of their development for reasons commonly seen in practice. For this reason, the term psychosomatic backache is the preferred term to use to categorize those cases in which such psychologic disturbance constitutes the dominating feature of the overall clinical picture and in which psychologic investigation and treatment is an essential part of their management.
Psychophysiologic Neuromuscular Reactions
A conditioned reflex in which an emotionally stressful situation refocuses awareness on a past physical injury that occurred in a psychologically stressful situation is called a psychophysiologic neuromuscular reaction. The new stress stimulates recall of the experience, and this serves as a stimulus for psychophysiologic responses creating the backache. This renewed attention to the back produces the stimulus for a reflex muscular spasm that, in turn, produces further backache and anxiety and more muscle spasm. Thus, a vicious cycle is established.
Screening Procedures
In evaluating a patient with low back pain, Brown and associates feel strongly that the presence of any four of the below six signs serve as a basis for requesting psychiatric consultation:
A vague history with irrelevant circumstantiality and poor chronology.
Dramatization of illness.
Paranoid attitudes toward the staff.
Nonanatomical distribution of pain. See Figure 9.9 a & b
Failure to respond to appropriate therapies.
Several symptoms of neurosis such as acute or chronic anxiety, insomnia, anorexia, irritability, headache, chronic fatigue, crying spells, trembling, sweating, nail biting, hypersensitivity to light and sound, sighing respiration, and patterns of helplessness, failure, and dependency.
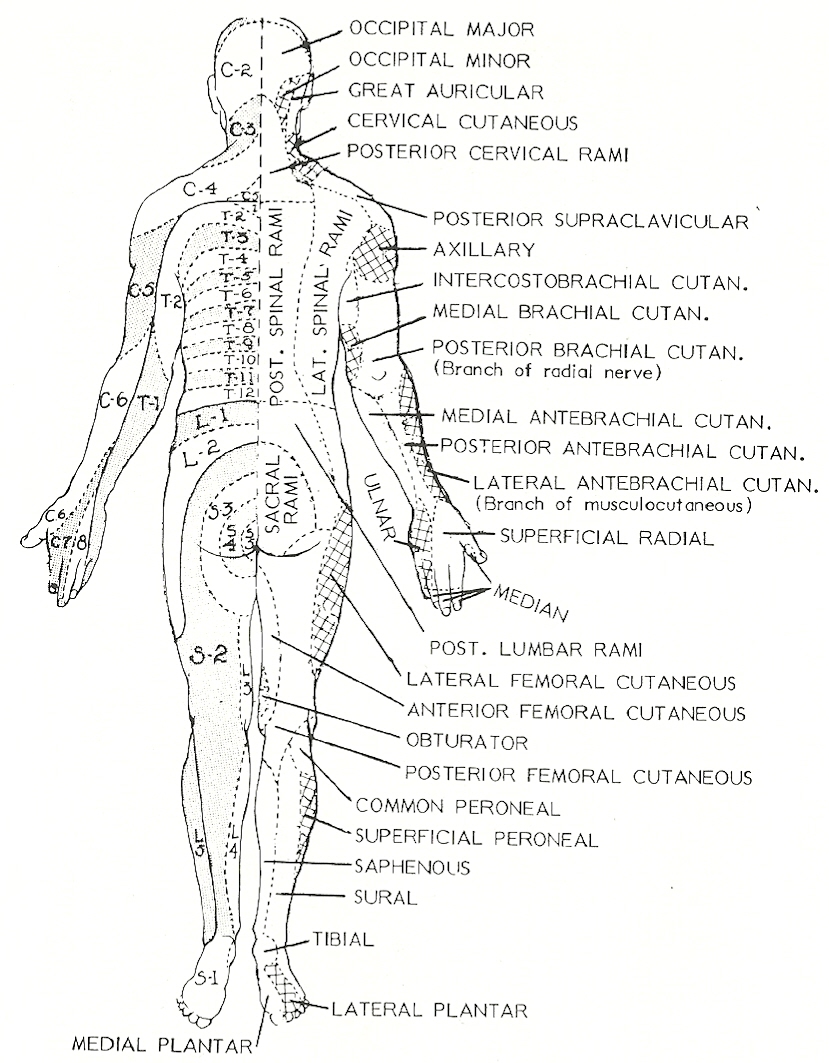
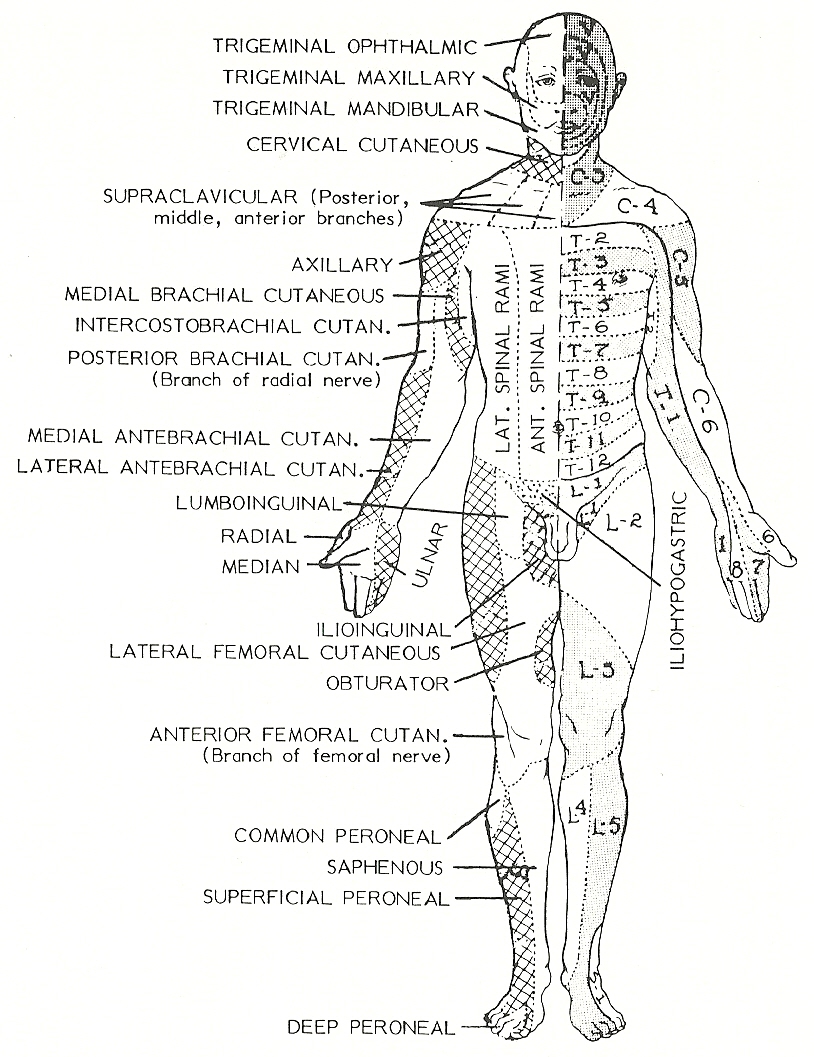
Any sign of muscle weakness, atrophy, paralysis, and incoordination is a significant clinical finding. The muscular aspect of the motor system should be checked for muscle tone, strength, and volume (mass), and nerve integrity is judged by the deep and superficial reflexes. Motor disorders may be caused by the same processes that cause sensory disturbances; eg, direct nerve injury, pathology, reflexes from visceral organs, and particularly nerve root involvement or upper motor neuron lesions.
Motor nerve root involvement is characterized by deep muscular pain in the muscles innervated. Early hypertonicity or muscular spasm is evident. Later or in chronic conditions, loss of tendon reflexes, muscular weakness, atrophy, and even trophic changes in the overlying skin may be present. Motor disturbances from upper motor lesions may also be a factor (hyperreflexia).
Signs of typical motor abnormalities and their related level in the nervous system are shown in Table 9.7.
Supratentorial Posterior Spinal Peripheral
Tracts Level Fossa Level Level
Final Atrophy Absent Absent
common Fasciculations abdominal abdominal
pathway Weakness reflexes reflexes
Atrophy Atrophy
Cramps Cramps
Fasciculations Fasciculations
Hyporeflexia Hyporeflexia
Hypotonia Weakness
Weakness
Direct Absent ab- Absent abddomi- Absent abdominal
activation dominal nal reflexes reflexes
pathway reflexes Babinski reflex Babinski reflex
Apraxia Hyporeflexia Weakness
Babinski re- Hypotonia
flex Weakness
Hyporeflexia
Hypotonia
Seizures
Weakness
Indirect Apraxia Clasp-knife Clasp-knife reflex
activation Clasp-knife reflex Clonus
pathway reflex Clonus Decorticate posture
Clonus Decerebrate Hyperreflexia
Hyperreflexia posture Spasticity
Spasticity Hyperreflexia
Spasticity
Cerebellar Ataxia Ataxia
control Dysmetria
circuit Dyssynergia
Hyporeflexia
Hypotonia
Intention tremor
Past-pointing
Holmes' rebound
phenomenon
Basal Athetosis
ganglia Chorea
control Dystonia
circuit Hemiballismus
Hyperkinesia
Resting tremor
Rigidity
_____________________________
*Adapted from Daube/Sandok with modifications.
Examination Protocol
After nerve trauma, painstaking examination is required as multiple nerve injury, related tendon or other soft-tissue damage, and fractures may complicate the picture. The immediate site of injury should be investigated first, followed by the part's general appearance, voluntary motion, reflexes, and vasomotor changes. Besides sensory and motor loss, the response to electric stimulation should be evaluated whenever the procedure is merited.
Tendon and Periosteal Reflexes
When reflexes are tested, the patient must be relaxed and the part placed in the proper position for each test. As both normal and pathologic reflexes vary widely in people at different times, the examiner should compare reflexes bilaterally when possible and make sure that the same force is used on each side because unilateral differences are common signals of pathology. It should be remembered that abnormal reflexes, particularly if bilateral or similar in other reflexes, may be normal for a particular person. Upper extremity reflexes, especially, are often difficult to evoke even in the healthy. All signs must be correlated.
General Considerations
Muscle movement is the motor response to most reflexes tested. Such tests involve the facilitation or inhibition of the alpha and gamma motor neurons of lamina IX. The alpha motor neurons are the largest of the anterior horn cells and can be stimulated monosynaptically through interneurons in response to segmental, intersegmental, and supraspinal reflexes. All descending tracts in the spinal cord are influential.
It should be noted that: (1) In upper motor neuron or pyramidal fiber lesions, the deep tendon reflexes are exaggerated, but the superficial skin reflexes are decreased or absent. (2) In lesions of a lower motor neuron or the motor fibers from the anterior horn cells of the cord, both the deep and the superficial reflexes are decreased or absent.
While a diagnosis of a neurologic disorder cannot be determined by reflexes alone, they are important aids in establishing the type and location of a lesion. Deep reflexes vary in direct proportion to muscle tone, while superficial reflexes apply to any reflex phenomenon that may be induced by a light stimulus such as stroking the skin with a wisp of cotton, resulting in horripilation (gooseflesh) or muscle contraction.
The afferent, center, and efferent aspects of the deep tendon reflexes are outlined in Table 9.8.
Reflex Afferent Limb Center Efferent Limb Achilles Tibial S1–S2 S1–S2 Biceps Musculocutaneous C5–C6 C5–C6 Jaw jerk Trigeminal Pons Trigeminal Patellar Femoral L2–L4 L2–L4 Radial Radial C6–C8 C6–C8 Triceps Radial C6–C7 C6–C7
Testing a tendon reflex segmentally evaluates the integrity of all components of the circuit (from the muscle spindles to the muscle fibers). This includes the sensory receptors, the afferent nerves, the spinal cord segment(s) involved, the alpha motor neurons and their axons, the apparatus at the neuromuscular junction, and the muscle fibers. The speed and magnitude of the reaction also give clues about adjacent segment and higher control center influence on the efferent neurons (ie, an exaggerated response when the inhibitory influences of the descending tracts are lacking). A grading system for deep reflexes is shown in Table 9.9.
Grade Reflex Reaction
0 Cannot be elicited
–3 Absent except on reinforcement
–2 Markedly decreased
–1 Weak
N Normal
+1 Slightly hyperactive
+2 Markedly increased and often associated with unsustained clonus
+3 Markedly increased and often associated with sustained clonus.
Deep Reflex Techniques
Biceps Reflex. The muscles of the patient's arm are bared and relaxed, and then flexed at the elbow. The examiner places a thumb over the biceps tendon, and then makes a light blow against the thumb with a percussion hammer. Note if the biceps muscle contracts, how quickly it contracts, and with what force. The biceps reflex, a normal response, tests C5—C6 segments in terms of integrity of the musculocutaneous nerve. It is hyperactive in the same disorders that cause a hyperactive knee jerk.
Triceps Reflex. The patient's arm should be relaxed and flexed at the elbow. Support the elbow and tap the triceps tendon where it crosses the olecranon fossa, observing the same phenomena as in the biceps reflex. The triceps reflex tests C6—C8 afferents, cord segments, and efferents. Both the biceps and triceps reflexes may be diminished in healthy patients.
Radial Reflex. With the patient's arm relaxed, flexed, and well supported, tapping the relaxed forearm over the lower radius results in flexion of the elbow. The response, a periosteal rather than a tendon reflex, tests the C5—C6 levels and has the same significance as the biceps tendon reflex. This reflex, absent in many healthy individuals, is frequently called the brachioradialis reflex. In C5—C6 segment lesions, an inverted radial reflex may be seen in which the fingers flex but the forearm remains relaxed.
Ulnar Reflex. This refers to tapping of the styloid process of the ulnar that results in pronation of the hand. The ulnar periosteal reflex is a highly unreliable normal reflex.
Patella Reflex. A rolled hard pillow is placed beneath the knees of a supine patient. With the muscles completely relaxed, the patellar tendon is tapped, and contraction of the quadriceps (L2—L4) is noted. Do not rely on the movement of the foot in response to the tapping. Place one hand on the patient's thigh, and use your other hand for the percussion hammer. Test bilaterally, and compare the force of contraction and quickness of response of the two sides. Absence of the reflex is known as Westphal's sign.
Normal reflex response depends upon the integrity of the femoral nerve and the lumbar segments. Other positions for obtaining the knee reflexes are with the patient sitting on the edge of a bed with muscles relaxed or sitting on a chair with the feet resting on the floor in parallel position. The thighs should be bared and the same methods employed as described previously.
Absent or diminished knee jerks are found in peripheral nerve lesions, anterior horn cell disease, and posterior column lesions. IVD herniation at the level of L2—L4 will diminish the response. Hyperactive responses will be seen in tense patients, corticospinal tract lesions, general pareses, cord tumor compression or bone compression above L3, multiple sclerosis, and early hemiplegia. The knee jerk is often wanting or feeble in young infants. It varies a great deal in persons of different temperament. In high-strung or oversensitive people, lively knee jerks are often seen without disease.
Achilles Reflex. The ankle jerk is obtained best by having the patient kneel in a padded chair with the feet projecting. The patient is asked to relax the feet, then the Achilles tendon is tapped just below the level of the malleoli, comparing the two sides. Ankle jerks are absent bilaterally in tabes dorsalis and frequently in normal old age. The response is increased in lesions of the pyramidal tract. A reduced or absent reflex may point toward a sciatic IVD herniation between L5 and S1 or L4 and L5. If the patient is in bed, flex and externally rotate the thigh and leg to about 45 degrees until the knee rests on the bed or pillow. Grasp the foot with one hand and hold it easily at right angles to the leg. Then tap the Achilles tendon as previously described. Some examiners test this reflex in the sitting position.
Muscle Strength Testing
The clinical art of muscle testing demands attention to detail and a good working knowledge of anatomy, muscle function, muscle origin and insertion, muscle antagonistic and agonistic action, and their role in joint movement and stabilization. The procedure and its evaluation depend greatly on the skill, knowledge, and experience of the examiner.
A patient's muscle power should be judged whenever there is a complaint of weakness or incoordination or a need for an aid in subluxation analysis and in evaluating correction. Three techniques are used: (1) active patient motion against an examiner's resistance, (2) examiner resistance against active patient motion, and (3) mechanical resistance against active patient motion.
A large number of neuromuscular and musculoskeletal disorders show evidence of disturbed muscle tone such as weakness or spasm, but weakness is the predominating pattern found in muscle testing. This is often depicted as a compensatory hypertonicity in the antagonistic muscle. Both muscle testing and inspection may disclose a weakness without palpable or measurable atrophy. This type of relative muscle weakness in comparison to its antagonist is often associated with a palpable trigger point at the origin and/or insertion of affected muscles.
The development of tension against resistance is the most obvious property of muscle. The ability to develop tension and perform mechanical work is greatly influenced by the length of the muscle at the moment of action. The two most common means to measure such tension are the maximum tension readout on a tensiometer (strain gauge) and the amount of load (eg, manual resistance) that can be moved.
The customary criteria of grading muscle strength are shown in Table 9.10.
Grade Degree, Title Description
Grade 5 100% (Normal) Complete range of motion against
gravity with full resistance.
Grade 4 75% (Good) Complete range of motion against
gravity with some resistance.
Grade 3 50% (Fair) Complete range of motion against
gravity with no resistance.
Grade 2 25% (Poor) Complete range of motion with
gravity eliminated.
Grade 1 10% (Trace) Evidence of slight contractility,
but no joint motion.
Grade 0 0% (Zero) No evidence of contractility.
Physical Procedures
Astute gross observation, regional inspection, palpation, bilateral comparison, and correct positioning are essential before manual muscle testing is attempted to assure valid evaluation. When unilateral muscle weakness is suspected, it is always best to test the contralateral muscle first to compare resistance. Pressure against action should be applied in a direction that is opposite to the line of the tested muscle's pull and at the distal aspect of the segment on which it inserts.
The "break" point in muscle testing, when the patient can no longer meet the resistance, is undoubtedly the result of the Golgi tendon organ response. The loss of power is usually abrupt. This suggests that maximum strength depends a great deal on how efficiently an individual can cortically oppose the inhibition of his or her Golgi tendon organ reflex.
The examiner should strive to evaluate one muscle at a time, thus the patient should be requested not to recruit allied muscles during resistance. The testing of individual muscles rather than muscle groups is essential in neuromuscular diagnosis and to determine the neurologic level. It is less important in gross biomechanical evaluation. In either case, extreme caution should be used during resistance to avoid creating cramps, stretch injuries, or excessive fatigue of the patient.
The fault with manual methods is that evaluation rests a great deal upon the subjective skill of the examiner, and some patients are more willing to exert maximum effort than others. Care must be taken that the direction and amount of pressure are controlled and consistent.
The degree of strength can be determined only if pressure is applied gradually after the patient has "set" the muscle being tested against resistance. Also, the length of lever arms varies with patients and this affects relative strength, as does age, joint angle, bulk of body parts, and sex differences. Muscles often test differently in various positions such as from prone, supine, to weight bearing. It also is important that the same examiner conduct and record initial and follow-up evaluations of the degree of "resistance."
Stabilization. To obtain maximum contraction, one segment (usually the site of origin) must be stabilized manually if not by muscle tension, body weight, or gravity as a muscle exerts as much pull on its origin as it does its insertion. Poor stabilization results in erroneous conclusions.
Substitution. Possible substitution (eg, in dystrophy) and synergism must be eliminated by careful positioning and stabilization. If a muscle is called into action only in assistance when unusual force is necessary, it is called an emergency mover or an accessory muscle. When the action of a muscle is to prevent the action of undesired contraction of another muscle, it is called a neutralizing muscle. The action of emergency and neutralizing muscles must be carefully considered during clinical muscle testing to avoid erroneous conclusions. In addition, care must be taken that antagonistic muscles are relaxed.
Multiple Innervation. Another point to be considered is that several large muscles such as the pectoralis major, trapezius, deltoid, latissimus dorsi, triceps brachii, and the quadriceps femoris are so constructed and innervated that portions of each muscle may function separately as well as together. The actions of different muscle parts may be palpated during function or recorded with greater accuracy by electromyography.
Mechanical Procedures
The hand dynamometer and electromyograph are the typical objective clinical instruments available to record the force of muscular contraction. In recent years, several sophisticated pieces of equipment that provide objective data, and sometimes a printout, have been placed on the market.
The simple hand dynamometer gives the examiner four measurements: (1) strength of grip muscles, (2) fatigue rate of grip muscles, (3) recovery rate of these muscles, and (4) a bilateral comparison of the muscles of both hands. While initial readings are helpful in diagnosis, subsequent readings are helpful in determining the patient's rate of recovery. In dynamometry, three readings are usually taken on each hand in sequence to show strength, fatigue, and recovery rates.
Electrodiagnosis
The general term electrodiagnosis refers to the use of any electrical modality to test the integrity of muscles and nerves. As a common adjunct to the physical examination of the motor system, electrodiagnosis has become a valuable tool in evaluating whether partial degeneration of a motor unit should be suspected.
Electrodiagnostic tests (1) help to determine if disease of the upper or lower motor neuron is being dealt with, (2) help to determine if the nerve is interrupted, and (3) help to determine if the muscles are undergoing degeneration. Low voltage currents are used in the process, and the degree of reaction gives the practitioner an idea of the extent of disability present. Innervated muscles normally react to electrical stimulation; however, several situations exist where normal responses are not seen.
Nerve Conduction Analyses
Nerve conduction studies are helpful in confirming physical findings of a peripheral nerve disorder, in localizing the site of the lesion, and in assessing the severity of the lesion. Eisen/Hoirch report that there is a 70% 80% correlation among clinical, myelographic, and electrophysiologic findings in cases of spinal root lesions, but only one may be found to be abnormal. They feel that these findings therefore complement each other in the overall evaluation.
When an electrical stimulus is applied to a peripheral nerve, all large myelinated axons can be discharged simultaneously and the resulting action potential can be measured by an oscilloscope. When a stimulus of 20—100 volts is applied for 0.1 millisecond to a mixed peripheral nerve, the action potentials induced will travel in both directions along the nerve. Those impulses traveling centrally will be perceived as an electric shock, but those coursing peripherally can be recorded either in the muscles innervated or on the surface of the cutaneous sensory branches.
Basic Measurements. The amplitude of the induced potential spike is determined by the number of axons involved in transmitting the stimulus from the point of excitation to the recording site. The latent period of the potential is determined by the rate (conduction velocity) at which the largest nerve fibers transmit the action potential through the axons involved. Conduction velocity can thus be determined by dividing the distance traveled by the time taken from application to recording. This will vary depending on the diameter size and thickness of myelination of the fibers activated.
Nerve conduction studies are normal in pure upper motor neuron lesions. Some basic changes occurring in lower motor neuron lesions are briefly described below:
Generalized blocks. Widespread demyelinating disorders of the peripheral nervous system feature slowed conduction speeds, amplitude loss (especially distal in axonal dystrophies), or both.
Local axonal blocks. Localized peripheral nerve lesions are characterized by a conduction block or a slowed conduction velocity in the area of the lesion. The response evoked is smaller when applied proximally than when applied distally.
Axolemmal lesions. In axolemmal disorders, impulses are blocked about the lesion. A stimulus applied proximally to the lesion produces no response or one with an extremely reduced amplitude, but a stimulus applied distally to the lesion will produce a normal response.
Axoplasmic lesions. Axonal narrowing results in slowed conduction, axonal degeneration produces a low-amplitude or an absent response, and demyelinating diseases cause a slowed conduction velocity and a progressive loss of amplitude on more proximal stimulation.
Neuromuscular transmission blocks. In these disorders, there is a progressive loss of amplitude with repetitive stimulation at rates of only 2—5 per second.
Primary muscle disease. Atrophic states are characterized by low-amplitude spikes with normal conduction velocity rates.
Degeneration Reactions
If the conduction of galvanic or faradic current through a peripheral nerve has become impaired because of disease, trauma to the nerve trunks or anterior roots, or a lesion in the spinal cord, changes occur in the electrical reaction of the muscles innervated. Such reactive changes usually occur within 10 days after the initial insult, and they are known as the reaction of degeneration (RD). With RD, two responses may be seen: (1) no response to brief impulses of faradic tetanizing current; or (2) a sluggish response to galvanism.
Partial Degeneration. When a muscle is partially denervated or when some of the nerve fibers are normal and others are denervated, greater amounts of current are required to elicit a response. In partial RD: (1) the nerve shows a decrease of both tetanus and galvanic responses; and (2) the involved muscles show (a) decreased tetanic excitability, (b) increased galvanic excitability, (c) a slow response, but not as pronounced as in full RD, (d) polar response changes, and possibly, (e) a displacement of the motor point.
Complete Denervation. In full RD: (1) the nerve does not respond to either faradic (tetanic) or galvanic stimulation; (2) after about 10 days, the involved muscle tissue does not respond to faradic (tetanic) stimulation; (3) the muscle will respond to galvanic stimuli with a sluggish response but only when greater current intensity is applied; (4) the motor point is displaced toward the periphery where the fibers of the muscle attach to the tendon, and (5) the formula for polar response may change. In full RD, there is absolutely no response to any current in either the nerve or the muscle. Thus, these signs exhibit the final stage of full RD. See Table 9.11. If reinnervation does not occur, destruction of the fibers will eventually take place.
Status Tissue Galvanic Stimulation Tetanizing Faradic
Normal reaction Muscle Brisk single contraction Tetanic contraction
Nerve Brisk single contraction Tetanic contraction
Partial reaction Muscle Sluggish contraction Diminished response
of degeneration Nerve Diminished response Diminished response
Full reaction of Muscle Sluggish response No response
degeneration Nerve No response No response
Complete reaction Muscle No response No response
of degeneration Nerve No response No response
_____________________________
*From Jaskoviak/Schafer: Applied Physiotherapy, ed 1.
Stages of Degeneration. Three distinct stages are found in the course of RD:
First stage: 10 days to 2 weeks. After the first week, the nerve loses all response to tetanic stimulation. If the muscle responds at all to tetanic current, it is quite feeble. Galvanic testing elicits only a slow, weak contraction in the muscle(s) involved, rather than the normal brisk contractions. The cathode-closing contraction is greater than the anodal closing contraction the reverse of the normal response.
Second stage: the stage of full RD, which lasts from a few weeks to 1 year or more.
Final stage: In this stage, there is either a gradual return of voluntary function with an electrical response or an absolute irreversible RD develops.
Miscellaneous Electrical Muscle Testing Procedures
In cases of peripheral nerve injuries, electrotherapy is indicated to maintain muscle tone and to prevent muscle atrophy. In such cases, electrical muscle testing should become an integral part of therapy to evaluate progress. Accordingly, muscle stimulators should provide features to conduct the following tests along with their therapeutic modes.
Accommodation Test. According to the established principles of electrophysiology, neuromuscular units can accommodate to a gradually increasing current (ie, an exponentially progressive current) Totally denervated muscles lose this ability, and this fact permits a simple but reliable test for establishing the degree of denervation.
Faradic Excitability Test. Innervated neuromuscular units should respond by contraction when currents of short duration (eg, 1 ms) are applied. For this test, a simple sine wave would do, but variable frequency generators allow for more precise evaluation.
Galvanic Excitability (Rheobase) Test. In this test where direct current pulses of long duration are used (eg, 500—1000 ms or interrupted dc), the actual amount of current strength (measured in milliamperage) necessary to contract a muscle is measured. Variable frequency generators permit the application of true square wave current and a more precise measurement, but simpler units also can be used for this test.
Chronaxie Test. This test requires a variable frequency generator that incorporates precise timing and current intensity measurements. The chronaxie determines the impulse time necessary for a muscle to contract with double the current strength of the rheobase. Most healthy neuromuscular units have a chronaxie of 1 ms or less.
Strength Duration Curves. This test can be performed with a variable frequency generator, measuring the current intensity in milliamperage, at different impulse settings; eg, 1000 ms (rheobase), 500 ms, 250 ms, 100 ms, 50 ms, 25 ms, 5 ms, 1 ms, 0.1 ms, and 0.05 ms. These measurements can be plotted graphically and provide detailed objective data about the excitability of any selected neuromuscular unit. The chronaxie is obtained from this test graphically. With experience, according to Wolf, a physician or therapist can perform the test in less than 5 minutes, particularly when it is used with subsequent treatments.
Because the techniques are similar, nerve conduction studies are usually made at the same time as electromyographic studies.
Electromyography
Electromyography is the study of the electrical impulses arising from muscles during muscle activity. It is based on the fact that a relaxed muscle has no obvious electrical activity, while an active muscle has an action potential that can be measured by electrodes placed within or on the skin over a muscle. The latter is the usual practice. When the electrodes are connected to an oscilloscope, action potentials of muscles and specific parts of muscles may be viewed and tracing can be made.
Rationale
Electromyography (EMG) allows the recording of oscillations in potential variations of skeletal muscles at rest and during activity. It offers a tracing of electrical activity transmitted from muscle to an electrode and then to an oscilloscope. This process allows study of the potential of muscle at rest, the reaction of muscle to contraction, and the response of muscle to external stimulation. Such tracings aid in determining whether a patient's illness is directly affecting the spinal cord, muscles, or peripheral nerves.
Surface electrodes are most frequently used to record myopotentials, but needle electrodes allow the recording of potentials of individual muscle fibers. Surface EMG yields data concerning muscle action or rest but fails to give data about individual fiber potentials.
The purpose of EMG recordings can be placed in several broad categories. EMG is frequently used to evaluate the amount of muscle activity occurring in specific muscles, and it can be used to study kinesiologic function of muscle. The general rule is that there will be less EMG activity in eccentric contractions as compared to concentric contractions.
EMGs can be used in pathologies to determine the nature, scope, and prognosis of diseases involving neuromuscular function. They can be used to differentiate between neurogenic and myogenic paralysis and differentiate between organic paralysis and psychogenic reactions. Thus, if muscle weakness is exhibited, an EMG will determine whether the loss of power is caused by a deficit in impulse transmission (eg, myasthenia), myopathy, or neuropathy.
The procedure is valuable in determining the affected level of spinal roots, localizing a disorder within the peripheral motor neuron, and differentiating between lesions of the 1st and 2nd neurons. It has also been shown to be effective in differentiating between pyramidal and extrapyramidal hypertonicity, in the analysis of tremor, in assessing myotonic and myasthenic disorders, in evaluating the success of therapy, and in arriving at a prognosis in traumatic and neuritic lesions.
Procedure
The patient should be positioned in a relaxed position while the selected peripheral nerves are stimulated. The electrical activity in muscles and nerves is then recorded. When muscle is at rest, there is normally no electrical activity observed. When muscles are active, the EMG shows a wave-like graph representation of each contraction. Graph lines are amplified with the increase in strength of each contraction.
Muscle disease produces a spiked wave pattern, with the shape of the spike often being characteristic of a specific disease. A diminished wave suggests muscle weakness. Waves disappear after a few minutes in myasthenia gravis. Nerve involvement, as opposed to muscle involvement, usually shows a decreased frequency of contractions.
In its common application, EMG provides objective evidence of partial muscle denervation. When test results are positive, it is believed to be of considerable importance in the accurate diagnosis of a herniated IVD. The test will not be positive within 4 days of the onset of root pathology. Thus, tests are helpful in the evaluation of a complex clinical picture in which evidence of radiculopathy is inconsistent or confusing. Abnormal EMG findings can be crucial in the evaluation and management of a patient when compensation, litigation, and psychiatric problems are involved.
The use of EMG recordings helps to establish the scientific basis for both diagnostic conclusions and to monitor the effectiveness of therapy. Spector feels that surface electromyography is one of the best means to assess the reliability of innovative as well as standard methods in the management of musculoskeletal disorders, thus decreasing the possibility of misdiagnosis and/or improper treatment. Accurate analysis, however, is complex and requires special instruction because recordings from different muscles are influenced by electrode configuration, orientation of muscle fibers, the amount of subcutaneous tissue beneath the electrode, and other factors.
Electromyography in Scoliosis
According to a study by Zetterberg and associates, a comparatively higher EMG signal amplitude has been found on the convex side of a scoliosis. This was due to a lower amplitude on the concave side when the scoliosis group was compared to a control group. The amplitude difference was correlated to the degree of scoliosis. A shift in the myoelectric spectrum toward the lower frequencies occurred during loading. There were no differences in this respect between the sides of the scoliosis nor were there differences between the scoliotic patients and the controls. It was concluded that secondary adaptation to the higher load demand by the muscles on the convex side in scoliosis appeared to explain the findings.
A study by Reuber and associates also suggested that the asymmetries in muscle actions shown by myoelectric measurements were the result of scoliosis. According to these investigators, scoliosis progression does not appear to be caused by asymmetry in muscle contractions; rather, it may be caused by a lack of adequate asymmetry.
Electromyographic Studies Following Adjustive Therapy
Widmann defined the advantages of EMG studies in chiropractic research in 1961, but it has only been within the last decade that his advice has been taken seriously. The findings of a few studies are described below.
In EMG studies of the effects of spinal adjustments on symptomatic patients, Grice found that there was a strong tendency toward decreased action potentials (both in frequency and amplitude) and more symmetry in both static and dynamic muscle potentials as compared with preadjustment imbalances.
In Thabe's EMG studies of the upper cervical and sacroiliac joints, it was found that manual mobilization techniques have a greater effect in reducing spontaneous segmental muscle activity than if afferent information from a restricted joint is blocked with a local anesthetic.
Hibbard found that significant EMG amplitude changes occurred in the activity of gait muscles following manipulation of the lower extremity articulations to reduce malposition, while the electrical activity of control subjects decreased only slightly.
Rebechini-Zasadny and associates found that 12 out of 12 subjects showed increased muscle activity following manipulation of the cervical spine and 9 out 12 subjects showed increased muscle strength.
It was thought for many years that much of the pain in spinal syndromes was due to paravertebral muscle spasm. Recent studies have not confirmed this. For example, Roland points out that EMG studies show increased muscle activity in back-pain patients, but the degree of activity is probably insufficient to produce pain. Current literature tends to view the spasm associated with back pain as a secondary factor in most instances; ie, most back pains originate from the nociceptors of the involved joints.
Evaluating the Cerebellar System
Earlier chapters have described how the lateral lobes of the cerebellum are chiefly concerned with the smooth coordination of striated muscle activity, while the central lobe maintains and controls posture, balance, and a smooth gait. The etiology of myokinetic malcoordination can be found in the sensory receptors, the peripheral nerves, the spinal cord, the brain stem, the cerebral cortex and subcortex, or the cerebellum.
It should be noted that there can be no proprioceptive tract defect, no loss in muscle tone, no muscle weakness, or no gross structural abnormality if coordination and balance are to be properly maintained. Thus, these factors must be eliminated before a disorder can be attributed to the cerebellum itself.
The term myokinetic coordination refers to a patient's ability to integrate separate motor abilities into a complex task. Well-coordinated movement, usually involving the large muscles, requires perfect timing between the nervous and muscular systems. Once the cerebral cortex receives an afferent impulse and decides what task must be performed in response, the cerebellum coordinates the reaction so that the act will be carried out smoothly. Thus, once a lower motor neuron lesion has been ruled out, cerebellar function should be evaluated.
Symptomatology
The primary motor signs of a cerebellar lesion are tremor, nystagmus, ataxia, decomposition of movement, dysmetria, dysdiadochokinesia or adiadochokinesia, scanning speech, asthenia, and hypotonia (Table 9.12). Other signs include vertigo, cerebellar fits presenting a rigid convulsion, and vocal dysarthria characterized by an explosive, slurred speech that is peculiar to cerebellar lesions. Any sign of skew deviation of the eyes should be noted; viz, one eyeball deviated up and outward and the other turned down and inward (brachium pontis lesion). Spooning of the hands (hyperextension of opened palms) is also occasionally seen in cerebellar disease.
Location Primary Suspect Disorders
Anterior horn Progressive spinal-mus- Syringomyelia
cular atrophy Poliomyelitis1
Cerebellar disease Oliopontocerebellar dis- Spinocerebellar diseases
eases Cerebellar ataxia
Muscle Various myopathies
Peripheral nerve Nerve compression Various neuropathies
Proprioception loss Pernicious anemia Tabes dorsalis
Type Primary Suspect Disorders
Permanent hypotonia Peripheral defect CNS defect
Anterior horn lesion Cerebellar ataxia
Myasthenic states Cerebellar degeneration
Myopathy Parietal lobe disease
Myositis (advanced) Tabes dorsalis
Peripheral nerve lesion
Temporary hypotonia Cerebral palsy Drugs
Brain anoxia Anticonvulsants
Kernicterus Muscle relaxants
Narcotics
Degenerative diseases Soporifics
Aminoacidopathy Tranquilizers
Cerebrohepatorenal
syndrome Spinal diaschisis (spinal
shock)
Infantile neuroaxonal Anoxia
dystrophy Brain or cord trauma
Krabbe's disease Hemorrhage
Lipid storage disease Infarct
Metachromatic leukodys- Sepsis
trophy
In time, cerebellar defects are compensated for to a considerable degree by other brain mechanisms. Thus, symptoms are less severe in slowly progressing diseases than those of acute cerebellar disorders.
It should be kept in mind that the left side of the body is under the influence of the left cerebellar hemisphere, and vice versa. Any symptoms that occur unilaterally will then be on the same side as the cerebellar lesion. The opposite is true with cerebral lesions, where the lesion invariably produces contralateral symptoms.
Testing Procedures
General cerebellar function is tested by the evaluation of gait, carriage, and Romberg's station test. Upper extremity coordination is evaluated by the finger-to-nose test, palm pronation and supination, hand patting, and arm extension tests. Lower extremity coordination is judged by gait, heel-to-knee, heel-to-toe, and foot-to-buttock tests.
Upper Extremity Coordination Tests
Finger-to-Nose Tests. If the patient is lying, the patient's arms should be outstretched at the sides; if sitting, the patient's hands should rest on the knees; if standing, the patient's arms should be relaxed at the sides. Direct the patient to touch the tip of the nose with the tip of the forefinger (finger-to-nose test), first with the eyes opened, then closed. Note the line between the starting point and the nose to determine if it is straight, curved, or if there is a jerking, irregular motion. Observe whether the finger becomes coarsely tremulous as the nose is touched (intention tremor). If a tremor is present, it indicates a proprioceptive (sensory) defect when the defect is noted primarily when the eyes are closed. Note if the finger goes beyond the nose (hypermetria), or fails to reach the nose (hypometria). The term dysmetria is used to denote if the finger goes beyond the nose or fails to reach it. The action should be smooth, rapid, and the arms should remain in the same plane. Note whether there is a difference when the eyes are closed or if the same degree of incoordination is present with them open. If there is a defect, it is technically called dysdiadokinesis and is a part of cerebellar dyssynergia. Failure to perform these tests suggests a lesion of the posterior columns or polyneuritis.
Finger-to-Finger Tests. This is just a variation of the finger-to-nose tests.
Palm Pronation and Supination Tests. The patient should be asked to extend the arms forward on a level with the shoulder and then separate the fingers. Any sign of tremor should be noted. Next, have the patient rapidly pronate and supinate the palms. When the patient is sitting, the patient's hands are first placed on the lower thighs. In these tests, note faulty movements such as (1) tendency to wide movements at the elbow or (2) incomplete supination and pronation. Again, the action should be smooth, rapid, and the arms should remain in the same plane. The presence of changes denotes dyssynergia. The term adiadokinesia refers to the inability to perform rapid alternating movements. Barognosis means the ability to sense the weight of objects.
Hand Patting Test. In this test, the patient rapidly pats the examiner's hand. Both sides should be checked. This is another method to check for dyssynergia.
Arm Extension Tests. The patient is placed in the erect position with the eyes closed and the arms are extended straight forward with hands parallel and held there actively for 20 30 seconds. The patient's arms are then extended straight up over the patient's head with the palms facing forward and held there actively for 20—30 seconds. It should be noted if there is any drooping of an arm or for a tendency of an arm and hand to flex and rotate internally because this is one of the earliest signs of paresis of the CNS. A drift of the upper extremity down and out suggests a cerebellar disorder. Senile and familial tremors appear most marked in outstretched hands. They disappear at rest and are aggravated by stress.
Holmes' Rebound Phenomenon. A positive sign is noted when the patient flexes his arm against the resistance of the examiner, and when the arm is suddenly released, it strikes the patient's chest. This is a significant finding in ipsilateral cerebellar disease.
Trunk and Lower Extremity Coordination Tests
Coordination of the trunk is judged in relation to carriage, gait, and station, and coordination in the lower extremities is evaluated by the heel-to-knee, heel-to-toe, and foot-to-buttock tests.
Gait. The stability of the trunk is mediated by the cerebellum, and abnormality is reflected by ataxia whether the patient's eyes are open or not. In screening, the patient is asked to walk a straight line at a normal rate with the eyes opened and then closed. The width of base, unsteadiness in any direction, or tendency to go to one side or the other (dyssynergia) should be noted. If the foot drags (spasticity) or flaps down flatly (ataxia), or if the toes are raised with the heel (foot drop), these signs should be recorded.
The patient should then be asked to walk and turn to the right, then to the left, to walk backward, and also to walk on the toes and then on the heels. The examiner should observe the patient's feet, legs, trunk, arms, and shoulders for deviations from the normal gait. Loss of arm swing may indicate basal nucleus disease while exaggeration of arm movements occurs in athetosis. All deviations from the norm should be recorded.
Normal gait features smoothness and ease with little attention required by the patient. The pelvis is fixed and the lower limb is carried straight forward with knee flexion, with the opposite limb swinging forward in harmony. An abnormal gait because of pain may be the result of some form of peripheral neuropathy or irritative radiculopathy. It is characterized by a gingerly walk with slow, short steps. If the pain is unilateral, weight will be thrown to the unaffected side. Besides local and cerebellar causes, gait disturbances can also be reflections of a basal ganglia, subthalamic nuclei, posterior column, or trunk muscle lesion.
Romberg's Station Test. The patient should be requested to stand erect with the heels and toes together (Romberg position) and look straight ahead. Then the patient is asked to close the eyes. Note the presence of any swaying of the body in any direction more than is ordinarily seen. Swaying with the eyes open or closed indicates either dyssynergia or ataxia of the legs or trunk, or of both, depending upon the presence or absence of sensory disturbances. The examiner must be alert to catch the patient if he begins to fall. Although this test may be positive in a normal subject and those with nonneurologic diseases, it is highly indicative of a lesion interrupting the proprioceptive pathways between the lower limbs and the cerebellum.
Heel-to-Knee and Heel-to-Shin Tests. With the patient in the supine position, request that the knee be touched with the heel of the opposite foot. Compare the two sides, and note any curve in the line or irregular movement. Note hypermetria or hypometria. Then have the patient touch the shin with the heel of the opposite foot and make bilateral comparison. Have the tests performed with the eyes opened and closed, noting the same characteristics as in the upper extremities. In cerebellar lesions, the patient will overhit or underhit the mark, and then finally get there.
Also observe for a last-minute intention tremor. The patient also may have difficulty from a proprioceptive loss, but this would indicate a defect due to loss of joint sensation rather than a loss of cerebellar coordination. Many examiners also find it advisable to perform these tests with the patient in the standing position.
Foot-to-Buttock Test. The patient should be asked to flex the thigh and leg, bringing the foot up near the buttock and resting it on the examining table. Note any swaying of the knee from side to side (dyssynergia). Again, many examiners also perform this test with the patient standing.
Evaluating Cranial Nerve Motor Fibers
The Oculomotor System (Cranial III, IV, VI)
Functional defects of cranial nerves III, IV, or VI are frequent but seldom persistent. Lesions of these nerves are commonly noted with various types of strabismus (squint) and pupil dysfunction. Failure to move the eye voluntarily in any given direction indicates muscular incompetence caused by primary muscle disease or a neurogenic factor.
Because of their proximity, cranial nerves III, IV, and VI are usually tested together by examining the eyelids, pupillary changes, and extraocular movements. Each eye should be tested separately and then together.
The Eyelids. It should be noted whether the eyelids droop. Compare the amount of cornea covered by each lid. Ask the patient to look upward. If ptosis exists, the affected lid cannot be raised except by compensatory action of the frontalis muscle, which produces a wrinkling of the forehead on the same side.
The Pupils. Seek abnormal pupil signs such as of size (miosis, mydriasis, anisocoria), shape (irregularity of margins), position (ectopia), or reactions to light and in accommodation. Place the patient in a position where strong light does not enter the eye; and with a penlight, test each eye separately. Note whether the pupil contracts readily or slowly, whether there is irregularity in the outline of the pupil or any inequality of the pupils. The light reflex results in normal constriction of the pupil when light is flashed into the eye. This is a direct reflex to light. The consensual reflex is tested by flashing light in one eye and noting if the opposite pupil contracts. This is a similar but weaker reaction than with the direct light reflex.
Adie's pupil is a benign disorder featuring a very weak light reflex that is delayed for several seconds, and often confused with an Argyll Robertson pupil. Adie's pupil is larger than normal, reacts slowly to light, and often found in young women with decreased or absent tendon reflexes. An Argyll Robertson pupil is an abnormally small pupil that fails to respond to the light reflex but does constrict with accommodation and convergence a well-established sign of CNS syphilis.
When the eyes are directed to a point close at hand, three different reflexes are brought into cooperative action: (1) convergence, (2) accommodation, and (3) pupillary constriction. All three reactions may be initiated by voluntarily looking at a near object, but an involuntary (reflex) mechanism will accomplish the same end if an object is moved slowly toward the eyes.
Convergence. In this test, the examiner moves a finger or some other object held some distance away toward the patient's eyes, midway between them. The eyes should move inward, and the pupils should contract. The medial recti muscles contract to move the eyes into alignment so that images in each eye focus on the same part of the retina to avoid diplopia. An inability to converge the eyes commonly occurs in encephalitis and vascular diseases of the midbrain.
Accommodation. To test accommodation, the examiner asks the patient to face the light, look at some object about 2 feet or less from the eyes, and then look off at a distant object. When looking at a near object, accommodation should accompany convergence and pupil constriction. During accommodation, the lenses are thickened as a result of tension by the ciliary muscles to maintain a sharply focused image.
Pupillary Constriction. Along with convergence and accommodation, the pupils should contract on looking at a near object. The pupils narrow as an optical aid to regulate the depth of focus. This type of near-object pupil constriction does not depend on any change in illumination and is separate from the direct and consensual light reflexes.
Extraocular Movements
Extraocular neuromuscular integrity is tested by having the patient follow the examiner's finger in all directions.
Any difficulty in doing so indicates a weakness of the corresponding muscles (Table 9.13).
Diplopia Direction Nerve Muscle Deviation of Eyeball when looking: of image III Inf. oblique Downward and outward Upward and inward Oblique III Inf. rectus Upward and inward Downward and outward Oblique IV Lat. rectus Inward (internal squint) Toward the temple Vertical III Med. rectus Outward (external squint) Toward the nose Vertical IV Sup. oblique Upward and outward Downward and inward Oblique III Sup. rectus Downward and inward Upward and outward Oblique
Note the presence or absence of nystagmus. Impairment of conjugate eye movements indicates a lesion in the midbrain. Certain tests are specific:
The oculomotor nerve supplies all muscles that move the eye except the superior oblique and rectus lateralis. It also supplies the sphincter pupillae and ciliaris muscles. Thus, it is tested by eye movements, particularly medially upward and downward, and by pupillary response to light and accommodation. Lesions of this nerve result in a ptosis of the upper lid and dilation of the pupil with loss of the light reflex.
The trochlear nerve supplies only the superior oblique muscle of the eye. Thus, it is tested for eye movement downward and inward.
The abducens nerve supplies only the rectus lateralis muscle of the eye. Thus, it is tested by the ability to move the eye laterally.
The Visual-Fixation Reflex. This reflex is demonstrated by an auto passenger looking out a side window at the passing scenery. The head and eyes turn slowly in the direction of apparent movement and then jump ahead quickly to fix the gaze on a new approaching site. This is done without conscious effort or awareness that the eyes are moving: a true optokinetic reflex. This reflex is also demonstrated and tested as in reading from line to line, which normally exhibits a combination of jerky eye movements interspaced with pauses.
Diplopia. Double vision occurs when the conjugate movements of the eyes are altered so that images do not fall on corresponding areas of the two retinae.
The result is that the brain interprets two images that are not exactly superimposed. If only one eye is affected, it will usually show a motion abnormality in the field of the involved muscle.
Trigeminal Nerve (Cranial V Motor Fibers)
The trigeminal nerve (cranial V) is the great sensory nerve to the face and anterior scalp. It is also the motor nerve to the muscles of mastication (except the buccinator). The motor division of the trigeminus runs only with the mandibular branch of the sensory division. Thus, weak jaw movements (eg, chewing) are likely to be associated with sensory changes in the chin, lower lip, cheek, upper ear, and lateral scalp.
Motor Function Tests. Motor function of the trigeminal is tested by the examiner placing the hands over the masseter and temporal muscles and asking the patient to make chewing motions with the jaw. Note if the muscles contract unequally. The pterygoids are tested by having the patient open the mouth widely and then close it. Note whether the jaw deviates to one side or the other during this motion. Palpate the masseter and temporalis muscles when the patient is asked to "bite down" on a tongue blade on each side. Jaw strength is tested by trying to extract the blade against the patient's resistance. The motor portion of the trigeminal is commonly impaired in cerebral vascular accidents, basal meningitis, syphilis, and brain tumors. These severe disorders are rarely difficult to differentiate from TMJ dysfunction.
Facial Nerve (Cranial VII Motor Fibers)
There are two components of this nerve: one that carries the motor division and another (the intermediate nerve of Wrisberg) that conveys the sensory and autonomic fibers. The parasympathetic fibers via the pterygopalatine and submandibular ganglions supply the lacrimal glands, the mucosa of the nasal cavity and roof of the mouth, and the sublingual and submandibular glands.
Motor Function Tests. The patient should be asked to raise the eyebrows and wrinkle the forehead, to frown, to close both eyes tightly, and then to close each eye separately. The patient is then asked to show the teeth, open the mouth widely, retract the lips, whistle, and smile. The inability to perform such upper and lower facial muscle tests usually indicates a weakness or paralysis of the nerve.
All facial movements should be equal bilaterally, but some patients habitually talk, smile, and chew more on one side than the other. Weakness of the muscles supplied by the facial nerve may be expressed as drooping of the corner of the mouth, smoothing out of the nasolabial fold, drooping of the lower lid, or inability to close the involved eye such as seen in Bell's palsy where the signs are unilateral. If the frontalis muscle is involved, the forehead is unusually smooth on the affected side. Note the presence or absence of atrophy, abnormal movements, contractures, etc.
In upper motor lesions affecting the face, involuntary movements such as blinking and smiling are far less affected than voluntary movements. The muscles of the forehead are spared in upper motor lesions affecting the face. This latter sign occurs because the muscles of the forehead have bilateral cortical representation. In contrast, all facial muscles are affected in lower motor neuron lesions. Thus, they exhibit paralysis of both voluntary and involuntary muscle groups.
Jaw Jerk. The jaw reflex is manifested by a rapid closure of the mouth that is caused by a downward blow on the lower jaw while it hangs passively open. It is rarely normal and usually considered a pathologic sign (eg, sclerosis of the lateral columns of the cord).
Chvostek's Test. In hypocalcemia, the irritability of the facial nerve is greatly increased and tested by Chvostek's reflex. A positive Chvostek's sign is a frequent but not pathognomonic sign of tetany and sometimes witnessed in tuberculosis. It is positive when tapping the facial nerve along its course (eg, over the parotid gland) induces contraction of muscles on the ipsilateral side of the face.
Glossopharyngeal and Vagus Nerves (Cranial IX and X Motor Fibers)
The glossopharyngeal nerve is the sensory nerve to the region of the isthmus faucium and posterior one-third of the tongue and pharynx. It is the motor nerve to the stylopharyngeus muscle and parasympathetic to the parotid gland. Thus, it is tested by the gag reflex (sensory, glossopharyngeal; motor, vagus) and taste sense of the posterior tongue. This nerve may be impaired in skull fractures and diseases affecting the brain stem such as in tumors, syphilis, and tuberculosis. Dysphagia and tachycardia may be associated. An occipital injury may tear through the posterior foramen and paralyze the glossopharyngeal, vagus, and accessory cranial nerves. Multiple cranial nerve signs are also seen in brain stem syndromes.
The vagus nerve is motor to the pharynx, uvula, larynx, and upper part of esophagus. It is sensory to the pharynx, larynx, and upper esophagus; and parasympathetic to the thoracic and upper abdominal viscera. Numerous viscerovisceral and viscerosomatic reflexes course through the vagus nerve. Upper vagal motor integrity is screened by the responses to the gag reflex, the pharyngeal reflex, and movements of the pharyngeal and laryngeal muscles during speech and swallowing.
Nasal speech may be the result of palatal paralysis or paralysis of the vocal cords. Weakness of the oropharynx is suggested by a soft breathy voice associated with nasal escape, while a lesion of the nerve supply to the upper larynx is suggested by a hoarse or husky voice.
Impairment of the vagus nerve may result from diphtheritic paralysis of the pharyngeal branch, injury to the recurrent laryngeal branch by surgery, cervical and mediastinal tumors, aortic aneurysms, or pressure on the nerve from a hypertrophied left atrium. The vagus also can become involved in infectious neuritis, multiple sclerosis, Guillain-Barr syndrome, amyotrophic lateral sclerosis, and bulbar poliomyelitis. In addition, the vagus is sometimes susceptible to trauma because of its long course and its proximity to several important organs. When direct vagal injury is seen, it is usually from damage to the recurrent laryngeal branch following neck trauma.
Motor Function Tests. The glossopharyngeal and vagus nerves are usually considered together as their functions during testing cannot be easily distinguished:
The patient is asked to open the mouth and say "Ah." The palate will normally rise in the midline. The raphe of the palate is observed and usually deviated to the nonparalyzed side; ie, unilateral palatal weakness will cause the uvula to move toward the intact side. The pharyngeal reflex refers to stimulation of the palate, fauces, or posterior pharyngeal wall that results in swallowing. Raising of the uvula (the uvular reflex) in phonation or from irritation is absent in disorders of the IX or X cranial nerves. It is important to make this test with the patient's head in the midline and not turned to the side.
The ability to swallow solids and liquids should be tested. If regurgitation occurs through the nose, its occurrence should be noted.
Spinal Accessory Nerve (Cranial XI)
The spinal accessory nerve provides motor innervation to the sternocleidomastoideus muscles and the upper half of the trapezius muscles. Injury to the spinal accessory nerve may result from subluxation complexes, trauma, IVD lesions, spasmotic torticollis, medulla and cervical cord lesions, and neck tumors and abscesses. Less frequently, multiple sclerosis, certain types of epilepsy, poliomyelitis, amyotrophic lateral sclerosis, and spinal cord tumors and involved. However, singular involvement of this nerve is rare; spinal accessory nerve dysfunction is usually associated with combined disorders of cranial nerves IX, X, and XII.
Motor Function Tests. The patient is asked to elevate the shoulders against resistance and then to lower the shoulders and thrust the shoulders backward against resistance to test the strength of the trapezius muscles. The patient is then asked to rotate the head from side to side against resistance to test the strength of the sternocleidomastoideus muscles. Note the presence or absence of atrophy, fibrillations, or spasms about the trapezius and sternocleidomastoideus. Strength can be screened bilaterally by having the patient flex the head while the examiner applies resistance to the patient's chin. The strength of the trapezius and sternocleidomastoids should be equal bilaterally unless a unilateral occupation is involved. The strength of lateral flexion against resistance is a helpful indicator. Marked bilateral weakness and atrophy of these muscles are often seen in primary muscle disease (eg, muscular dystrophy).
Hypoglossal Nerve (Cranial XII)
The hypoglossal nerve is the motor nerve to muscles of the tongue. The major signs of a cranial XII lesion are deviation of the tongue and difficult speech. Differentiation should be made from involvement of the carotid artery above its bifurcation or an injury to the recurrent nerve of the high vagus. Positive signs of hypoglossal dysfunction point toward skull fracture, aneurysm of the circle of Willis, and sometimes cervical subluxation. Hemiatrophy of the tongue and fibrillations are seen in bulbar palsy, syringomyelia, and not rarely in poliomyelitis. Coarse tremors are featured in Parkinson's disease and paresis. Fine tremors suggest alcoholism, bromide poisoning, senility, and idiopathic functional disorders. Injury to the hypoglossal nerve is not infrequently seen from fracture.
When inspecting the tongue, seek signs of atrophy, tremors (an early sign of lower motor neuron disease), wormy fasciculations (amyotrophic lateral sclerosis), and deviation (paralysis). Palpate the tongue if atrophy is seen. Ipsilateral atrophy and fasciculations are characteristic of a unilateral lower motor neuron lesion.
Evaluation of Motor Integrity. The patient is asked to protrude the tongue and rapidly move it from side to side. Rapid movement will be impaired in upper motor neuron lesions. The relaxed tongue will always deviate toward the side of paralysis in lower motor lesions. In bilateral involvement, the tongue may be protruded very slowly or not at all. In central lesions of the nerve, the tongue will be paralyzed on the contralateral side. It will be paralyzed on the homolateral side in peripheral lesions. The strength of the tongue may be estimated by having the patient press the tongue against the inside of the cheek.
Speech Test. Vocal articulation is a complex coordinated function involving the cooperation of muscles supplied by cranial nerves V, VII, IX, and XII. Note whether the patient's speech is clear, distinct, slurring, scanning, or tremulous. Use test phrases such as "truly rural" or "Methodist Episcopal." Keep in mind that a vocal dysarthria must be differentiated from an aphasia.
American Orthopaedic Association: Manual of Orthopaedic Surgery. Chicago, American Orthopaedic Association, 1972, pp 27-38.
Arbuckle BE: Reflexes. Journal of the American Osteopathic Association, 46(7), July 12, 1946.
Balduc HA: Overview of contemporary chiropractic science for the Chiropractic Association of Oklahoma. Northwestern College of Chiropractic, Convention notes, April 24, 1983.
Beardall AG: Additional gait tests. Digest of Chiropractic Economics, 19(5), March/April 1977.
Berthold CH: Morphology of normal peripheral axons. In Waxman SG (ed): Physiology and Pathobiology of Axons. New York, Raven Press, 1978.
Blacker HM: Evaluating sensory and motor systems. Patient Care, 17(16):121-136, 1983.
Brown JR: Diseases of the cerebellum. In Baker AB, Baker LH (eds): Clinical Neurology. New York, Harper & Row, 1975, Vol 2, Chapter 29.
Brown T, et al: Psychological factors in low back pain. New England Journal of Medicine, 25:4-22, 1954.
Bullock TH: The neuron doctrine and electrophysiology. Science, 129:17, 1959.
Burnside JW: Adams' Physical Diagnosis. Baltimore, Williams & Wilkins, 1974, pp 200-214.
Cabot RC: Physical Diagnosis, ed 7. New York, William Wood, 1919, pp 481-484.
Cailliet R: Disuse syndrome: fibrositic and degenerative changes. In Brena SF, Chapman SL (eds): Management of Patients with Chronic Pain. New York, Spectrum Publications, 1983, pp 63-71.
Calbe DB, Eisler T: The pathogenesis and medical treatment of extrapyramidal disease. Medical Clinics of North America, 63:715-727, 1979.
Canadian Memorial Chiropractic College: Segmental Neuropathy. Toronto, Canadian Memorial Chiropractic College, date of publication not shown, p 29.
Cerny K: Pathomechanics of stance: clinical concepts for analysis. Physical Therapy, 64:1851-1859, 1984.
Chusid JG: Correlative Neuroanatomy & Functional Neurology, ed 19. Los Altos, CA, Lange Medical, 1985, pp 117-119, 190-199, 205-215, 240, 269-278, 448-460.
Clark RG: Manter and Gatz's Essentials of Clinical Neuroanatomy and Neurophysiology, ed 5. Philadelphia, F.A. Davis, 1975, pp 16-23, 31-34, 40-42, 97-103, 127-133, 160-166
Coers C, Woolf AL: Innervation of Muscle. Springfield, IL, Charles C. Thomas, 1959.
Coote JH, et al: Reflex discharges into thoracic white rami elicited by somatic and visceral afferent excitation. Journal of Physiology, 202:141-159, 1969.
Cyriax J: Textbook of Orthopaedic Medicine: Vol One, Diagnosis of Soft Tissue Lesions, ed 8. London, Bailliere Tindall, 1982, pp 36-53, 453-466.
Daniels L, Worthingham C: Muscle Testing: Techniques of Manual Examination, ed 4. Philadelphia, W.B. Saunders, 1980, pp 167-177.
Daube JR, Sandok BA: Medical Neurosciences. Boston, Little, Brown, 1978, pp 168, 188-191, 221-222, 287-292, 354-357, 370-371.
Davis L: Neurological Surgery, ed 2. Philadelphia, Lea & Febiger, 1942.
Davis NJ, Kovac MP: The command neuron and the organization of movement. TINS, 4(3):73-76, 1981.
Debrunner HU: Orthopaedic Diagnosis, rev. ed 2. Translated by G Stiasny. Chicago, Year Book Medical, 1982, pp 33-52.
Dee R: Articular neurology. In Sokoloff L (ed): The Joints and Synovial Fluid. New York, Academic Press, 1978, p 177.
de Reuck AVS, Knight J (eds): Myotactic, Kinesthetic, and Vestibular Mechanisms. Ciba Foundation Symposium. Boston, Little, Brown, 1967.
Ducroquet R, Ducroquet J, Ducroquet P: Walking and Limping: A Study of Normal and Pathological Walking. Philadelphia, J.B. Lippincott, 1968.
Eisen A, Hoirch M: The electrodiagnostic evaluation of spinal root lesions. Spine, 8(1):98-106, 1983.
Elias SB, Appel SH: Current concepts of pathogenesis and treatment of myasthenia gravis. Medical Clinics of North America, 63:745-757, 1979.
Fowler WM Jr, Taylor RG: Differential diagnosis of muscle disease. In D'Ambrosia RD: Musculoskeletal Disorders: Regional Examination and Differential Diagnosis. Philadelphia, J.B. Lippincott, 1977, pp 93-95.
Friedman HH: Problem-Oriented Medical Diagnosis, ed 2. Boston, Little, Brown, 1979, pp 316-341.
Goldstein M (ed): The Research Status of Spinal Manipulative Therapy. Bethesda, MD, National Institutes of Health, DHEW Publication No. (NIH) 76-998, 1975, p 27.
Goodheart GJ: Collected Published Articles and Reprints. Montpellier, OH, Williams County Publishing, 1969, pp 23-24.
Gottschalk L: Psychologic factors in backache. General Practitioner, 33:91-94, 1966.
Grice AS: Muscle tonus change following manipulation. Journal of the Canadian Chiropractic Association, 18(4):29-31, 1974.
Grieve DW: The assessment of gait. Physiotherapy, 55:452-460, 1975.
Guyton AC: Textbook of Medical Physiology, ed 6. Philadelphia, W.B. Saunders, 1981, pp 626-670.
Haldeman S: The electrodiagnostic evaluation of nerve root function. Spine, 9(1):42-48, 1984.
Heilman KM, Watson RT, Greer M: Handbook for Differential Diagnosis of Neurologic Signs and Symptoms. New York, Appleton-Century-Crofts, 1977, pp 105-106.
Hibbard D: Effects of manipulation on gait muscle activity: preliminary electromyographic research. ACA Journal of Chiropractic, 17(10):104-106.
Hollingshead WH, Jenkins DB: Functional Anatomy of the Limbs and Back. Philadelphia, W.B. Saunders, 1981, pp 17-19, 38-42.
Holmes G: The cerebellum of man. Brain, 62:1-30, 1939.
Homewood AE: The Neurodynamics of the Vertebral Subluxation, ed 3. Place of publication not shown, published by author, 1981, pp 88-102, 130, 136-139, 284-286.
Hoppenfeld S: Physical Examination of the Spine and Extremities. New York, Appleton-Century-Crofts, 1976, pp 134-141.
Inman VT, Ralston HJ, Todd F: Human Walking. Baltimore, Williams & Wilkins, 1981, pp 2-21, 103-117.
Inman VT, Saunders JB: Referred pain from skeletal structures. Journal of Nervous and Mental Disorders, 99:660, 1944.
Janda V: Muscle and joint correlations. In Lewit K, Gutmann G (eds): Rehabitcia. Proceedings of the IVth Congress. Prague, International Federation of Manual Medicine, 1975, pp 154-157.
Janse J: The integrative purpose and function of the nervous system: A review of classical literature. Journal of Manipulative and Physiological Therapeutics, 1(3), September 1978.
Janse J: Principles and Practice of Chiropractic. Lombard, IL, National College of Chiropractic, 1976, pp 48-50, 73-74, 310-312.
Jaskoviak PA, Schafer RC: Applied Physiotherapy: Practical Applications Within Clinical Chiropractic. Arlington, VA, American Chiropractic Association, 1986, pp 55-58, 87-91, 113-114, 271-273.
Judge RD, Zuidema GD (eds): Methods of Clinical Examination: A Physiological Approach, ed 3. Boston, Little, Brown, 1968, pp 341-366.
Karvinen E, Komi PV: Neuromuscular performance. In Larson LA (ed): Fitness, Health, and Work Capacity. New York, Macmillan, 1974, pp 73-78, 81-86.
Kellgren JH: Observations on referred pain arising from muscle. Clinical Science, 3:175, 1938.
Keesler HH: Low Back Pain in Industry. New York, Commerce and Industry Association of New York, 1953.
Kessler RM, Hertling D (eds): Management of Common Musculoskeletal Disorders. Philadelphia, Harper & Row, 1983, pp 27-30, 91-98, 202-226.
Korr IM (ed): The Neurobiologic Mechanisms in Manipulative Therapy. New York, Plenum Press, 1978, pp 27-40, 61-62, 235-236, 375-390.
Korr IM: Proprioceptors and somatic dysfunction. Journal of the American Osteopathic Association, 74(3):638-650, 1975.
Krupp MA, Chatton MJ, Werdegar D: Current Medical Diagnosis & Treatment 1985. Los Altos, CA, Lange Medical, 1985, pp 605-610, 613-614.
Krupp MA, Tierney LM Jr, Jawetz E, Roe RL, Camargo CA: Physician's Handbook, ed 21. Los Altos, CA, Lange Medical, 1985, pp 34-53.
Landau WM, O'Leary JL: Disturbances of movement. In MacBryde CM, Blacklow RS (eds): Signs and Symptoms, ed 5. Philadelphia, J.B. Lippincott, 1970, pp 703-704.
Laporte Y, Emonet-Denand F, Jami L: The skeletal-fusimotor or beta-innervation of mammalian muscle spindles. TINS, 4(4):97-99, 1981.
Laufenberg PC: New dimensions in neurologic evaluation. The Digest of Chiropractic Economics, pp 10-12, 105-106, May/June 1979.
Luria AR: Higher Cortical Functions in Man. New York, Basic Books, 1966, pp 432-439.
MacBryde CM, Blacklow RS: Signs and Symptoms, ed 5. Philadelphia, J.B. Lippincott, 1970, pp 655-667.
MacDonald ML, Stanish WD: Neuromuscular system. In Scott WN, Nisonson B, Nicholas JA: Principles of Sports Medicine. Baltimore, Williams & Wilkins, 1984, pp 15-24.
Nouwen A, Bush C: The relationship between paraspinal EMG and chronic low back pain. Pain, 20(2):109-123, 1984.
Olson WH, Brumback RA, Gascon G, Christoferson LA: Practical Neurology for the Primary Care Physician. Springfield, IL, Charles C Thomas, 1981, pp 1-32, 98-114, 157-178, 236-269.
Pastan RS: Diffuse musculoskeletal pain. Diagnosis, 5(3):42-46, 1983.
Penry JK, Porter RJ: Epilepsy: Mechanisms and therapy. Medical Clinics of North America, 63:801-812, 1979.
Perry JA: Clinical interpretation of the mechanics of walking. Physical Therapy, 47:778-801, 1967.
Pinkenburg C: A basis for the theory of manipulative medicine. Journal of Manipulative and Physiological Therapeutics, 3(2):81-85, June 1980.
Pottenger FM: Symptoms of Visceral Disease, ed 6. St. Louis, C.V. Mosby, 1949.
Prichard JW: Nerve. In Albright JA, Brand RA (eds): The Scientific Basis of Orthopaedics. New York, Appleton-Century-Crofts, 1979, pp 408-412.
Prior JA, Silberstein JS: Physical Diagnosis, ed 5. St. Louis, C.V. Mosby, 1977, pp 394-418.
Quigley WH: Self-concept, mental health, and chiropractic. ACA Journal of Chiropractic, March 1971.
Rebechini-Zasadny H, Tasharski CC, Heinze WJ: Electromyographic analysis following chiropractic manipulation of the cervical spine: A model to study manipulation-induced peripheral muscle changes. Journal of Manipulative and Physiological Therapeutics, 4(2):61-63, 1981.
Reuber M, Schultz A, McNeil T, Spencer D: Trunk muscle myoelectric activities in idiopathic scoliosis. Spine, 8:447-456, 1983.
Roland MO: A critical review of the evidence for a pain spasm pain cycle in spinal disorders. Clinical Biomechanics, 1:102-109, 1986.
Rosse C: Muscle action and its control. In Rosse C, Clawson DK (eds): The Musculoskeletal System in Health & Disease. Hagerstown, PA, Harper & Row, 1980, pp 64-65, 70-75.
Rosse C: The vertebral column. In Rosse C, Clawson DK (eds): The Musculoskeletal System in Health & Disease. Hagerstown, NJ, Harper & Row, 1980, pp 138, 140.
Sandoz R: Some reflex phenomena associated with spinal derangements and adjustments. Annals of the Swiss Chiropractic Association, VII:45, 1981.
Sato A: The somatosympathetic reflexes. In Goldstein M (ed): The Research Status of Spinal Manipulative Therapy. NINCDS Monograph No. 15, DHEW Publication No. (NIH) 76-998, Washington, DC, U.S. Government Printing Office, 1975.
Sato A: Spinal and medullary reflex components of the somato-sympathetic reflex discharges evoked by stimulation of the group IV somatic afferents. Brain Research, 51:307-318, 1973.
Schafer RC: Chiropractic Management of Sports and Recreational Injuries. Baltimore, Williams & Wilkins, 1982, pp 471, 516, 527.
Schafer RC: Chiropractic Physical and Spinal Diagnosis. Oklahoma City, American Chiropractic Academic Press, 1980, pp I:30-34, II:29-30.
Schafer RC: Clinical Biomechanics: Musculoskeletal Actions and Reactions. Baltimore, Williams & Wilkins, 1983, pp 136-137, 148-158, 162-164.
Schafer RC (ed): Basic Chiropractic Procedural Manual, ed 4. Arlington, VA, American Chiropractic Association, 1984, pp 39, 517-558.
Schafer RC: Physical Diagnosis: Procedures and Methodology in Chiropractic Practice. Arlington, VA, American Chiropractic Association. In preparation. Released in 1987. Chapter 6, Basic Musculoskeletal Considerations; Chapter 7, Basic Neurologic Considerations.
Schafer RC: Symptomatology and Differential Diagnosis. Arlington, VA, American Chiropractic Association, 1986, pp 105-114, 294, 555-556, 939-940, 967-968.
Schwartz HS (ed): Mental Health and Chiropractic: A Multidisciplinary Approach. New Hyde Park, NY, Sessions, 1973.
Seliktar R, Susak Z, Najenson T, Solzi P: Dynamic features of standing and their correlation with neurological disorders. Scandinavian Journal of Rehabilitation Medicine, 10:59-64, 1978.
Shepherd GM: Microcircuits in the nervous system. Scientific American, 238(2): 92, 1978.
Singarajah KV: Neurophysiology evidence for manipulative therapeutic principles: Involvement of synaptic interaction. Annals of the Swiss Chiropractors' Association, 6:143-159, 1976.
Skully RL: The nervous system and its disorders. ACA Journal of Chiropractic, January and February 1972.
Soderberg GL: Kinesiology: Application to Pathological Motion. Baltimore, Williams & Wilkins, 1986, pp 39-43.
Spector B: Surface electromyography as a model for the development of standardized procedures and reliability testing. Journal of Manipulative and Physiological Therapeutics, 2:214-222, 1979.
Speransky AD: A Basis for the Theory of Medicine; translated by C.P. Dutt. New York, International Publishers, 1943.
Steward SL: An investigation into the effect of chiropractic adjustments on the psychological state of the patient. Bulletin of the European Chiropractic Union, 26(2):10-23, 47-59, 1978.
Stolov WC: Normal and pathologic ambulation. In Rosse C, Clawson DK (eds): The Musculoskeletal System in Health & Disease. Hagerstown, NJ, Harper & Row, 1980, pp 318-328.
Taylor RG, Fowler WM Jr: Electrodiagonosis of musculoskeletal disorders. In D'Ambrosia RD: Musculoskeletal Disorders: Regional Examination and Differential Diagnosis. Philadelphia, J.B. Lippincott, 1977, pp 61, 78-80, 84-85.
Thabe H: Electromyography as a tool to document diagnostic findings and therapeutic results associated with somatic dysfunctions in the upper cervical spinal joints and sacroiliac joints. Manual Medicine, 2:53-58, 1986.
Tran TA: Clinical correlations of the pyramidal system. The Chirogram, November 1976.
Tran TA: The motor system: A general look at its components and their clinical correlations. The Chirogram, October 1976.
Ufberg SH: Muscular nociception. ACA Journal of Chiropractic, 14:93-96, September 1980.
Vazuka FA: Essentials of the Neurological Examination. Philadelphia, Smith, Kline, & French Laboratories, 1962.
Walker HK, Hall WD, Hurst JW (eds): Clinical Methods. Woburn, MA, Butterworth, 1976, pp 796-839.
Walther DS: Applied Kinesiology; Volume I: Basic Procedures and Muscle Testing. Pueblo, CO, Systems DC, 1981, pp 220-223, 234-240.
Wayne KM: Disturbances of the nervous system as related to chiropractic. Journal of the Canadian Chiropractic Association, 13(2):20-23, 1969.
Widmann BJ: Electromyography for chiropractic. Annals of the Swiss Chiropractors' Association, 2:132-160, 1961.
Williams HG: An anatomical-functional review of selected CNS motor control structures. The Texas Chiropractor, April 1977.
Wood KW: Myospasm, myosprain and myalgia. The Digest of Chiropractic Economics, pp 126-127, May/June 1985.
Wolf SL (ed): Clinics in Physical Therapy: Electrotherapy. New York, Churchhill Livingstone, 1981.
Wyke BD: Articular neurology and manipulative therapy. In Aspects of Manipulative Therapy. Proceedings of Multidisciplinary International Conference on Manipulative Therapy. Melbourne, Lincoln Institute of Health Sciences, Carl ton, Victoria, Australia, August 1979, pp 67-72.
Zetterberg C, Bjork R, Ortengren R, Anderson GBJ: Electromyography of the paravertebral muscles in idiopathic scoliosis: measurements of amplitude and spectral changes under load. Acta Orthopaedica Scandinavica, 55:304-309, 1984.