

Qualitative Analysis of Illness Representations and
Coping Perceptions Among Older Adults With Chronic
Spinal Disability: "A Thought in the Back of My Mind"This section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Manipulative Physiol Ther 2021 (Oct); 44 (8): 652–662 ~ FULL TEXT
OPEN ACCESS Stacie A. Salsbury, PhD, RN • Michele Maiers, DC, MPH, PhD
Palmer Center for Chiropractic Research,
Palmer College of Chiropractic,
Davenport, Iowa.
Illness Representations and Coping PerceptionsObjective: The purpose of this study was to explore older adults' illness representations, their beliefs about health, and their coping perceptions of chronic spinal disability.
Methods: This qualitative descriptive study used structured interviews that were completed during a randomized trial of non-pharmacological management of spine-related disability with chiropractic spinal manipulative therapy and exercise. Dual coders conducted a descriptive thematic analysis of 50 randomly selected transcripts supported by qualitative data management software. The Common-Sense Model provided an organizing framework for coding and interpretation.
Results: Fifty participants (34 women, median age: 68 years) described 4 illness representations, 4 coping styles, and 6 coping strategies for their management of spinal disability. Illness representations formed a continuum of little-to-no health impact to bothersome symptoms to heightened symptom intensity to unmanaged pain and/or disability. Most participants adopted either self-care or self-management coping styles, but some used healthcare-seeking or fear avoidance with worsening symptoms or interference with employment or preferred activities. Participants mentioned 6 coping strategies for spinal disability. Distraction included position changes, hobbies, and supportive relationships. Limitation focused on rest and/or relaxation, restricted movements, and activity modifications. Prevention enhanced self-care knowledge, posture and/or ergonomics, nutrition, and stress management. Movement emphasized stretching, home exercise and/or walking, and exercise therapy. Palliation augmented patient comfort through the use of heat and/or ice, over-the-counter medicine, and spinal manipulation. Avoidance strategies included missing employment, stopping house and/or yard work, and prescription medication.
Conclusion: The community-dwelling older adults in this study offered varied illness representations of their chronic spinal disability. Most participants combined and personalized coping strategies to minimize pain and symptom impact; thus, representations may influence the coping styles adopted by older persons to manage their spinal conditions. A quote from a participant that pain was "a thought in the back of my mind" suggests the presence of cognitive and emotional processes that may influence individual perceptions and feelings about their spinal symptoms or conditions. These findings suggest that there may be a broader role for spine care clinicians to include teaching older people about self-management strategies to better cope with spinal disabilities.
Keywords: Adaptation, Psychological; Back Pain; Chronic Disease; Functional Status; Geriatrics; Illness Behavior; Models, Biopsychosocial; Patient Acceptance of Health Care; Qualitative Research.
From the FULL TEXT Article:
Introduction
Older adults often experience spinal disability, with pain and functional problems in the low back and neck commonly reported in this patient population. [1, 2] Spinal disability impacts the lives of older people by hampering mobility, limiting functional independence, and making engagement in work or social activity more difficult and less enjoyable. [1, 3] Spinal disability often persists over months or years [4] and demonstrates recognizable trajectory patterns, particularly for low back pain (LBP). [5, 6] Thus, for many people, spinal disability does not end with complete resolution of symptoms. [6] Rather, older persons with spinal disability experience varied states of recovery in which acceptance of chronic illness and long-term coping with spinal symptoms are ongoing aspects of everyday life. [7-9] Understanding how people with chronic spinal conditions make sense of their health and illness is important as clinical guidelines increasingly shift the locus of treatment from provider-based modalities to person-centered self-management strategies. [10, 11]
Illness representations are lenses through which patient and provider perceptions of health might be understood. Illness representations may be defined as the ways in which a person thinks and feels about their own health. Illness representations of spine-related conditions may have implications for how people recognize and experience their symptoms, the ways they cope with illness, their choice of health interventions, and the impact of those treatments on clinical outcomes. For example, illness representations of restricting back pain among older adults are an important construct encompassing a severe identity, a varying timeline, the perceived causes of prior occupation and age-related changes, the consequence of limitations in daily activities and quality of life, and the goal of symptom control. [12] Further, patient perceptions of restrictive back pain describe its inevitability in older age, negative attitudes about treatments, including medication and surgery, and the prioritization of other comorbidities, such as diabetes, heart disease, or kidney conditions, over musculoskeletal complaints by both the patient and their providers. [13] Although understanding the experience of restrictive back pain is essential, most older adults live with mild-to-moderate spinal symptoms. Little is known about the illness representations of older people with these more prevalent symptom profiles or about the coping perceptions of older patients who use non-pharmacological treatments for spinal disability.
People with spinal disability who are age 65 years and older may benefit from chiropractic care, especially for functional outcomes. [14-16] Chiropractic care may even offer protective effects against declines in physical function experienced by older people. [17] Doctors of chiropractic use several non-pharmacological treatments endorsed in clinical practice guidelines, including spinal manipulative therapy and exercise, to treat spine-related conditions. Chiropractors also commonly employ a range of other therapies in practice, including patient education, advice for activity, and self-care recommendations to encourage adaptive coping among their patients. [18-20] However, the ways in which spine care patients incorporate such recommendations into their coping strategies and self-management routines is not understood. One early practice-based, prospective study reported that chiropractic and medical patients each engaged in numerous self-care behaviors during and between LBP episodes, including making work modifications, using correct posture and lifting techniques, taking pain medication, and exercising. [21] A more recent survey of 1,677 chiropractic patients demonstrated regular, proactive use of many coping strategies among individuals with back pain, with the greatest range and frequency of coping techniques used by those with severe symptoms. [22] In that study, older adults were more likely to use medication, heat, and cold therapy but less likely to exercise than younger adults. [22]
These studies have provided useful insight into the coping strategies used by chiropractic patients. [21-23] However, clinicians also must understand how people think about their symptoms so that they may better support patients as they accept their illness and adopt new coping strategies to manage their spinal health. [24, 25] Critical knowledge gaps exist in understanding how patients think about self-management, including the decision to seek healthcare and the circumstances under which they use different coping strategies. Qualitative interviews, nested in a randomized controlled trial (RCT) of non-pharmacological interventions for chronic spinal disability in older adults, afforded the researchers an opportunity to consider how participants perceived their condition and their experiences managing it. [14, 26-28] Reading the interviews prompted the research question: how do older adults identify their chronic spinal condition, and how do they cope with it? Therefore, the purpose of this study was to describe spine-related illness representations, distinguish coping styles, and identify coping strategies among community-dwelling older people with chronic spinal disability.
Methods
This study was a secondary analysis of interview data derived from a qualitative study that was nested within an RCT. The RCT, conducted at Northwestern Health Sciences University in Bloomington, Minnesota, from January 2010 to October 2014, compared short-term (12 weeks) treatment or longer-term (36 weeks) management of spinal disability with chiropractic spinal manipulative therapy and supervised rehabilitative exercises. [14, 26] We used a qualitative descriptive design, a rigorous methodology well-suited for answering questions of importance to clinicians and patients, such as how do older adults think about and cope with spinal disability. [27] Advantages of qualitative descriptive designs include “low-interference”(p. 335) yet comprehensive data descriptions, openness in coding that allows researchers “choices about what to describe,”(p. 336) and a preference for the presentation and interpretation of data using “everyday language”(p. 336) as opposed to overly theoretical or jargonized language of other qualitative methodologies. [27]

Figure 1 As an organizing framework, we employed Leventhal's Common-Sense Model (CSM) of Self-Regulation, also known as the Common-Sense Model of Illness Representations, to characterize participants’ descriptions of their spinal disability. [29] The institutional review board at Northwestern Health Sciences University provided ethics approval (Project ID: 103-78-10-09). The trial was registered prospectively at ClinicalTrials.gov (NCT01057706). Participants provided written consent for RCT enrollment and gave verbal consent for interview audio-recording. Figure 1 provides an overview of the analysis process. A supplement offers methodological details outlined by the Consolidated Criteria for Reporting Qualitative Studies Checklist. [30]
Participants
Trial participants (n = 182) were 65 years or older and reported spine-related disability in both the low back and neck, with a minimum symptom duration of 12 weeks. [14, 26] Most participants (n = 171; 94%) completed an interview after the trial intervention phase. For this qualitative analysis, the investigators analyzed 50 randomly selected interviews (25 per treatment group), an a priori decision based on previous studies in which we reached thematic saturation after coding a similar percentage of available transcripts. [28, 31] Our qualitative sample included 34 women and 16 men, with a median age of 68 years (range 65-84), White racial/ethnic background (96%), and some college education (76%). For back pain, the mean (standard deviation) duration was 16.7 (13.1) years, pain severity in the past week was 5.2 (1.7) on a 0 to 10 numerical rating scale, and Back Disability Index was 27.0 (10.0) on a 0 to 100 scale. For neck pain, duration was 9.1 (9.2) years, pain severity was 4.6 (2.1), and Neck Disability Index was 25.4 (7.8). Demographic and clinical characteristics were similar to the RCT sample. [14, 28]
Data Collection and Management
Trained research staff conducted in-person, individual interviews using semi-structured, open-ended questions [32] to elicit participants’ perceptions about study treatment, which included probes about their approaches to managing spinal conditions. The audio-recorded interviews were transcribed verbatim and de-identified, with a 10% random sample of transcripts checked against the recording to ensure accuracy. Selected transcripts were imported into NVivo v9.2 (QSR International Pty Ltd, Victoria, Australia) for data analysis.
Qualitative Data Analysis and Organizing Framework
This secondary analysis used a qualitative descriptive design [27] with inductive (open-ended, data-driven) and deductive (confirmatory of an organizing framework) approaches. Both investigators independently read each transcript in its entirety to understand participants’ responses to the interview questions from the primary qualitative study. [28] Then, inspired by the work of Makris and colleagues [12, 13] and reflective of similarities to the general tenets of Leventhal's Common-Sense Model (CSM) of Self-Regulation, [29] we reconsidered these data through the lens of illness representations, coping styles, and coping strategies. Our coding process used both established codebooks developed during previous clinical trials [31, 33] and a flexible, template-style, open coding process to identify new codes and themes unique to this study. [28, 34] Template-style coding process is a rigorous yet less time-consuming approach to qualitative analysis that is well-suited for larger datasets (20 or more interviews) when understanding the perspectives of many different people within a specified context. [35] Within NVivo, salient transcript passages were selected, ascribed a node (code), and conceptually defined. Based upon our previous experience, [28] the investigators coded 10 transcripts and then convened via videoconference to compare our individual coding results. We achieved consensus on codes and definitions through discussion, revision, merger, or deletion of codes and organized updated coding within a primary NVIVO database. Each transcript was reviewed to assure all nodes were coded to this consensus codebook and further organized hierarchically in a thematic analysis to produce higher-ordered clusters of information. [29, 30]
Our analytic focus explored how these older adults were coping with or managing chronic spinal disability in their daily lives. We examined coding passages where participants described the strategies they used to lessen or prevent spinal symptoms, those instances when they sought care from providers, and times when they disengaged from activity. Repeated readings of the transcripts and coded passages allowed deeper comprehension of these older adults’ efforts to cope with their spinal symptoms, and semblances to the CSM surfaced. Broadly, the CSM framework posits that individuals understand and respond to symptoms, illnesses, or other threats to their health and well-being through cognitive and emotional processes. [29]
In its 50-year history, the CSM has served as a dynamic model for theoretical and clinical research, including within the field of musculoskeletal health. [12, 36, 37]
To apply this framework to this analysis, we organized codes into 3 facets of the CMS:
illness representations, coping styles, and coping strategies.
Illness representations were defined as the perceived impact of spinal symptoms on the individual's health.
Coping style was the individual's main management approach to their spinal symptoms.
Coping strategies identified specific actions to handle, manage, ignore, or otherwise cope with spinal symptoms. Representative quotations, identified by participant number, are presented as exemplars.
Results
Thematic Overview

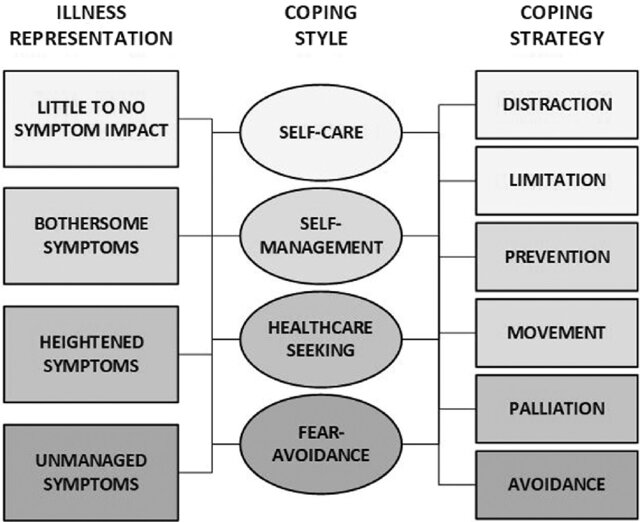
Figure 2 Older adults described their experience of spinal disability with varied language and offered many different examples of how they coped with their neck and back symptoms.
Our analysis coded these efforts into 4 illness representations, 4 coping styles, and 6 coping strategies (Figure 2).
Illness representations of spinal disability ranged along a continuum in which some participants noted little impact of spinal symptoms in their daily lives to experiences in which unmanaged pain and disability were commonly experienced.
Most participants described coping styles with a focus on self-care or self-management, although healthcare-seeking and fear-avoidance coping styles also were used, with little overlap or contemporaneous use between the different styles.
Participants mentioned multiple approaches to symptom management, which we classified into 6 coping strategies: distraction, limitation, prevention, movement, palliation, and avoidance.
Older adults often combined and personalized their coping strategies to minimize pain and symptom impact, but participants clearly had favored methods for managing spinal symptoms.
Illness Representations of Spinal Disability
Illness representations were categorized as little-to-no impact, bothersome, heightened symptom intensity, and unmanaged pain and/or disability. Participants who described spinal complaints as having little-to-no impact (n = 4) emphasized the minimal influence of symptoms on their daily activity:I keep going. It just hurts. I just do everything. I'm very active.
(19246)
Usually it doesn't [affect me] ‘til somebody asks me why my head's tilted to the right…they'll say, ‘Geez, I see your neck is botherin’ ya’. I've had it so long, I tend not to notice it…But it doesn't really bother me.
(17809)In contrast, illness representations of spinal disability described as bothersome (n = 31) focused on physical discomfort and the intrusive nature of pain, such as
“it's a pain, and it's a nuisance”
(18314),
“the pain starts to bother me”
(17930),
“aggravates me”
(17946), and
“it's just annoying, bugs me a lot”
(19488).Bothersome symptoms resulted in mild-to-moderate impacts on everyday activities, like driving or personal care:
“temporarily slows you up”
(18316) or
“it hurts when I drive, to turn my head”
(15525).Pleasurable activity, like pet care or going to movies, also might be affected:
[Pain] sometimes made it difficult for me to walk the dog. That is, pain in my neck and back caused me a fair amount of discomfort and the weight of the leash, believe it or not, I sometimes found oppressive or difficult.
(18900)Bothersome symptoms were characterized as transitory in duration, such as
“it's uncomfortable now, but it doesn't stop my world”
(18072) or
“it's a little inconvenient, but that's life”
(16016).Several older adults reported that bothersome symptoms interfered with their thoughts:
“when I've had the pain, it reminds me, it limits me”
(16921) or
“you can't concentrate ‘cuz you're thinking about that pain”
(16016).The combination of bothersome pain and aging affected cognition for some:
It's kind of a thought in the back of my mind that's always there when I'm in pain. It's a distraction…As I get older, my ability to really focus all the time at the task at hand, I notice some days, if my neck or my back is in pain, I don't focus as much. I acknowledge the pain and it distracts me.
(16699)Heightened symptom intensity was an illness representation described by several participants (n = 11). Spinal symptoms in this category were more constant in duration, greater in severity, and appreciably altered the daily lives of older adults through mobility impairments, decreased hobbies or housework, and postponement of social engagements. Relationships suffered, too.
When I have discomfort? I don't feel like doing anything…haven't been active as I should…a tendency to stay home more. If it's a choice, if it's someplace I have to walk (chuckles), I usually stay home. Unless it's a very short walk…then, I'll take a walker…if I have to go.
(15449)
I have to slow down and do less. I just sit more. My house is way dirtier than I want it to be (chuckles). I can't do some of my favorite hobbies – kayaking, hiking, horseback riding, walking…and sexually probably. I'm grumpier. Probably a little more conflict with my husband because I'm edgier and less patient.
(17085)Unmanaged pain and/or disability was an uncommon illness representation in this sample (n = 4), likely due to eligibility criteria that required participants be ambulatory, on stable pain medication, and without significant comorbidity. Nevertheless, a few participants described substantial limitations in employment from their spinal disability: “It affects my work, meaning that I can't work” (16359). Others voiced social disengagement, difficulty adopting new treatments, and emotional concerns:
I get depressed…I feel kinda hopeless, like, how am I gonna change anything, if I can't move… It's not that I can't move, it's just that my energy doesn't allow me to do what I really want to do. I would feel 400% better, if I could do the exercises. I know it. I feel like I am stuck.
(18842)
Coping Styles
Four coping styles for spinal disability were identified: self-care, self-management, healthcare seeking, and fear-avoidance.
Most participants described 1 primary coping style, although some adopted a secondary coping style with worsening pain or recurrent spinal symptoms. Many participants (n = 20) used a self-care coping style. These older adults were cautiously attentive to their symptoms but did not allow it to prevent them from engaging in activities:I feel pretty fortunate. At my age, I'm still able to do most of the things I want to do, only not with the duration that I'd like to do it sometimes.
(16699)
Most of the time it doesn't [affect me]. I just shuffle through whatever discomfort I have. Makes it a little more difficult to do a few things, but not overly so.
(18537)When faced with a sudden onset of pain or an acute problem with physical function, these older adults made modest attempts at self-care, such as resting, to relieve their discomfort or other symptoms:
Back one is the worst. I can't do anything when it comes…no warning is what I'm trying to say…it comes when I'm just standing. Then I just usually go upstairs and lay down.”
(15424)Older adults (n = 22) who used a self-management coping style addressed current symptoms with physical activity, and many did so to prevent recurrence of spinal symptoms. Participants managed their back complaint with exercise, stretching, ergonomic considerations, and other forms of movement to maintain posture, spinal function, and overall health:
A reminder that my posture isn't right…that discomfort in my neck or body periodically reminds me if I do some exercises, they'd be OK. That's one of the best things I have gotten from this program. You think I would catch on by the time I am 70, but no. Sometimes things take longer (chuckles).
(16921)Participants using self-management also described efforts to gain new knowledge about spine care and to reflect on how to accomplish goals while living with spinal pain, disability, or other symptoms:
[Pain] affects you if it's there. And it's been there. Learn to cope. Learn how to direct your life so that you can do the things you want to do in your life, in spite of the pain.
(17272)Older adults (n = 9) used a healthcare-seeking coping style when their spinal symptoms could not be self-managed, such as when symptoms negatively affected social events, sports participation, reading, or strenuous physical activities. Often used as a secondary coping style, several older adults turned to healthcare interventions, including participating in this research study, when spinal disability infringed on their paid employment:
This time of the year from January through May, I sit at a desk a lot, unfortunately, doing income taxes…my quality of life has improved from being in the study because I haven't gone home yet this year with a bad headache… learning some exercise techniques, getting the chiropractic treatment, I believe it's helped.
(16359)Some older adults (n = 9) described using a fear-avoidance coping style during periods of unmanaged pain and/or disability or when worried that intended activities might trigger a symptom flare-up or cause an injury to their spine:
Every aspect [of my life]. There's a fear of falling, a fear of doing activities that would put a strain on my back. I find that I wouldn't do those things then.
(16651)
I just try to be careful not to do something that would damage something, so that I can't keep going on. If I thought I was going to hurt myself, I would probably pull back and be careful.
(19522)
Coping Strategies

Table 1
See p.658Participants described 6 coping strategies for spinal disability: distraction, limitation, prevention, movement, palliation, and avoidance (Table 1).
Most older adults mentioned 1 or 2 preferred strategies, while some combined multiple approaches. Participants used coping strategies to manage symptoms, decrease pain, and engage in desired or required activities.Short-term, reactive strategies include distraction and limitation.
Proactive, long-term strategies included prevention and movement.
Palliative strategies may necessitate interactions with healthcare providers,
whereas avoidance strategies resulted in disconnection from other people and activities.Older adults used distraction, such as brief position changes, when spinal symptoms first were noticeable. Participants described how a short shift (seconds to minutes in duration), such as moving from sitting to standing, often offered relief.
In contrast, participants used limitation, such as resting, stopping activity, or modifying how they move through the world, for longer durations (minutes to hours) to reduce current symptoms.
Older adults who engaged in prevention did so as a form of chronic illness management. Learning new information, managing stress, and using good posture and ergonomics were thought to promote long-term spinal health.
Participants engaged in movement or exercise to maintain or improve long-term physical strength or fitness. Stretching movements or ‘loosening up’ the muscles might also be used as a short-term response to acute spinal symptoms.
Older adults who used palliation strategies sought respite from persistent pain or symptoms. Palliation could be applied in the home, through over-thecounter medication, heat or ice, or transcutaneous electrical nerve stimulation. These older adults also described practitioner-delivered interventions used for palliative purposes, such as massage and spinal manipulation.
Lastly, avoidance seemed to allow older adults to pull away from daily routines, housework, paid employment, or social activities, and at times, other people. Prescription medications to “deaden” the pain might also be used.
DISCUSSION
This qualitative study expands our current knowledge about the illness representations and coping perceptions of chronic spinal disability among older adults. That spine pain is “a thought in the back of my mind,” a quote from a participant, suggests that cognitive and emotional processes might be considered as an individual's perceptions and feelings about their spinal symptoms or conditions.
These data, although drawn from participants enrolled in an RCT comparing shorter-term and longer-term spinal manipulation and exercise, may be applicable to many older people who experience back and neck pain and dysfunction. [14. 26, 28] Our analysis was informed by the CSM of Self-Regulation, a well-established health framework for understanding how patients interpret and respond to their symptoms and illnesses using cognitive and emotional processes to guide their behavior. [29] One participant offered an insightful definition of illness representation useful for readers unfamiliar with this concept: “It's kind of a thought in the back of my mind that's always there when I'm in pain” (16699). Using this as an example, an illness representation is a thought or metaphor about health that an individual holds in their mind: in this case, a pain in one's back.
Individuals perceive meaning about their health using illness representations, [29] although this process may be informal and may not be shared with the healthcare provider. During their individual interviews, participants offered rich descriptions of the perceived impact of neck and back symptoms on their health and daily life. Participant reflections allowed us to categorize their coping styles and the context in which specific coping strategies were used to manage spinal disability. Our findings expand what is known about coping perceptions among persons who use non-pharmacological treatments, like chiropractic care, by going beyond previous investigations that simply list treatments used to manage spinal complaints. [21, 22] In contrast, we assembled these coping perceptions into a continuum of illness representations that can be considered relative to each another, according to an established conceptual framework, the CSM. [29] The resulting model may be a useful reference tool for communication between patients and providers to understand how spinal symptoms are experienced, what coping styles and strategies should be enhanced, and where changes should be made in treatment and self-management approaches.
Our findings are similar to the illness representations of restricting back pain elicited by Makris and colleagues [12, 13] as the older adults in both investigations described negative consequences of spinal disability in the areas of physical health, emotions, and social interactions. [12] However, the participants in the Makris study were older than our participants (median age 86 versus 68 years), reported at least 3 chronic conditions, and had severe enough symptoms to restrict daily activity for at least 3 months. [12] In our study, participants reported mild-to-moderate spinal pain and disability, many worked in paid employment, and most described engagement in numerous recreational and social activities. Thus, the illness representations described by our participants might be situated in the middle of a continuum of perceptions about spinal health.
These participants described their spinal disability as being bothersome, with periods of heightened spinal symptoms. Fewer described their illness representation on the low end of having little-to-no symptom impact or the high end of unmanaged pain and/or disability. Participants also described fluctuations in pain intensity and variations in symptom duration, similar to those reported in studies of LBP trajectories. [5]
A novel contribution of our study is our categorization of coping styles used by older spine care patients. Study participants’ descriptions of their typical approach to managing spinal symptoms usually aligned with 1 of 4 coping styles: self-care, self-management, healthcare seeking, and fear-avoidance. Participant narratives suggested some transition between coping styles when symptoms increased in duration or intensity, such as moving from a self-care to a healthcare-seeking style. However, most individuals seemed to respond to their spine-related condition with a primary coping style, which has clinical implications, such as assisting patients to recognize when their coping style may not be serving their best interests.
Encouragingly, nearly half of the participants in our study described a self-management coping style that embodies learning new information about spinal health or engaging in exercise to address current symptoms or prevent long-term declines. This finding supports previous research that older adults with higher levels of self-efficacy for management of musculoskeletal pain may be more likely to use coping strategies associated with better health outcomes, such as activity pacing, exercise or stretching, relaxation, and coping self-statements. [38, 39]
In contrast, coping styles that rely upon strategies, such as ignoring pain sensations or catastrophizing, similar to either the self-care or fear-avoidance styles described in our project, may lead to worsening pain or disability over time. [40] Healthcare professionals might engage in deep listening of patient stories to better understand the personal meaning of chronic spinal disability and the different ways that older people cope with spinal symptoms in their everyday lives to enhance active coping.
The older adults in our sample engaged in many of the same coping strategies, such as analgesic medicines, exercise, cognitive coping, activity restriction, and heat or cold modalities, described in studies of older patients with chronic musculoskeletal pain and disability and for chiropractic patients with back pain. [7, 21, 22, 41] Among older adults who experience post-surgical back and leg pain, adaptive coping with physical activity positively mediated the association between chronic pain and physical health and was negatively associated with the use of maladaptive coping strategies (eg, guarding, resting). [42] Adaptive coping strategies like task persistence, relaxation, and pacing activities are associated with less pain and positive affect among low back pain sufferers. [7] Conversely, maladaptive coping strategies like guarding, pain-contingent rest, and overreliance on social supports, are associated with greater pain, psychological distress, and increased disability. [43-45] For these reasons, best practice recommendations emphasize the importance of evaluating pain coping strategies among older adults with chronic back pain. [46]
Investigator Reflexivity
Investigator reflexivity may be defined as the practice through which researcher(s) examine our own beliefs about a topic and seek to understand how those beliefs may influence the research process. Our shared interest in older adults’ experiences with the treatment of musculoskeletal conditions stems from personal relationships with aging family members and friends from the Midwestern United States, many of whom had difficulty navigating a complex and often inadequate healthcare system to address multi-layered spinal conditions. Our complementary backgrounds as healthcare professionals (MM, a Doctor of Chiropractic, and SS, a Registered Nurse), supported a problem-solving approach, which led to the primary reflexive questions of this analysis: “How can older patients feel more enabled to manage their spinal conditions?” and “How can healthcare providers help?” Because of our familiarity with health promotion theories, we applied a pragmatic conceptual framework, the CSM to better situate our findings in the established literature. Finally, we used annotations, memos, and rigorous conversation at all steps of the research process to better understand how our beliefs guided this analysis and data interpretation.
Strengths
Our study design used multiple strategies to enhance methodological rigor, [34] including using dual coders from different disciplines (credibility), a rigorous consensus-building process to establish coding structures (credibility), and the use of qualitative data management software to document coding decisions (dependability). The completeness of our data was bolstered by the high receptivity of trial participants to engage in the qualitative interviews. While the transferability of our findings is limited by its clinical trial population, the large sample size (n = 50) for qualitative work, garnered randomly and equally from both treatment groups, suggests general representation of how older adults with mild-to-moderate spinal disability think and feel about their chronic health condition.
Limitations and Future Research
The qualitative data for this analysis were collected during an RCT in which participants received study-related care at no cost, including chiropractic spinal manipulation and exercise therapy. Although study treatments were designed to mirror the way they are typically delivered to patients in public settings, the absence of a financial exchange for services and the setting of a research clinic may have influenced participants’ responses. We feel the impact of this was likely minimal, however, as the research questions did not relate specifically to study treatment, focusing instead on managing their spinal conditions generally. Although older adults are under-represented in clinical trials for low back pain, [47] people who enroll in research may differ from typical patients seeking care for spinal disability. We used a random sample of 50 transcripts drawn from the sample of 171 participants who completed interviews in the RCT. [14, 26, 28] Although we balanced this sample by treatment group, individuals with differing clinical characteristics or life circumstances may have offered varying responses to those reported here. Chronic spinal disability increases with age and is more common in women, [1] which is reflective of this sample; however, non-White older adults and people reporting low socioeconomic status may report different coping styles and strategies than those reported here, and thus our findings may not be transferrable to other older adult populations. [4, 48] In addition, the clinical trial from which these data were derived took place in a metropolitan geographic area, and most participants had some familiarity or comfort with the interventions tested in the clinical trial. Persons living in settings with less access to healthcare services and those who do not wish to use non-pharmacological treatments for spinal disability may offer other perspectives than those described here. Although secondary analysis of qualitative data is an established methodological practice, [49] the original interview did not ask participants to describe their specific spine-related illness representations, coping styles, or coping strategies using those terms. Thus, our team is engaged in research to evaluate the findings reported here in a different sample of midlife and older persons.
Conclusion
Community-dwelling older adults who participated in an RCT of conservative care offered varied illness representations of their chronic spinal disability, which may influence the coping styles adopted by older persons to manage their spinal conditions. While self-care and self-management styles were espoused over healthcare-seeking and fear-avoidance behaviors, those coping styles, too, were important ways in which older adults coped with back and neck pain. While older adults, as a group, enumerated similar coping strategies to those reported in the literature, as individuals, many older people reported using only a few typical strategies. These results suggest a broader role for spine care clinicians in teaching older people about evidence-based self-management strategies to cope with spinal disability.
Practical Applications :
Qualitative interviews allowed older adults to richly describe their lived experience with spine-related disability.
The Common-Sense Model is a useful construct to represent the range of illness representations, coping styles, and coping strategies employed by older adults with spine conditions.
These results may allow both patients and providers to understand how spine symptoms are experienced and develop optimal coping styles and strategies.
Appendix
Appendix- Consolidated Criteria for Reporting Qualitative Studies (COREQ) Checklist (23KB .DOCX)
Funding Sources and Conflicts of Interest
The Chiropractic and Exercise Management of Spinal Dysfunction in Seniors Clinical Trial received direct national funding from the U.S. Department of Health and Human Services, Health Resources and Services Administration (HRSA), Bureau of Health Professions (BHPr), and the Division of Medicine and Dentistry (DMD) under Grant Number R18HP15127. Northwestern Health Sciences University and Palmer College of Chiropractic, Palmer Center for Chiropractic Research, provided in-kind salary support and resources for this analysis. The content and conclusions of this manuscript are those of the authors and should not be construed as the official position or policy of, not should any endorsements be inferred by the U.S. government, HHS, HRSA, BHPr, the DMD, or the authors’ academic institutions.
S.S. and M.M. have received funding from the NCMIC Foundation, Inc. S.S. and M.M. have received funding from the National Institutes of Health, National Center for Complementary and Integrative Health. S.S. is a board member of the Chiropractic Educators Research Forum and serves on the Research Committee of the World Federation of Chiropractic. M.M. is the president of the American Chiropractic Association.
Contributorship Information
Concept development (provided idea for the research): M.M., S.S.
Design (planned the methods to generate the results): M.M., S.S.
Supervision (provided oversight, responsible for organization and implementation, writing of the manuscript): S.S., M.M.
Data collection/processing (responsible for experiments, patient management, organization, or reporting data): M.M.
Analysis/interpretation (responsible for statistical analysis, evaluation, and presentation of the results): S.S., M.M.
Literature search (performed the literature search): S.S., M.M.
Writing (responsible for writing a substantive part of the manuscript): S.S., M.M.
Critical review (revised manuscript for intellectual content, this does not relate to spelling and grammar checking): M.M., S.S.
References
R Docking, J Fleming, C Brayne, J Zhao, G Macfarlane, G. Jones
Epidemiology of back pain in older adults:
prevalence and risk factors for back pain onset
Rheumatology, 50 (9) (2011), pp. 1645-1653D Hoy, C Bain, G Williams, et al.
A systematic review of the global prevalence of low back pain
Arthritis Rheumatol, 64 (6) (2012), pp. 2028-2037J Scheele, WTM Enthoven, SMA Bierma-Zeinstra, et al.
Characteristics of older patients with back pain in
general practice: BACE cohort study
Eur J Pain, 18 (2) (2014), pp. 279-287SD Rundell, KJ Sherman, PJ Heagerty, et al.
Predictors of persistent disability and back pain in older
adults with a new episode of care for back pain
Pain Med, 18 (6) (2017), pp. 1049-1062A Kongsted, P Kent, I Axen, AS Downie, KM. Dunn
What Have We Learned From Ten Years of
Trajectory Research in Low Back Pain?
BMC Musculoskelet Disord. 2016 (May 21); 17 (1): 220
Refer to our collected materials on
The Trajectories of Low Back Pain (2006-2024)A Kongsted, P Kent, L Hestbaek, W. Vach
Patients With Low Back Pain Had Distinct Clinical Course
Patterns That Were Typically Neither Complete Recovery
Nor Constant Pain. A Latent Class Analysis
of Longitudinal Data
Spine J. 2015 (May 1); 15 (5): 885–894
Refer to our collected materials on
The Trajectories of Low Back Pain (2006-2024)M Ersek, JA Turner, CA. Kemp
Use of the chronic pain coping inventory to assess
older adults’ pain coping strategies
J Pain Off J Am Pain Soc, 7 (11) (2006), pp. 833-842DE Beaton, V Tarasuk, JN Katz, JG Wright, C. Bombardier
"Are you better?" A qualitative study of the meaning of recovery
Arthritis Rheum, 45 (3) (2001), pp. 270-279C Myburgh, E Boyle, HH Lauridsen, L Hestbaek, A. Kongsted
What influences retrospective self-appraised recovery
status among Danes with low-back problems?
A comparative qualitative investigation
J Rehabil Med, 47 (8) (2015), pp. 741-747M Almeida, B Saragiotto, B Richards, CG. Maher
Primary Care Management of Non-specific Low Back Pain:
Key Messages from Recent Clinical Guidelines
Medical J Australia 2018 (Apr 2); 208 (6): 272–275R Meroni, D Piscitelli, C Ravasio, et al.
Evidence for managing chronic low back pain in primary care:
a review of recommendations from high-quality
clinical practice guidelines
Disabil Rehabil, 43 (7) (2021), pp. 1029-1043UE Makris, TV Melhado, SC Lee, HA Hamann, LM Walke, TM. Gill
Illness representations of restricting back pain:
the older person's perspective
Pain Med, 15 (6) (2014), pp. 938-946U Makris, R Higashi, E Marks, et al.
Ageism, negative attitudes, and competing co-morbidities -
why older adults may not seek care for restricting
back pain: a qualitative study
BMC Geriatr, 15 (2015), p. 39M Maiers, J Hartvigsen, R Evans, et al.
Short or Long-term Treatment of Spinal Disability
in Older Adults with Manipulation and Exercise
Arthritis Care Res (Hoboken). 2019 (Nov); 71 (11): 1516–1524CM Goertz, SA Salsbury, CR Long, et al.
Patient-centered Professional Practice Models
for Managing Low Back Pain in Older Adults:
A Pilot Randomized Controlled Trial
BMC Geriatr. 2017 (Oct 13); 17 (1): 235KR Holt, H Haavik, ACL Lee, B Murphy, CR. Elley
Effectiveness of Chiropractic Care to Improve
Sensorimotor Function Associated With Falls Risk
in Older People: A Randomized Controlled Trial
J Manipulative Physiol Ther. 2016 (May); (39) 4: 267–278P Weigel, J Hockenberry, S Bentler, F. Wolinsky
The Comparative Effect of Episodes of Chiropractic and
Medical Treatment on the Health of Older Adults
J Manipulative Physiol Ther 2014 (Mar); 37 (3): 143–154PJH Beliveau, JJ Wong, DA Sutton, et al.
The Chiropractic Profession: A Scoping Review of
Utilization Rates, Reasons for Seeking Care,
Patient Profiles, and Care Provided
Chiropractic & Manual Therapies 2017 (Nov 22); 25: 35P Dougherty, C Hawk, D Weiner, B Gleberzon, K Andrew, L
The Role of Chiropractic Care in Older Adults
Chiropractic & Manual Therapies 2012 (Feb 21); 20 (1): 3C Hawk, MJ Schneider, M Haas, et al.
Best Practices for Chiropractic Care for Older Adults:
A Systematic Review and Consensus Update
J Manipulative Physiol Ther 2017 (May); 40 (4): 217–229J Nyiendo, M Haas, B Goldberg, C. Lloyd
A descriptive study of medical and chiropractic patients
with chronic low back pain and sciatica: management
by physicians (practice activities) and
patients (self-management)
J Manip Physiol Ther, 24 (9) (2001), pp. 543-551CD Sherbourne, GW Ryan, MD Whitley, et al.
Coping and management techniques used by chronic low back
pain patients receiving treatment from chiropractors
J Manipulative Physiol Ther, 42 (8) (2019), pp. 582-593K de Luca, S Hogg-Johnson, M Funabashi, S Mior, SD. French
The Profile of Older Adults Seeking Chiropractic Care:
A Secondary Analysis
BMC Geriatrics 2021 (Apr 23); 21 (1): 271SC Baker, C Gallois, SM Driedger, N. Santesso
Communication accommodation and managing musculoskeletal disorders:
doctors’ and patients’ perspectives
Health Commun, 26 (4) (2011), pp. 379-388N Foster, J Hartvigsen, P. Croft
Taking responsibility for the early assessment and treatment
of patients with musculoskeletal pain:
a review and critical analysis
Arthritis Res Ther, 14 (1) (2012), p. 205C Vihstadt, M Maiers, K Westrom, et al.
Short Term Treatment Versus Long Term Management of Neck
and Back Disability in Older Adults Utilizing Spinal Manipulative
Therapy and Supervised Exercise: A Parallel-group Randomized
Clinical Trial Evaluating Relative Effectiveness and Harms
Chiropractic & Manual Therapies 2014 (Jul 23); 22: 26M. Sandelowski
Whatever happened to qualitative description?
Res Nurs Health, 23 (4) (2000), pp. 334-340M Maiers, SA. Salsbury
"Like Peanut Butter and Jelly": A Qualitative Study
of Chiropractic Care and Home Exercise Among
Older Adults with Spinal Disability
Arthritis Care Res 2022 (Nov); 74 (11): 1933–1941H Leventhal, LA Phillips, E. Burns
The Common-Sense Model of Self-Regulation (CSM):
a dynamic framework for understanding
illness self-management
J Behav Med, 39 (6) (2016), pp. 935-946A Tong, P Sainsbury, J. Craig
Consolidated criteria for reporting qualitative research
(COREQ): a 32-item checklist for interviews
and focus groups
Int J Qual Health Care, 19 (6) (2007), pp. 349-357M Maiers, MA Hondras, SA Salsbury, G Bronfort, R. Evans
What Do Patients Value About Spinal Manipulation and Home
Exercise for Back-related Leg Pain? A Qualitative Study
Within a Controlled Clinical Trial
Manual Therapy 2016 (Dec); 26: 183–191N. Britten
Qualitative interviews in medical research
BMJ, 311 (6999) (1995), pp. 251-253M Maiers, C Vihstadt, L Hanson, R. Evans
Perceived Value of Spinal Manipulative Therapy and
Exercise Among Seniors With Chronic Neck Pain:
A Mixed Methods Study
J Rehabil Med. 2014 (Nov); 46 (10): 1022–1028BF Crabtree, WL. Miller
Doing Qualitative Research
(2nd ed.), Sage Publications, Inc.,
Newbury Park, California (1999)N. King
Using templates in the thematic analysis of text
C Cassell, G Symon (Eds.),
Essential Guide to Qualitative Methods in Organizational Research,
SAGE Publications, Newbury Park,
California (2004), pp. 256-270P van Wilgen, A Beetsma, H Neels, N Roussel, J. Nijs
Physical therapists should integrate illness perceptions
in their assessment in patients with chronic
musculoskeletal pain; a qualitative analysis
Man Ther, 19 (3) (2014), pp. 229-234AA Kaptein, J Bijsterbosch, M Scharloo, SE Hampson
Using the common sense model of illness perceptions to
examine osteoarthritis change:
a 6-year longitudinal study
Health Psychol, 29 (1) (2010), pp. 56-64JA Turner, M Ersek, C. Kemp
Self-efficacy for managing pain is associated with
disability, depression, and pain coping among
retirement community residents with chronic pain
J Pain, 6 (7) (2005), pp. 471-479M Ersek, JA Turner, KC Cain, CA. Kemp
Results of a randomized controlled trial to examine the
efficacy of a chronic pain self-management group
for older Adults [ISRCTN11899548]
Pain, 138 (1) (2008), pp. 29-40K Benyon, S Muller, S Hill, C. Mallen
Coping strategies as predictors of pain and disability in
older people in primary care: a longitudinal study
BMC Fam Pract, 14 (1) (2013), p. 67LC Barry, RD Kerns, Z Guo, BD Duong, LP Iannone, M Carrington Reid
Identification of strategies used to cope with chronic pain
in older persons receiving primary care from a
Veterans Affairs Medical Center
J Am Geriatr Soc, 52 (6) (2004), pp. 950-956D. Higuchi
Adaptive and maladaptive coping strategies in older adults
with chronic pain after lumbar surgery
Int J Rehabil Res, 43 (2) (2020), pp. 116-122MM Wertli, R Eugster, U Held, J Steurer, R Kofmehl, S. Weiser
Catastrophizing—a prognostic factor for outcome in patients
with low back pain: a systematic review
Spine J, 14 (11) (2014), pp. 2639-2657MM Wertli, E Rasmussen-Barr, S Weiser, LM Bachmann, F. Brunner
The role of fear avoidance beliefs as a prognostic factor
for outcome in patients with nonspecific low back pain:
a systematic review
Spine J, 14 (5) (2014), pp. 816-836 e4AC Mercado, LJ Carroll, DJ Cassidy, P. Côté
Passive coping is a risk factor for disabling neck or
low back pain
Pain, 117 (1) (2005), pp. 51-57EA DiNapoli, M Craine, P Dougherty, et al.
Deconstructing Chronic Low Back Pain in the Older Adult -
Step by Step Evidence and Expert-Based Recommendations
for Evaluation and Treatment.
Part V: Maladaptive Coping
Pain Medicine 2016 (Jan); 17 (1): 64–73T Paeck, ML Ferreira, C Sun, CWC Lin, A Tiedemann, CG. Maher
Are older adults missing from low back pain clinical trials?
A systematic review and meta-analysis
Arthritis Care Res (Hoboken), 66 (8) (2014), pp. 1220-1226FRD Jesus-Moraleida, PH Ferreira, ML Ferreira, JPD Silva
The Brazilian Back Complaints in the Elders (Brazilian BACE)
study: characteristics of Brazilian older adults with
a new episode of low back pain
Braz J Phys Ther, 22 (1) (2018), pp. 55-63S Ziebland, K. Hunt
Using secondary analysis of qualitative data of patient
experiences of health care to inform health
services research and policy
J Health Serv Res Policy, 19 (3) (2014), pp. 177-182

Return to SPINAL PAIN MANAGEMENT
Since 5-19-2026| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |