

The Vast Majority of Patients With Fibromyalgia
Have a Straight Neck Observed on a Lateral View
Radiograph of the Cervical Spine: An Aid in
the Diagnosis of Fibromyalgia and a
Possible Clue to the EtiologyThis section was compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Clinical Rheumatology 2023 (Mar 1); 29 (2): 91–94 ~ FULL TEXT
OPEN ACCESS Robert S Katz, MD, Frank Leavitt, PhD, Katya Cherny,MS , Alexandra Katz Small, MD, Ben J Small, MD
From the Rush Medical University.
Rheumatology Associates.
Northwestern University Medical Center,
Chicago, IL.Objective: A straight cervical spine is an underappreciated and often overlooked finding in fibromyalgia. The aim of this medical records review study was to evaluate the cervical curvature on radiographs of patients with fibromyalgia.
Methods: A consecutive series of 270 cervical spine radiographs of patients with neck pain from 2015 to 2018 were retrospectively analyzed for cervical curvature using the Cobb angle measurement. One hundred fifty-five patients met full American College of Rheumatology criteria for fibromyalgia, whereas 115 subjects with other rheumatic diseases who were similar in age and education served as control subjects.
Results: Mean cervical curvature in fibromyalgia was 6.4 ± 5.2 degrees and 13.8 ± 7.4 degrees in control subjects. The more than 7-degree difference was significant (p < 0.001). Curvature in the magnitude of 21 degrees is at the low end of normal. At ≤10 degrees, where the cervical spine is essentially straight, there were 129 fibromyalgia patients (83.2%) and 37 control subjects (32.2%). The 51% difference was significant (p < 0.001).
Conclusion: Most patients with fibromyalgia share an abnormality in common that is verifiable by a simple radiograph. In 83.2% of the patients, the cervical spine was essentially straight (Cobb angle ≤10 degrees). In fibromyalgia patients, the loss of cervical curvature was approximately 6.5 times greater than in control subjects (50.3% vs. 7.8%). A straight neck without other radiographic abnormalities may be a major anatomical abnormality in fibromyalgia that has gone unnoticed. It may assist in the diagnosis, as well as suggest increased muscle tension/pressure as a possible etiology.
Keywords: cervical spine; fibromyalgia; muscle pressure; radiograph
From the FULL TEXT Article:
BACKGROUND
A straight neck seen on radiographs is a stealth feature that is undetected in the evaluation of patients with fibromyalgia. It is our distinct impression from observing lateral view radiographs of the cervical spine that the normal lordotic curve is missing or reduced in the absence of other radiographic abnormalities in patients with fibromyalgia. In many patients, the cervical spine shows a curvature to approach 0 degrees or a straight line. Variations this far outside of the natural appearance bring into question whether a straight line is the configuration of the cervical spine for most patients with fibromyalgia. This study assesses the lack of curvature in the neck of fibromyalgia patients.
Vertebrae from the base of the skull to C7 constitute the first of 4 structural curves of the spine1 and form the cervical lordotic curve. With an apex that curves naturally forward analogous to a reverse “C,” the 7 vertebrae create curvature in the magnitude of 21 to 43 degrees. [2, 3] With proper alignment, the cervical spine acts in synergy with the 3 adjacent curves (thoracic, lumbar, and sacral) to confer posture, mobility, and balance of the spine. Working in unison, the 4 curves of the spine form a spring-like structure that protects the body from vibrations arising from motion. [4]
Abnormal alignment of the cervical spine may be a diagnostic sign as well as a clue to the mechanism for understanding the pain in fibromyalgia. The loss of the normal cervical spine lordotic curve eliminates 1 of the 4 spinal curves that act like protective pillows against the vibrations of motion.
METHODS
We analyzed the medical records of patients who had cervical spine radiographs in a rheumatology office practice. A consecutive series of 270 patients who underwent radiographic examination of the cervical spine for moderate to severe neck pain over a 4-year period from 2015 to 2018 formed the subject pool. Among these patients, 155 met the American College of Rheumatology (ACR) criteria for fibromyalgia, [5] and 115 met the ACR criteria for another rheumatic disease. Inclusion criteria were ages 18 to 70 years, neck pain of moderate to severe intensity, and meeting the full ACR criteria for a rheumatic disease. Exclusion criterion was history of cervical spine surgery. All patients had radiographs performed at 1 location, a rheumatology office practice.
The alignment of the cervical spine was evaluated using lateral view radiographs. The radiographs were taken in a standing position with a tube-to-film distance of 72 inches. Patients were instructed to stand relaxed and to look straight ahead. Positioning procedure was standard. [6] Cervical spine views were centered at the C4 cervical vertebra.
The convention has been adopted to measure the lordotic cervical curve from C2 to C7. [2] A line drawn from the top of C2 and another line drawn from the bottom of C7 create the Cobb angle, considered to be the most usable metric for quantifying lordotic curvature. [7, 8] Perpendicular lines were drawn to the line across the top of C2 and the line across the bottom of C7, and the angle of these intersecting lines was measured with a protractor. EvoView software (Umg/Del Medical, Bloomingdale, IL) was also used to measure the Cobb angle. Because radiographic measurement is dependent on image quality, radiographs were excluded with low image quality that resulted in poor visualization of the C2 or C7 end plates using the measurement of the Cobb angle or from motion artifact.
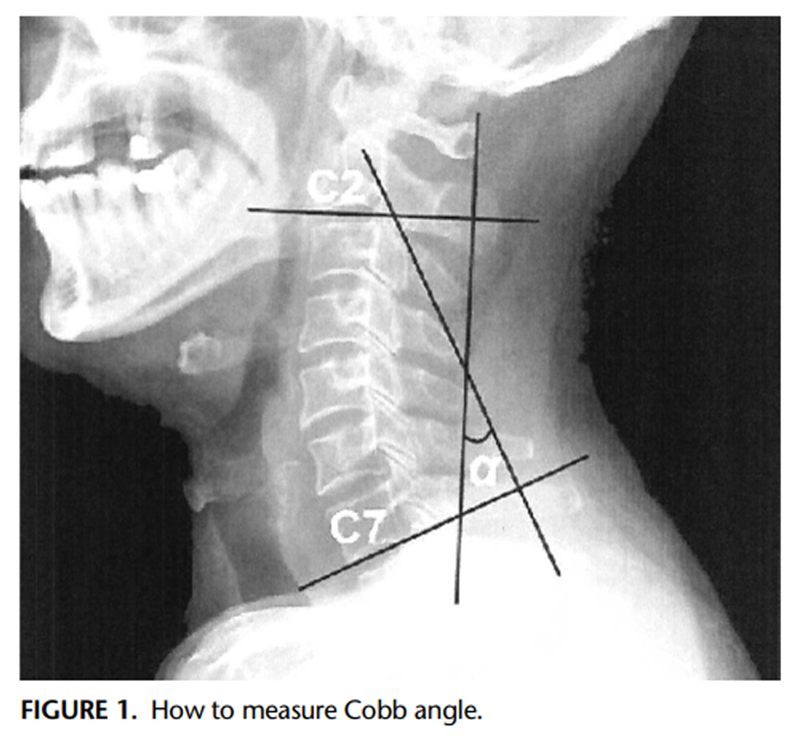
Figure 1 Cobb angle measurement (Figure 1) was conducted by a radiology technician with more than 10 years’ experience with the calculation of Cobb angles and blind to the diagnosis. Interobserver reliability was assessed by comparing Cobb measurements of the cervical curve obtained by a second independent examiner, a rheumatologist who was also blind to the diagnosis on 20 randomly selected radiographs from the fibromyalgia and nonfibromyalgia patient groups. Interrater reliability was excellent based on a Pearson correlation of 0.91.
Statistical analyses were performed using SPSS version 22.0 for Windows (IBM Corp, Armonk, NY). Differences between groups of continuous variables were analyzed by the Student t test with corresponding 95% confidence intervals. Differences between groups on categorical data were analyzed by the χ2 test. p ≤ 0.05 was considered statistically significant. To assess interrater reliability for the Cobb angle, Pearson correlation coefficients were calculated.
RESULTS

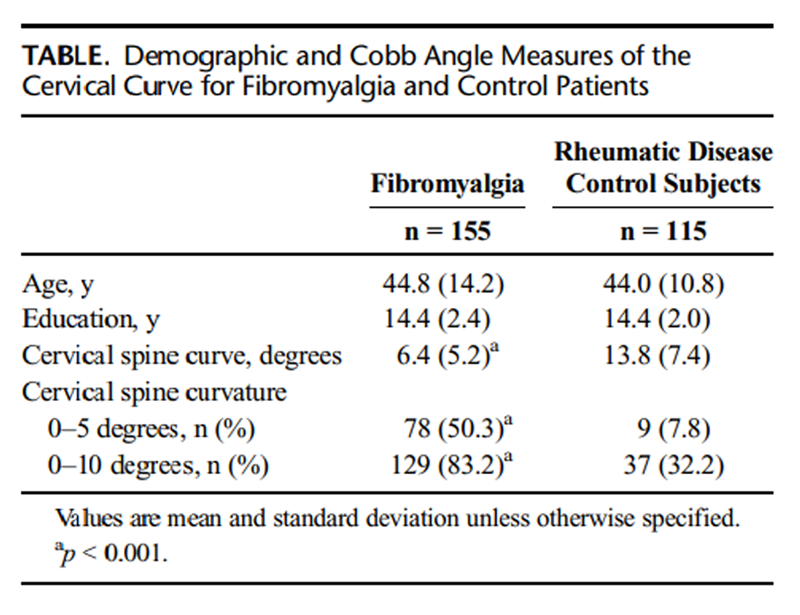
Table 1 The study enrolled a total of 155 adult female patients with fibromyalgia and 115 adult female control subjects with another rheumatic disease other than fibromyalgia. The control subjects included 30 subjects (26.1%) with rheumatoid arthritis; 26 subjects (22.6%) with systemic lupus erythematosus; 14 subjects (12.2%) with ankylosing spondylitis; 13 subjects (11.3%) with osteoarthritis in their knees, hands, and other joints including the cervical spine; and 32 subjects (27.8%) had nonspecific neck pain. The Table lists patient characteristics and Cobb angle measurements. As can be seen, the mean age and education of the 2 groups did not significantly differ (p > 0.05).
Cervical lordosis measured by the Cobb angle from C2 to C7 showed a mean curvature of 6.4 ± 5.2 degrees in fibromyalgia patients and 13.8 ± 7.4 degrees in control subjects. The more than 7-degree difference was significant at the p < 0.001 level. The cervical spine is essentially visually straight at ≤10 degrees. There were 129 fibromyalgia patients (83.2%) and 37 control subjects (32.2%) with a cervical Cobb angle of 10 degrees or less. The 50+ percentage difference between the 2 groups was significant (p < 0.001). At ≤5 degree where straightening of the cervical spine is fairly complete, there were 78 fibromyalgia patients (50.3%) and 9 control subjects (7.8%). The 42% difference was significant (p < 0.001). Two independent raters blind to the diagnosis exhibited a high degree of consensus in scoring the Cobb angle. The Pearson correlation for the 2 raters was 0.91.
DISCUSSION
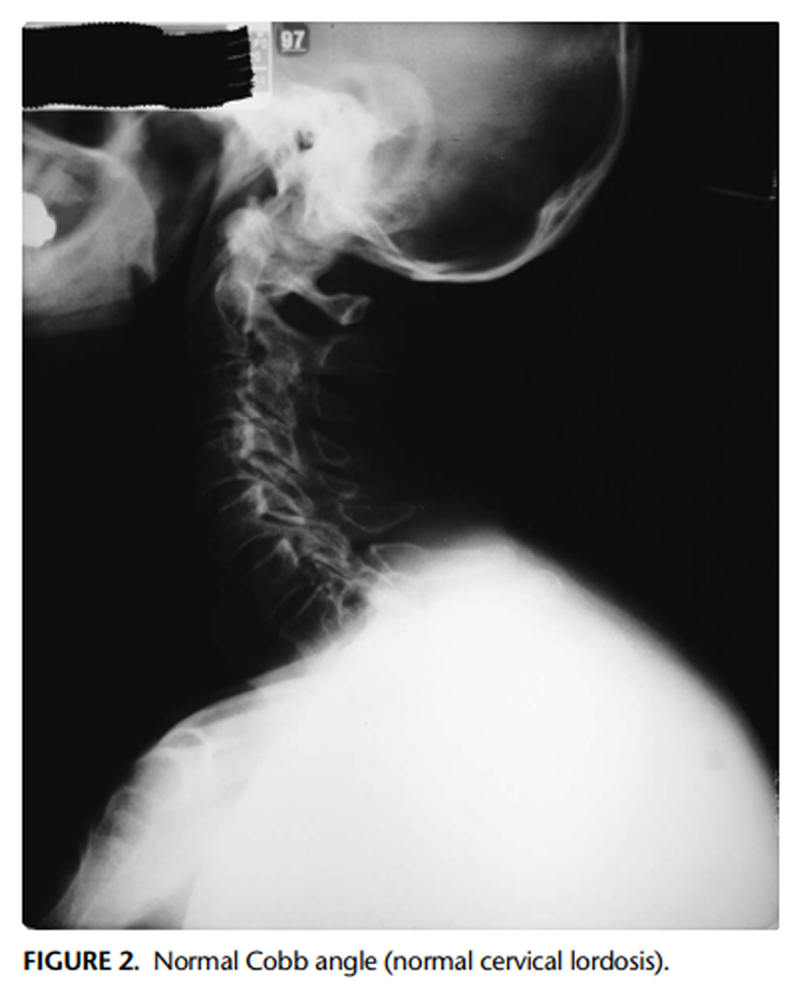
Figure 2
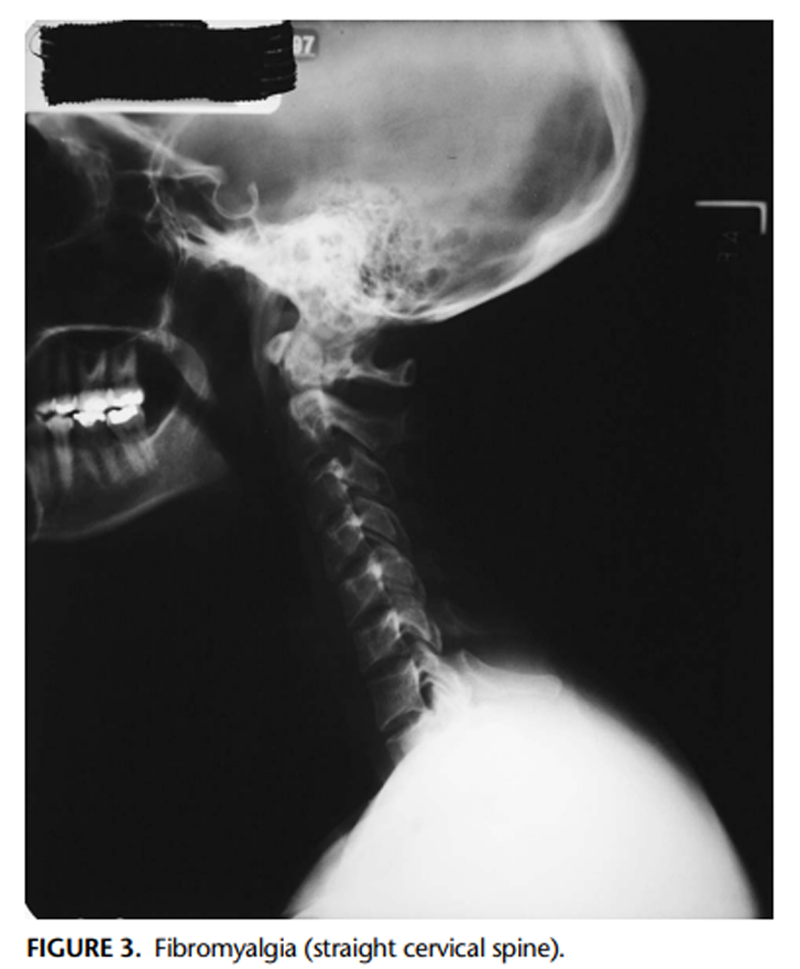
Figure 3 Our data indicate that the great majority of patients in the fibromyalgia group showed radiographic evidence of cervical spine straightening (Figures 2 and 3). In 83.2% of the patients, the cervical spine was essentially straight (Cobb angle of ≤10 degrees). A complete loss of cervical lordosis (Cobb angle ≤5 degrees) affected 50.3% of the fibromyalgia sample. This loss of curvature was more than 6 times greater than that found in the control sample (50.3% vs. 7.8%). For patients with fibromyalgia, a straight neck may be the natural configuration of the cervical spine.
Curvature of the cervical spine in fibromyalgia patients differs from the normal variation in cervical curvature found in the general population. A consensus on normative curves for the cervical spine is lacking, with the literature reporting a wide range of normal values for the Cobb angle from a low of 21 degrees to a high of 43 degrees. [2, 3, 8] In the case of fibromyalgia, there is a sharp departure from the lower boundary of these values, with the great majority of the fibromyalgia curvature scores well outside the range of reference values reported, suggesting the cervical spine normality in fibromyalgia is different.
The radiographs of the fibromyalgia and rheumatic disease control groups were alike in some respects; both rheumatologic groups with neck pain showed a diminished cervical lordotic curve with the mean curvature as measured from radiographs on average 7 degrees smaller in the fibromyalgia group. Diminished lordosis in the control group with neck pain was not unexpected, as reduced lordosis is overrepresented in patient groups with neck pain as part of their rheumatic disease. [7]
The loss of cervical lordosis in fibromyalgia has not been previously described, and its roots are unclear. It may be abnormal because curvature of the cervical spine has flattened or possibly was never present. In the case of change of the cervical spine, there is good evidence that the natural cervical curve can be lost or diminished by traumatic events such as whiplash. [9, 10]
We have found muscle pressure using a pressure gauge with a needle inserted into the trapezius muscle to be 3 times higher in fibromyalgia patients compared with control subjects. [11] It is possible that the increased muscle tension leads to straightening of the cervical spine. [12]
However, there is also evidence that diminished curvature of the cervical spine is not always a later life event. It can predate the adult years. In a 2017 study of radiographs of individuals aged 6 to 19 years, diminished cervical curves were encountered in 23% of the sample. [13]
Looking back at the early writings on fibromyalgia, one is struck by the seminal observations of Smythe, [14] who was the first to foresee an important connection between the origins of pain in fibromyalgia and the difficulties at the level of the cervical spine. [14] He recommended using a special neck pillow for fibromyalgia patients because he reasoned that the neck is unsupported by musculature in humans compared with all other animals. [15]
The present study also opens a window on how the cervical spine might become a diagnostic aid, as well as a possible clue to etiology including increased muscle tension.
Our study had several limitations. First, the study was performed by reviewing the patients medical records, which may represent a design bias. Second, the subjects were all referrals for cervical imaging. This may have skewed the sample toward those with greater symptoms. Third, this is a single-site study, which may limit the generalizability of the findings. Finally, imaging abnormalities were detected by plain film radiographs. A broader spectrum of abnormalities might have been detected with computed tomography or magnetic resonance imaging scans.
Fibromyalgia is thought to be well characterized in the 2010 revision of criteria for fibromyalgia. [5] However, a major shortcoming is the absence of any objectively measurable findings. The subjectivity of the key features of fibromyalgia—widespread pain sites, fatigue, sleep disorder, cognitive dysfunction, and somatic symptoms—can pose uncertainties to the treating physician, which may make them hesitant to diagnose. However, the magnitude of cervical spine involvement with a straight cervical spine seen on lateral radiographs views encountered in this study could provide an additional aid in the diagnosis.
The evidence is substantial that fibromyalgia affects the cervical spine. When a patient has fibromyalgia, the cervical spine is not normal; it is misaligned. Curvature is partially or fully flattened. Upward of 80% of the patients with fibromyalgia show flattening of the cervical curvature. In fact, in 50% of the patients, there is complete loss of lordotic curvature as reflected in the Cobb angle ≤5 degrees.
Patients with the symptoms and signs of fibromyalgia share an abnormality that is verifiable by a simple radiograph, a lateral view of the cervical spine. By providing support for an observable abnormality, it helps take fibromyalgia out of the subjective realm. It is often heard medically that nothing was found, but through the lens of a simple x-ray, a rheumatologist can see and measure an abnormality in the alignment of the cervical spine that may be another signature feature associated with fibromyalgia.
The complete loss of lordosis (Cobb angle ≤5 degrees) is common among those with fibromyalgia, especially without other visible radiographic abnormalities. It affects those with fibromyalgia more than 6 times more often than those with other rheumatic disease disorders and in concert with an otherwise normal cervical radiograph likely signals fibromyalgia. A straight cervical spine may also occur in other rheumatic diseases but is generally accompanied by other significant radiographic abnormalities such as intervertebral disc space narrowing, spondylolisthesis, bony productive changes, and facet osteoarthritis.
Radiograph lateral views of the neck provide a valuable tool in transforming the diagnostic process for fibromyalgia and should be considered a part of the evaluation.
References:
Frymoyer JW.
The Adult Spine. Principles and Practice. 2nd ed.
Philadelphia, PA: Lippincott-Raven; 1997Gore DR, Sepic S, Gardner G.
Roentgenographic findings of the cervical spine in asymptomatic people.
Spine. 1986;11:521–524Shealy CN.
Restoration of normal cervical lordosis.
Pract Pain Manage. 2009;14:42–43Benzel EC.
Biomechanics of Spine Stabilization: Principles & Clinical Practice.
New York: McGraw-Hill; 1995Wolfe F, Clauw DJ, Fitzcharles MA, et al.
The American College of Rheumatology preliminary diagnostic criteria
for fibromyalgia and measurement of symptom severity.
Arthritis Care Res. 2010;62:600–610Harrison DE, Harrison DD, Colloca CJ, et al.
Repeatability over time of posture, radiograph positioning and
radiograph line drawing: an analysis of six control groups.
J Manipulative Physiol Ther. 2003;26:87–98McAviney J, Schulz D, Bock R, et al.
Determining the relationship between cervical lordosis and neck complaints.
J Manipulative Physiol Ther. 2005;28:187–193Gelb DE, Lenke LG, Bridwell KH, et al.
An analysis of sagittal spinal alignment in 100
asymptomatic middle and older aged volunteers.
Spine. 1995;20:1351–1358Eyadeh AA, Kondeva M, Khamees MF, et al.
Neck pain, neck mobility and alignment of cervical spine
in 30 patients with cervical strain.
Kuwait Med J. 2004;36:186–190Hohl M.
Soft tissue injuries of the neck in automobile accidents.
J Bone Joint Surg Br. 1974;56a:1675–1681Katz RS, Leavitt F, Small AK, et al.
Intramuscular pressure is almost three times higher in fibromyalgia patients:
a possible mechanism for understanding the muscle pain and tenderness.
J Rheumatol. 2021;48:598–602Helliwell PS, Evans PF, Wright V.
The straight cervical spine: does it indicate muscle spasm?
J Bone Joint Surg Br. 1994;76:103–106Been E, Shefi S, Soudack M.
Cervical lordosis: the effect of age and gender.
Spine J. 2017;17:880–888Smythe H. Editorial.
The “repetitive strain injury syndrome” is referred pain from the neck.
J Rheumatol. 1988;15:1604–1608Helewa A, Goldsmith CH, Smythe HA, et al.
Effect of therapeutic exercise and sleeping neck support on
patients with chronic neck pain: a randomized clinical trial.
J Rheumatol. 2007;34:151–158.
Return to RADIOLOGY
Return to FIBROMYALGIA
Return to SPINAL ALLIGNMENT
Since 11-06-2022
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |