

Cervicogenic Headaches:
A Critical ReviewThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Spine J 2001 (Jan); 1 (1): 31–46 ~ FULL TEXT
OPEN ACCESS Scott Haldeman, DC, MD, PhD, Simon Dagenais, DC
Department of Neurology,
University of California, Irvine,
Medical Center,
101 The City Drive South,
Orange, CA 92868, USA.
Background context: The notion that headaches may originate from disorders of the cervical spine and can be relieved by treatments directed at the neck is gaining recognition among headache clinicians but is often neglected in the spine literature.
Purpose: To review and summarize the literature on cervicogenic headaches in the following areas: historical perspective, diagnostic criteria, epidemiology, pathogenesis, differential diagnosis, and treatment.
Study design/setting: A systematic literature review of cervicogenic headache was performed.
Methods: Three computerized medical databases (Medline, Cumulative Index to Nursing and Allied Health Literature [CINAHL], Mantis) were searched for the terms "cervicogenic" and "headache." After cross-referencing, we retrieved 164 unique citations; 48 citations were added from other sources, for a total of 212 citations, although all were not used.
Results: Hilton described the concept of headaches originating from the cervical spine in 1860. In 1983 Sjaastad introduced the term "cervicogenic headache" (CGH). Diagnostic criteria have been established by several expert groups, with agreement that these headaches start in the neck or occipital region and are associated with tenderness of cervical paraspinal tissues. Prevalence estimates range from 0.4% to 2.5% of the general population to 15% to 20% of patients with chronic headaches. CGH affects patients with a mean age of 42.9 years, has a 4:1 female disposition, and tends to be chronic. Almost any pathology affecting the cervical spine has been implicated in the genesis of CGH as a result of convergence of sensory input from the cervical structures within the spinal nucleus of the trigeminal nerve. The main differential diagnoses are tension type headache and migraine headache, with considerable overlap in symptoms and findings between these conditions. No specific pathology has been noted on imaging or diagnostic studies which correlates with CGH. CGH seems unresponsive to common headache medication. Small, noncontrolled case series have reported moderate success with surgery and injections. A few randomized controlled trials and a number of case series support the use of cervical manipulation, transcutaneous electrical nerve stimulation, and botulinum toxin injection.
Conclusions: There remains considerable controversy and confusion on all matters pertaining to the topic of CGH. However, the amount of interest in the topic is growing, and it is anticipated that further research will help to clarify the theory, diagnosis, and treatment options for patients with CGH. Until then, it is essential that clinicians maintain an open, cautious, and critical approach to the literature on cervicogenic headaches.
Keywords: Cervicogenic; Headache; Review
From the FULL TEXT Article:
Introduction
It is common in clinical practice to encounter conditions that are widespread and routinely treated but that suffer from limited research and lack of consensus among experts. Cervicogenic headache (CGH) is one of these conditions. Although the idea that headaches can originate from structures in the neck and can be treated by interventions directed at the cervical spine is long-standing, it is only in the past two decades that the topic has gained attention in the mainstream headache and pain literature. There are now several associations dedicated solely to studying CGH, including the Cervicogenic Headache International Study Group and the World Cervicogenic Headache Society (WCHS). These societies are comprised mainly of neurologists and pain management and headache specialists. Journals and professional associations devoted to studying the spine, however, have not participated in this development. This is unfortunate, because the majority of spinal pain syndromes are managed by clinicians who treat the spine rather than those who treat headaches.
This problem of headaches related to the cervical spine cannot be underestimated. Up to 80% of patients with cervical acceleration-deceleration injuries report headaches within 2 months of injury. [1] Almost 25% of patients with this form of injury continue to have significant neck pain 2 years later, with the majority also complaining of headaches. [2] These figures do not by themselves confirm that the headaches noted in these studies originate from the cervical spine. Many patients with whiplash injuries to the neck are also under financial and litigation stresses, and their headaches may be the result of muscle tension. Furthermore, these patients commonly take medications with the potential of causing headaches. To make the issue more complicated, many of these patients have also had head injuries that may be the primary cause of their headaches. It is therefore not sufficient to assume that patients with complaints of both neck pain and headaches after injury have headaches that are being caused by the same pathology that is causing the neck pain. It is up to the clinician to be aware of the current literature in order to be able to make a reasonable diagnostic effort to differentiate between the various types of headache that may accompany neck pain.
This article is an attempt to assist the spine specialist in understanding the current literature on CGH. With this review it is hoped that a clinician will be able to discuss the current state of knowledge and be aware of the controversies concerning CGH, as well as place the multiple theories and treatment approaches for this condition in some perspective.
The literature search
A search was performed with three computerized medical databases (Medline, CINAHL, Mantis) for the terms “cervicogenic” and “headache” for the periods covered by each database (1966 for Medline, 1982 for CINAHL, 1880 for Mantis). The search was limited to articles in English, French, and German. Search results from the different databases were merged using reference-managing software, and duplicates were eliminated. The reference section of each article was then searched for relevant articles not uncovered by the computerized databases. Although no formal search strategy was attempted for books, theses, and presentation abstracts, these were included when articles uncovered by our search made reference to them. This strategy yielded 212 papers, some of which were not relevant to our review. These results encouraged us to pursue our original goal of reviewing the literature pertaining specifically to CGH rather than attempt to cover the much broader topic of headaches and neck pain. Because the term CGH was introduced in 1983, this search was mainly limited to papers published within the last two decades, although additional papers were added when relevant and important to the discussion. Although this may seem too restrictive, we thought that this type of review could reduce some of the confusion surrounding this topic by excluding older literature where it is impossible to determine if the authors are in fact describing CGH or a different condition.
The information gleaned from our literature review was divided into the following six categories for analysis: historical perspective; definition and diagnostic criteria; epidemiology; pathogenesis; differential diagnosis; and treatment.
Historical perspective

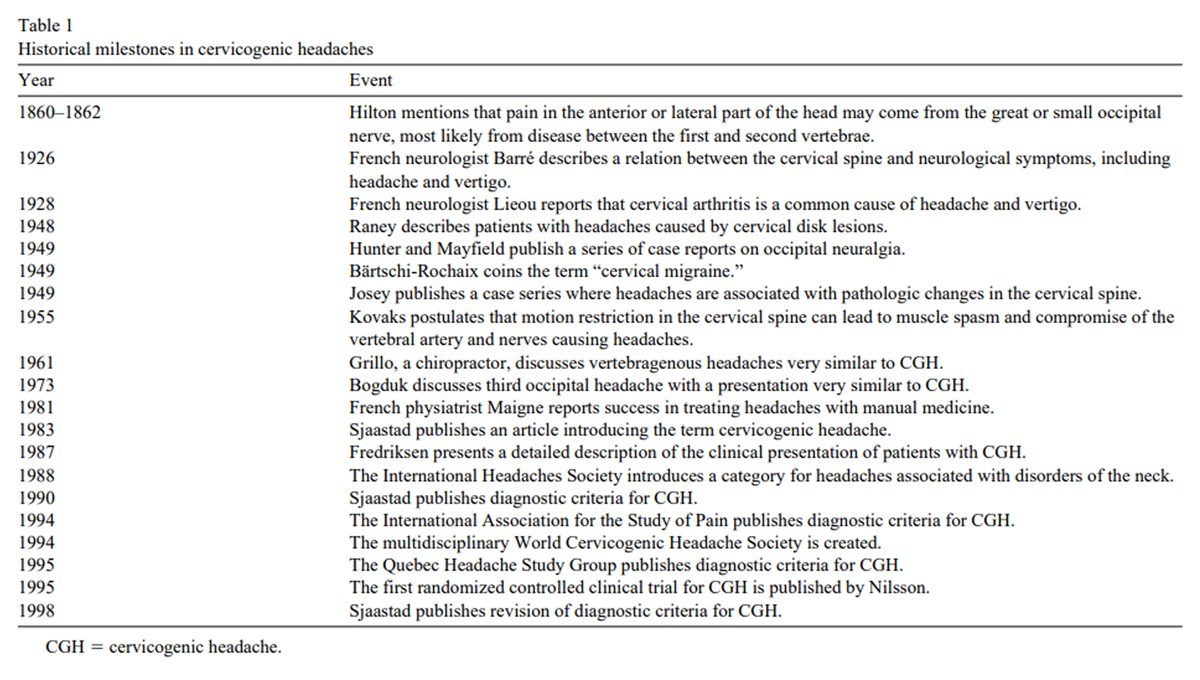
Table 1 Table 1 highlights some of the historical milestones in the evolution of the concept of CGH. The earliest reference we uncovered was a series of lectures given by Hilton in the period 1860–1862, as reported by Pearce. [3] In those lectures, Hilton proposed that pain in the anterior or lateral part of the head may come from the great or small occipital nerve, most likely from disease between the first and second vertebrae. Sixty years later, in 1926, Barré [4] hypothesized a relationship between the cervical spine and neurological symptoms, including headache and vertigo. His collaborator, Lieou [5], stated in 1928 that cervical arthritis should be considered a common cause of these symptoms. Twenty years later, Raney and Raney [6] reported that headache may be a common symptom of cervical disk lesions. The following year, a case series published by Hunter and Mayfield [7] reported that occipital neuralgia, where pain radiated from the occiput to the periorbital and jaw areas, could be an important cause of headaches. This theory, in turn, was used to justify the injection of analgesics into the occipital nerves in an attempt to relieve these headaches. Also in 1949, Bärtschi-Rochaix [8] used the term “cervical migraine” to describe headaches presumed to come from the neck, while Josey [9] published a case series on patients with headaches associated with pathologic changes in the cervical spine. In 1955 Kovacs [10] wrote that motion restriction in the cervical spine could lead to muscle spasm and compromise of the vertebral artery and nerves, causing headaches. This helped popularize osteopathic, chiropractic, and manual treatment of the cervical spine to relieve headaches. Maigne [11] was a prominent advocate of using manipulation to treat headaches, while Bogduk and Marsland [12] advocated surgical intervention to treat what they termed “3rd occipital headache”.
The term “cervicogenic headache” was first introduced to the medical literature in 1983 by Sjaastad et al. [13], who described patients with a headache not classified by diagnostic criteria at that time. In 1987 Fredriksen et al. [14] gave a more detailed description of patients they had diagnosed with CGH. In 1988 the International Headache Society (IHS) [15] amended its diagnostic classification system to include a category for headaches associated with disorders of the neck. In 1990 Sjaastad et al. [16] published very specific and detailed diagnostic criteria for CGH. This was followed by the publication of less stringent diagnostic criteria for CGH by the International Association for the Study of Pain (IASP) in 1994, and by the Quebec Headache Study Group in 1995. [11, 17] In 1998, Sjaastad et al. [18] revised their diagnostic criteria for CGH based on more extensive clinical research.
Definition and diagnostic criteria
Table 2
Table 3
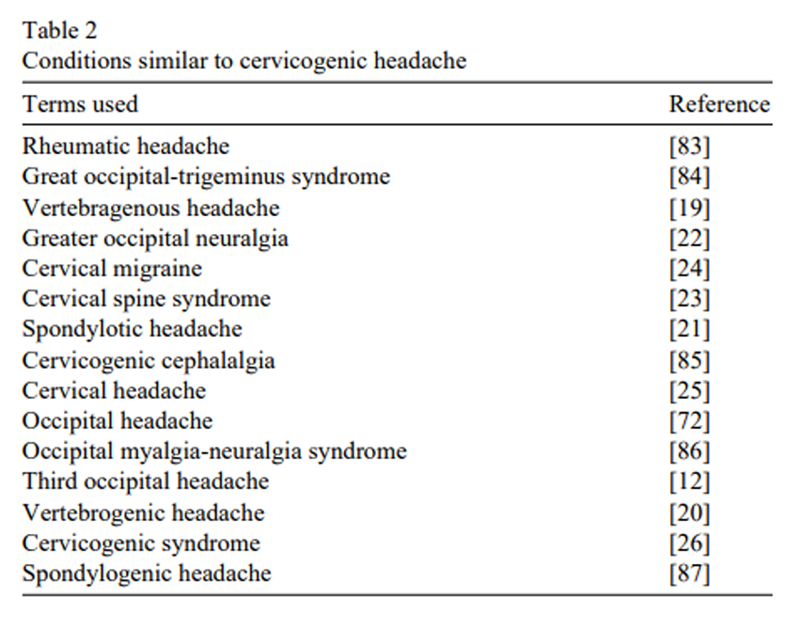
page 4The term CGH, although adopted by a number of organizations, is not universally accepted, and there remains a great deal of variation in the terminology used to discuss headaches associated with disorders of the cervical spine. This is especially true of literature before 1983, when a number of terms (Table 2) appear to have referred to the same clinical entity. Many of these terms, such as vertebragenous [19], vertebrogenic [20], or spondylotic [21] headaches, can be considered synonymous with CGH, at least in their connotation. Such terms as neuralgia, especially those referring to a specific nerve, assume, with little evidence, that the origin of the headache is known. [12, 22] Other terms are more vague, referring simply to a syndrome or a specific location of the headache. [23–26]
The confusion seen in CGH terminology is also apparent when examining the diagnostic criteria for CGH. Table 3 summarizes the prominent features of the diagnostic criteria published by various expert groups. The most widely used diagnostic criteria for many years were those proposed by Sjaastad [16] in 1990 and subsequently updated in 1998. [18] Although the publication of these criteria brought focus to the field of CGH research, certain aspects have proved difficult to embrace. For example, Sjaastad vigorously advocated the position that these headaches should be strictly unilateral, whereas others have accepted that these headaches may be unilateral or bilateral. Sjaastad also included a number of accompanying symptoms, such as nausea, vomiting, flushing, dizziness, phono- and photophobia, blurred vision, and dysphagia, making his criteria too specific and detailed for general practice.
Lack of consensus is also evident in the criteria of the three other main expert groups. For example, the IHS included radiological abnormalities in their diagnostic criteria, despite a failure to identify radiographic abnormalities specific to CGH. [15, 27] The IASP and WCHS focused their attention on the relief of pain by the injection of analgesics into cervical structures with no convincing clinical trials to support this position and no consensus regarding the various injection techniques. [17, 28]
Despite these differences, certain features are common to the majority of the diagnostic criteria for CGH. There is agreement that these headaches start in the neck or occipital area and can then spread to other areas of the head, including the frontal, temporal, and periorbital regions. The pain tends to be dull, nonthrobbing, and nonlancinating, and can become moderate to severe in intensity. Examination reveals tenderness and abnormal palpatory findings in the cervical paraspinal tissues, as well as possible decreased cervical range of motion. The other reported findings and characteristics of CGH appear to be less well defined.
Epidemiology
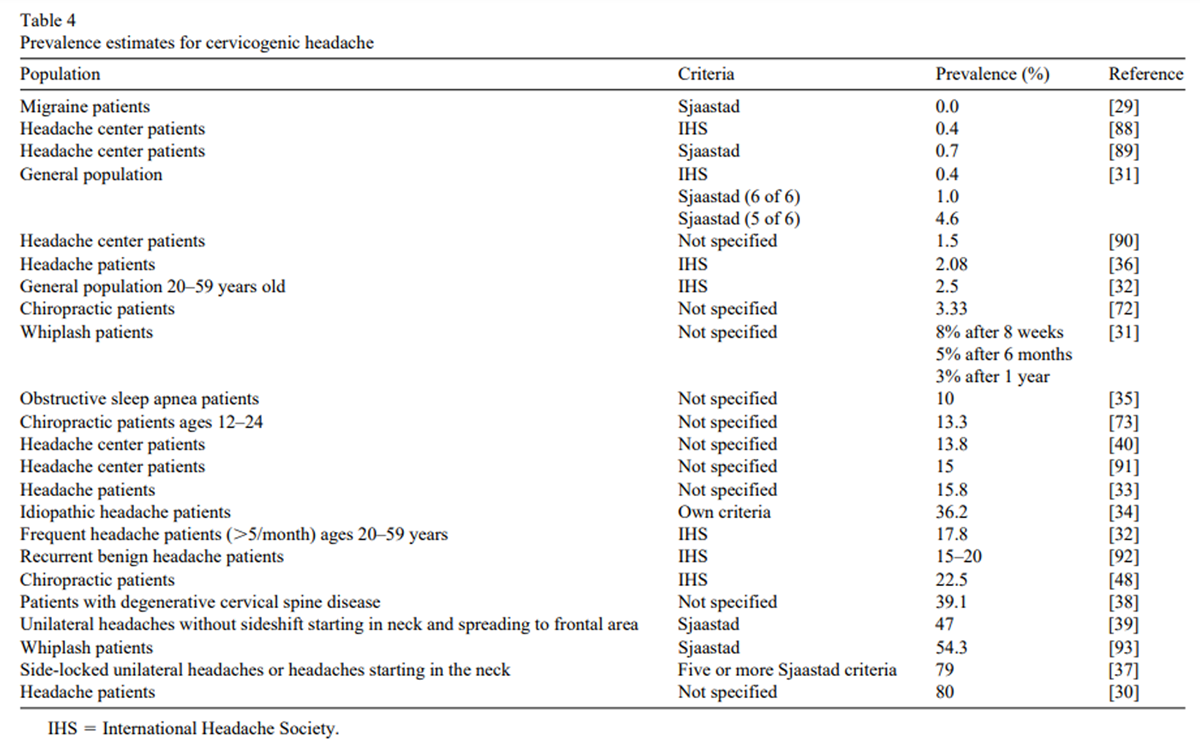
Table 4 There is a great deal of variation in the perceived prevalence of CGH. The published prevalence rate estimates uncovered through our literature search are presented in Table 4. These ranged from 0% of patients with migraine headache (MH) [29] to 80% of patients with headache. [30] There are several reasons for this wide range of published estimates, including vastly different populations of subjects. In the general population, for example, prevalence rates ranged from 0.4% to 2.5% [31, 32], whereas studies looking at all patients with a complaint of headache reported estimates of 15% to 20%. [15, 32–34] The highest variation was among headache center patients, with prevalence estimates of 0.4% to 80%. Part of this variation can be attributed to the different methodology used in these studies (i.e., prospective cohort, retrospective analysis, etc.), as well the different diagnostic criteria used to define CGH. Several studies did not specify the criteria used to define CGH, making direct comparisons impossible; even studies using the same criteria varied in the stringency with which these were applied (i.e., patient must fulfill a minimum of x criteria to be included). The study reporting the highest prevalence for CGH was by Rothbart [30], a clinician from a pain management center, who estimated that 80% of the patients with headache in his clinic had CGH. As founder of the WCHS, he may have spent considerably more time than other physicians in seeking patients with this syndrome. An incidental finding in a study by Loh et al. [35] reported that 10% of patients with obstructive sleep apnea were diagnosed with CGH, although no explanation was offered as to the mechanism of action.
Analysis of patient descriptive data (age, gender, etc.) from studies where such information was given reveals that patients with CGH appear to form a fairly homogeneous population, with a mean age of 42.9 years, a gender distribution that is 79.1% female and 20.9% male, and a mean duration of symptoms of 6.8 years. More detailed demographic data were found in a study by Shah and Nafee [36] in India, where patients with CGH were described as 43% urban and 57% rural, with 55.7% employed as handicraft workers, 28.3% as laborers, 10.0% as clerks, 4.9% as business executives, and 1.6% as doctors. Shah and Nafee speculated that the poor ergonomics associated with the handicraft occupations may account for the higher prevalence in that group. They also reported that the population in his study had a mean age of onset of 62.5 years for CGH, which is considerably older than the mean age of typical patients with CGH reported above.
Another factor influencing prevalence rates in headache centers is the apparent overlap between the diagnosis of CGH, tension-type headache (TTH), and common migraine headache. Bono et al. [37] report that 75% of patients fulfilling IHS criteria for MH also meet most of the criteria for CGH. Furthermore, the CGH diagnostic criteria by Sjaastad et al. [16] include many of the systemic symptoms, such as nausea, vomiting, phonophobia, and photophobia commonly seen in MH. CGH also appears to frequently co-exist with primary headache disorders such as MH and TTH. One study of headache center patients reported that whereas only 16.1% were diagnosed with CGH, an additional 20.1% were diagnosed with both MH and CGH, for a total prevalence of 36.2% [34]. A recent study of patients with neck injuries reported that 34.3% had CGH, whereas an additional 11.4% had both CGH and MH, and an additional 8.6% had CGH in combination with headaches associated with the neck, for a total prevalence of 54.3%. [38] The reason for distinguishing CGH from headaches associated with the neck was unclear. When narrowing the field among patients with headache to those with unilateral pain without sideshift and pain starting from the neck and spreading to the oculofrontal area, Bono et al. [39] diagnosed 47% of such patients with CGH, including 15% where there was overlap between MH and headaches associated with the neck, although again the distinction of the latter from CGH was unclear. Another study reported that 56.4% of CGH diagnoses occur in combination with other headaches, including MH, TTH, and drug-induced headache. [40] Although Sjaastad has tended to disagree that CGH symptoms are commonly found in patients with MH, he and Bovim [41] reported on four patients where both MH and CGH co-existed. These patients were able to distinguish between episodes of each headache, reporting improvement of MH but not CGH with sumatriptan and ergotamine, and relief of CGH but not MH with greater occipital nerve anesthetic blockade.
Pathogenesis
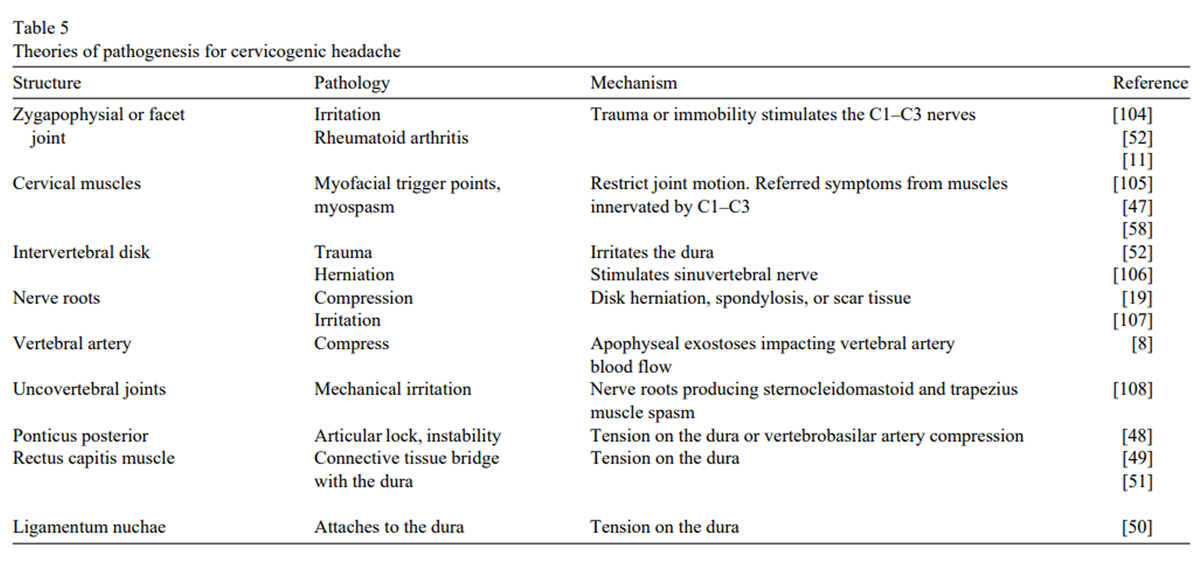
Table 5 One of the most controversial areas within the CGH literature is the discussion of its cause. Almost every structure and pathology within the cervical spine has been implicated as a cause of these headaches. Table 5 summarizes the structures suggested as the origin of CGH and the types of pathology associated with these headaches. The rationale for most of the theories is the observation, usually in a small number of cases, of either a reproducible finding on clinical examination, a response to stimulation of the structure, or relief of symptoms after treatment directed at the structure. Examples include the response of patients to surgery for disk disease [42], injections of posterior facets with anesthesia [43], and injections of cervical muscles with botulinum toxin. [47]
One theory of CGH etiology comes from anatomical studies showing an attachment of the suboccipital tissues to the dura mater at the cervical–cranial junction, and the observation that mechanical traction on these tissues can cause movement of the dura. [48–51] The rectus capitus posterior minor muscle [51] and ligamentum nuchae [60] have been shown to have direct connections to the suboccipital dura on very delicate dissection in a small number of cadavers. This suggests a role for the dura as a nociceptive structure in CGH.
Figure 1
page 7Structures implicated in the genesis of CGH all have their sensory innervations through the upper cervical and midcervical nerve roots, which lead to the cervical cord and converge within the spinal tract of the trigeminal nucleus [49] (Figure 1). This allows nociceptive input from cervical structures to be perceived as head pain, including pain to the temporal, frontal, and orbital regions. This convergence may also help to explain the systemic and sympathetic nervous system features accompanying CGH. Studies showing relief of headache after lower nerve root blocks have cast a doubt on whether only the upper nerve roots are significant in CGH. [43, 44]
Martelletti has reported increased levels of pro-inflammatory cytokines interleukin-I β and tumor necrosis factor-α during mechanically induced attacks of CGH; these were significantly higher than in patients with MH. [45, 46] He postulated that this could represent a specific signal from the immune system to activate such pain-producing agents as substance P and calcitonin-gene–related peptide. This may help define CGH as an inflammatory consequence of cervical trauma, explaining the wide variety of pathological processes in different structures that can cause similar headaches.
The inability to find a definitive structure or pathology as the cause of CGH has lead some to believe that CGH does not represent a single pathological entity but rather a pain syndrome resulting from the nociceptive stimulation of almost any structure in the cervical spine. [52]
Differential diagnosis
The differential diagnosis stressed in most of the literature on this topic is between CGH, MH, and TTH. It is generally assumed that intracranial pathology from infection, neoplasm, trauma, and so forth has been ruled out. Headaches associated with sinusitis, temporomandibular joint syndrome, visual or auditory disturbances, and cluster headache are rarely confused with CGH, because each possesses unique distinguishing characteristics. To aid the task of differential diagnosis, several studies have reported the results of various radiographic, neurologic, and physiologic testing in patients with CGH.
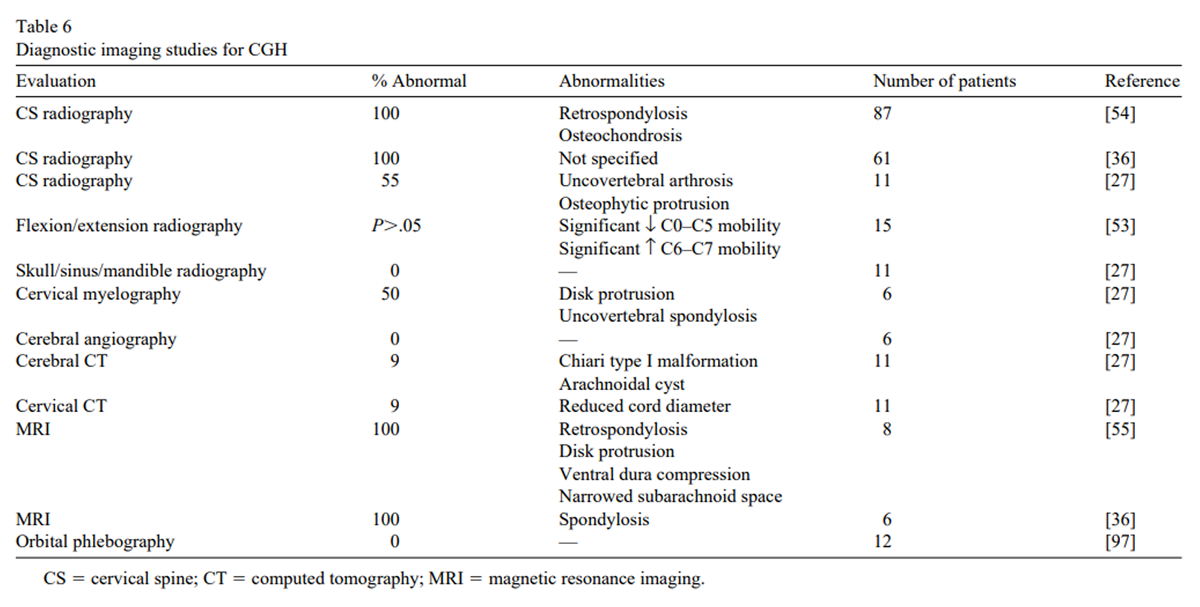
Table 6 The significance of radiological findings in CGH has been difficult to establish (Table 6). Only one of these studies used a control group [53], and most had a small number of subjects. These shortcomings make it difficult to draw conclusions regarding the relationship of radiological findings and CGH. Although degenerative changes have been found in patients with CGH on plain film radiography and magnetic resonance imaging scans of the cervical spine, these changes cannot be considered specific and unique to CGH. [27, 36, 54, 55] A study by Jansen [54] in 1998 found that 100% of patients with CGH had radiographic evidence of retrospondylosis and osteochondrosis. With multiple spinal levels involved (42.9% at C5–C6, 22.7% at C4–C5, 21.4% at C6–C7, 11.0% at C3–C4, 0.6% at C7–T1, and only 1.3% at C2–C3), it is difficult to assess the importance of this finding. The description of Chiari type 1 malformations and spinal cord compression in small numbers of patients with characteristics of CGH may simply represent pathology that causes headaches by stimulating cervical structures rather than a finding specific to CGH.
Table 7
page 9Table 7 summarizes the results of various diagnostic tests on patients with CGH. Although many of these studies report statistically significant findings, the number of subjects is too small to reach any conclusion. Many of the physiological tests, such as sweating patterns [56] and electronystagmography [57], are so esoteric that it is difficult to determine their significance or relevance in clinical practice. The finding of various forms of muscle dysfunction, such as myofascial trigger points [58], responses of different muscle groups to mental stress [59], and cervical muscle strength and endurance [60], seems to confirm the involvement of cervical and paraspinal muscles in CGH. The lack of response to common vasoactive medications used in MH [61] argues against arterial involvement in CGH and can be one of the clues that a patient may have a CGH.
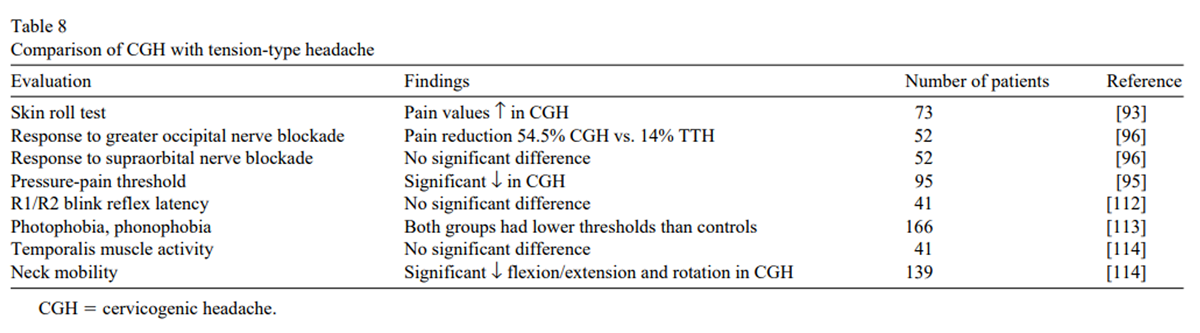
Table 8
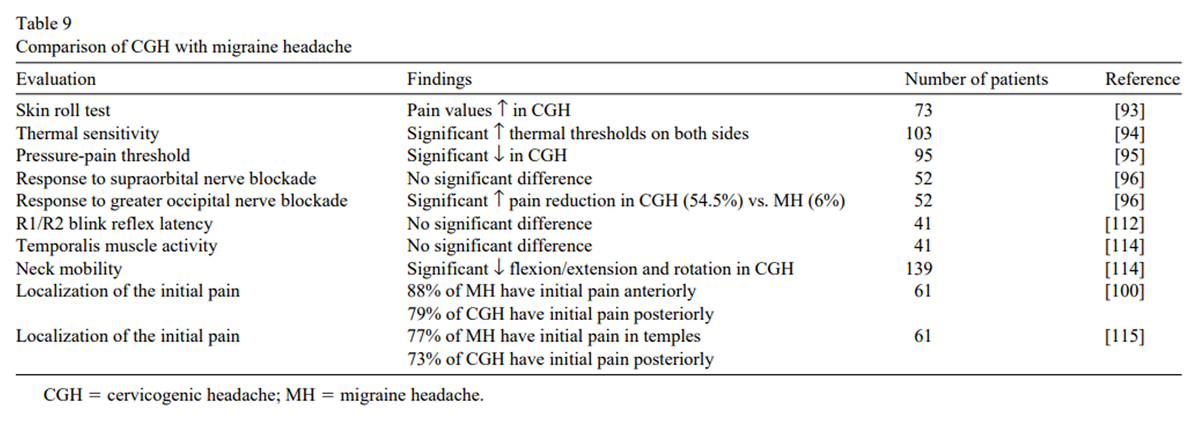
Table 9 Attempts to differentiate CGH from MH and TTH on the basis of some clinical or experimental measure are presented in Tables 8 and 9. It does not appear that any specific test or clinical finding can be used to define patients with CGH. A detailed clinical history is therefore imperative in order to diagnose CGH. The difficulties of diagnosing CGH were stressed by Sjaastad and Bovim in 1991 [41], when they compared CGH with MH and reported that CGH fulfilled seven of eight common MH criteria (the exception being aggravation by physical activity). Nausea and/or vomiting was reported in 55% of patients with CGH versus 70% to 85% for MH. Photophobia was reported in 45% of patients with CGH versus 88% of patients with MH. Patients with MH, however, did not fulfill the most important criteria for CGH, that is, precipitation of headaches with neck movements and/or external pressure on the neck. A second study by Sjaastad et al. [63] in 1992 compared pain patterns in CGH and MH and reported that whereas typical MH attacks were unilateral without side shift (the typical CGH pattern) in only 16% of patients, 75% of nontypical MH attacks presented in this fashion. Their group of patients with CGH fulfilled only 3.79 of 7 IHS criteria for common MH criteria, compared with 6.78 for patients with MH.
A study by Vincent and Luna in 1999 [62] examined the number of patients with CGH, TTH, and MH who could fulfill Sjaastad’s criteria for CGH. Patients with CGH met 10.51 of 18 criteria versus 3.85 for patients with MH and 4.89 for patients with TTH, a statistically significant difference. One third (33.3%) of patients with CGH met the IHS criteria for MH, whereas only 3.3% of patients with CGH met IHS criteria for TTH. In other words, 63.4% of patients with CGH could not be classified according to IHS criteria as having either MH or TTH. D’Amico et al. [64] similarly examined the characteristics of patients with headache and reported that in patients with long-lasting, side-locked, unilateral pain, the diagnosis was MH in 85.1%, TTH in 10.8%, and CGH in 4.1%. The percentage of patients with headache in whom the pain was localized in the occipitonuchal region was 100% in CGH, 12.5% in MH, and 20.0% in TTH. Conversely, the percentage of patients in whom the initial pain was nonoccipital was 0% in CGH, 76.6% in MH, and 30.0% in TTH. CGH may then be differentiated from MH and TTH by a pattern of unilateral pain without sideshift, with the initial pain located in the occipital area, and failure to be classified by diagnostic criteria for other headaches.
Treatment
Table 10
page 10The type of treatment recommended to patients with CGH appears more dependent on the specialty of the treating physician than the science or research supporting it. The four treatment options generally recommended are surgery for a number of pathological entities; cervical spine manipulation; injections of various cervical structures with a variety of agents; and medication. The published literature in support of surgical intervention for CGH is listed in Table 10. The main criticisms of this literature are the small sample sizes, the marked variation in the surgical procedures used, the difference in the structures being operated on, the poor documentation of the criteria used for diagnosing CGH, and the lack of standardized outcome measures in the majority of these studies.
For example, a number of papers on radiofrequency neurotomy report some improvement of symptoms in 71% to 83% of patients and complete relief in 7% to 43% of patients. [65–69] The authors, however, reported the ablation of different nerves in these studies, making it difficult to reach conclusions or compare the results. A number of papers on various decompression procedures report relief of headaches in a substantial number of patients but again have not used a standardized protocol. [55, 70] The remaining papers on surgery consist mainly of isolated case reports. There are no controlled studies to support the use of any surgical procedure for the management of CGH, and current justification for surgery appears to be based solely on the anecdotal experience of the surgeon.
Table 11
page 11As mentioned above, the prevalence of CGH ranges from 3.3% to 22.5% of chiropractic patients, indicating the frequency with which these headaches are treated with manipulation. [48,72,73] A survey of primary care physicians in Australia reported that 69% of them agreed that referral to a chiropractor was appropriate for headache provoked by head/neck postures. [71] The results of studies on cervical manipulation for CGH are listed in Table 11. The results from the case series are similar to those reported after surgery but suffer from the same shortcomings. However, there are more randomized controlled trials on manipulation than any other treatment for CGH. The studies by Nilsson et al. [74, 75] have been the most rigorous and demonstrated that spinal manipulation was more effective, in the short term, than massage in reducing the frequency and severity of headaches and the amount of analgesic use by patients.
A study by Howe et al. [76] indicated that the addition of one cervical manipulation to nonsteroidal anti-inflammatory drug (NSAID) therapy was superior to NSAID therapy alone immediately after treatment, but this difference was lost at 3 weeks posttreatment. Bitterli et al. [21] found an advantage for cervical manipulation compared with mobilization and controls after 3 weeks of treatment, but the differences did not reach statistical significance. In an effect size analysis of randomized controlled trials on manipulation, Bronfort [77] concluded that there is moderate evidence of efficacy of cervical manipulation in the management of CGH. Similar conclusions have been reached in qualitative analyses by Hurwitz et al. [78] and Coulter et al. [79]
Table 12
page 12
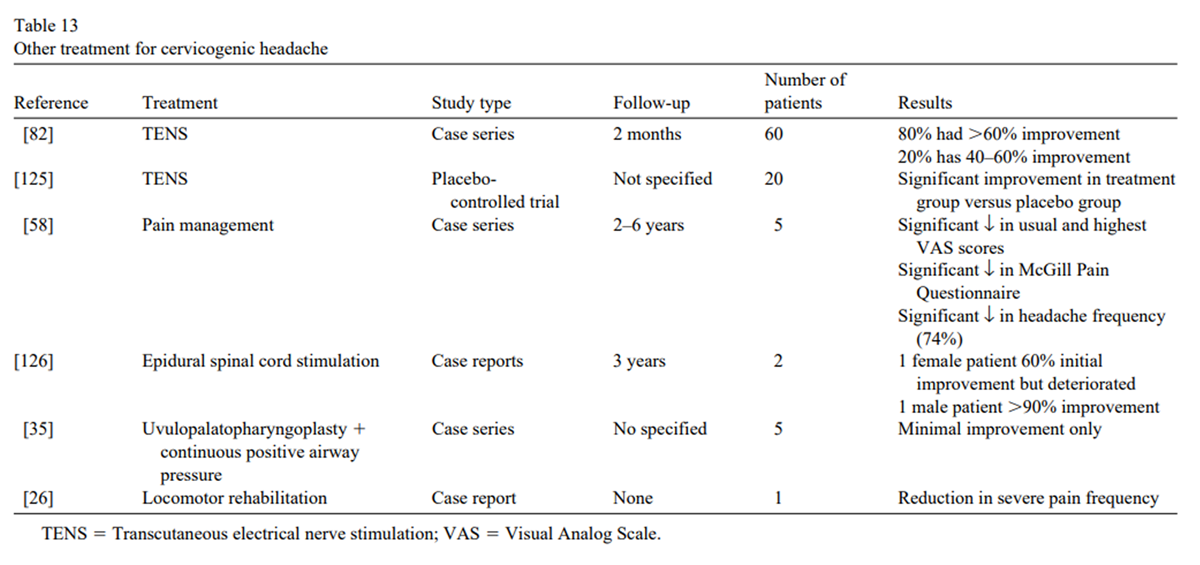
Table 13 Another common treatment approach for CGH is therapeutic injections. The results of injection of various agents and anesthetics on CGH are listed in Table 12. There are a number of small case series on the injection of the occipital nerves where short-term improvement of was noted in 50% to 90% of patients. [34, 43, 54] Again, these studies suffer from the same shortcomings as those on surgery and manipulation, and many reported only immediate postinjection results with no follow-up period. One study [34] compared lignocaine, lignocaine with methylprednisolone, and methylprednisolone alone in a nonrandomized case series and found that methylprednisolone was less effective than lignocaine and did not add anything to the injection of lignocaine alone.
This finding does not support Martelletti’s theory about the role of inflammation in CGH. [45, 46] Two relatively good cohort studies on the injection of sterile water and saline into tender points in cervical muscles failed to show any improvement of symptoms. [80] A small case series on epidural corticosteroid injection reported some degree of relief. [84] One intriguing study was a randomized controlled trial comparing botulinum toxin with saline injection into the cervical paraspinal muscles, which found a significant decrease in pain and increased cervical spine range of motion in the botulinum group. [47]
Among other treatments for CGH (Table 13) we found one randomized controlled trial on the use of transcutaneous electrical nerve stimulation [85] suggesting slight temporary relief of symptoms. There were no significant studies that we could find on the use of medication for CGH. Where medications have been discussed, there has been the suggestion that CGH is relatively unresponsive to most medications commonly used to treat other forms of headache. Although other treatments, including massage, biofeedback, exercise, or nutrition, are commonly used to treat other headaches, including TTH, no studies were found on their use for CGH.
Conclusions
Despite a growing body of literature on CGH and an increasing acceptance that headaches can originate from the cervical spine, there remains considerable controversy and confusion concerning all aspects of this topic. However, a number of comments on CGH appear quite reasonable. The concept that headaches can originate from the neck is not new. The pain appears to be generated by irritation of nociceptors from structures in the cervical spine and may accompany injury and pathology in the neck. These headaches are difficult to differentiate from MH and TTH, although they possess the distinguishing characteristics of being triggered by neck movements, pain spreading to the occipital region, tenderness in the suboccipital tissues, decreased cervical range of motion, and unresponsiveness to typical headache medication.
The significance of radiological findings and advanced diagnostic testing is unclear. Evidence to support treatment with surgery and injections consists mainly of case series without controls or standardized follow-up. The only treatment approach supported by a reasonable body of controlled trials is cervical manipulation, but this is by no means conclusive.
Until additional research and improved consensus on the topic of CGH becomes available, it is essential that any clinician maintain an open, cautious, and critical approach to the literature. At this point, the clinician must be wary of enthusiastic and dogmatic claims concerning CGH. As the literature on this topic grows in volume and quality, the debate will intensify and hopefully result in the clarification of the cause, diagnosis, and treatment of CGH.
References:
Maimaris C, Barnes M, Allen M.
“Whiplash injuries” of the neck: a retrospective study.
Injury 1988;19(6):393–6.Balla J.
The late whiplash syndrome.
Aust N Z J Surg 1980;50(6): 610–4.Pearce JM.
Cervicogenic headache: an early description.
J Neurol Neurosurg Psychiatry 1995;58(6):698.Barré M.
Sur un syndrome sympathique cervical postérieur et sa cause fréquente:
l’arthrite cervicale.
Rev Neurol (Paris) 1926;33: 1246–8.Lieou Y.
Syndrome sympathétique cervical postérieur et arthrite
chronique de la colonne vertébrale cervicale.
Thesis, University of Strasbourg 1928.Raney A, Raney R.
Headache: a common symptom of cervical disc lesions.
Arch Neurol Psychiat 1948;59:603–21.Hunter C, Mayfield F.
Role of the upper cervical roots in the production of pain in the head.
Am J Surg 1949;48:743–51.Bärtschi-Rochaix W.
Migraine cervicale, das encephale Syndrome nach Halswirbeltrauma.
Bern: Huber 1949.Josey A.
Headache associated with pathologic changes in cervical part of spine.
JAMA 1949;140:944–9.Kovacs A.
Subluxation and deformation of the cervical apophyseal joints:
a contribution to the etiology of headache.
Acta Radiol 1955; 43:1–16.Meloche J. Bergeron Y, Bellavance A, et al.
Painful intervertebral dysfunction: Robert Maigne’s original contribution
to headache of cervical origin. The Quebec Headache Study Group.
Headache 1993;33(6):328–34.Bogduk N, Marsland A.
On the concept of third occipital headache.
J Neurol Neurosurg Psychiatry 1986;49(7):775–80.Sjaastad O, Saunte C, Hovdahl H, et al.
“Cervicogenic” headache. An hypothesis.
Cephalalgia 1983;3(4):249–56.Fredriksen TA, Hovdal H, Sjaastad O.
“Cervicogenic headache”: clinical manifestation.
Cephalalgia 1987;7(2):147–60.IHS, Headache Classification Committee of the International Headache Society.
Classification and diagnostic criteria for headache disorders,
cranial neuralgias, and facial pain.
Cephalalgia 1988;8(Suppl 7):1–96.Sjaastad O, Fredriksen TA, Pfaffenrath V.
Cervicogenic headache: diagnostic criteria.
Headache 1990;30(11):725–6.Merskey H, Bogduk N. (eds.).
Classification of chronic pain. Descriptions of chronic pain
syndromes and definitions of pain terms.
Cervicogenic headache. 2nd ed. Seattle: IASP, 1994.Sjaastad O, Fredriksen TA, Pfaffenrath V.
Cervicogenic headache: diagnostic criteria. The Cervicogenic Headache International
Study Group. Headache 1998;38(6):442–5.Grillo F.
The differential diagnosis and therapy of headache.
Swiss Ann Chiroprac 1961;II:121–66.Vernon HT.
Spinal Manipulation and Headaches of Cervical Origin
Journal of Manipulative and Physiological Therapeutics 1989 (Dec); 12 (6): 455–468Bitterli J. Graf R, Robert F, et al.
Zur Objektivierung der manualtherapeutischen
Beeinflussbarkeit des spondylogenen Kopfschmerzes.
Nervenarzt 1977;48(5):159–62.Chouret E.
The great occipital neuralgia headache.
Headache 1967; 7(1):33–4.Hogan L, Beland I.
Cervical spine syndrome.
Am J Nurs 1976; 76(7):1104–7.Dutton C, Riley L.
Cervical migraine. Not merely a pain in the neck.
Am J Med 1969;47(1):141–8.Bogduk N, Corrigan B, Kelly P, et al.
Cervical headache.
Med J Aust 1985;143(5):202,206–7.Stevans JM.
The effects of remote locomotor rehabilitation in a
chronic cervicogenic syndrome: a case report.
Chiroprac Tech 1996; 8(3):121–4.Fredriksen TA, Fougner R, Tangerud A, et al.
Cervicogenic headache. Radiological investigations concerning head/neck.
Cephalalgia 1989;9(2):139–46.WCHS.
Taxonomical definition of cervicogenic headache.
www.cervicogenic.com/definit1.htm 1994.Leone M, D’Amico D, Moschiano F, et al.
Possible identification of cervicogenic headache among
patients with migraine: an analysis of 374 headaches.
Headache 1995;35(8):461–4.Rothbart P.
Cervicogenic headache: a pain in the neck.
Can J Diagnos 1996;13(2):64–6,71–6.Sjaastad O, Fredriksen TA.
Cervicogenic headache: criteria, classification and epidemiology.
Clin Exp Rheumatol 2000;18(2 Suppl 19):S3–6.Nilsson N.
The Prevalence of Cervicogenic Headache in a
Random Population Sample of 20-59 Year Olds
Spine (Phila Pa 1976) 1995 (Sep 1); 20 (17): 1884–1888Kränzlin P, Wälchli B.
The concept of cervicogenic headache.
Annual postgraduate course of the association of
Swiss chiropractors, vol. 13. Interlaken, Switzerland: 1993.Anthony M.
Cervicogenic headache: prevalence and response to local steroid therapy.
Clin Exp Rheumatol 2000;18(2 Suppl 19):S59–64.Loh NK, Dinner DS, Foldvary N, et al.
Do patients with obstructive sleep apnea wake up with headaches?
Arch Intern Med 1999; 159(15):1765–8.Shah PA, Nafee A.
Clinical profile of headache and cranial neuralgias.
J Assoc Physicians India 1999;47(11):1072–5.Bono G, Antonaci F, Ghirmai S, et al.
The clinical profile of cervicogenic headache as it emerges from a
study based on the early diagnostic criteria (Sjaastad et al. 1990).
Funct Neurol 1998;13(1):75–7.Bono G, Antonaci F, Ghirmai S, et al.
Whiplash injuries: clinical picture and diagnostic work-up.
Clin Exp Rheumatol 2000;18(2 Suppl 19):S23–8.Bono G, Antonaci F, Dario A, et al.
Unilateral headaches and their relationship with cervicogenic headache.
Clin Exp Rheumatol 2000; 18(2 Suppl 19):S11–5.Pfaffenrath V, Kaube H.
Diagnostics of cervicogenic headache.
Funct Neurol 1990;5(2):159–64.Sjaastad O, Bovim G.
Cervicogenic headache. The differentiation from common migraine. An overview.
Funct Neurol 1991;6(2):93–100.Fredriksen TA, Salvesen R, Stolt-Nielsen A, et al.
Cervicogenic headache: long-term postoperative follow-up.
Cephalalgia 1999; 19(10):897– 900.Bovim G, Berg R, Dale LG.
Cervicogenic headache: anesthetic blockades of cervical
nerves (C2–C5) and facet joint (C2/C3).
Pain 1992;49(3):315–20.Martelletti P, Di Sabato F, Granata M, et al.
Failure of long-term results of epidural steroid injection in cervicogenic headache [letter].
Eur Rev Med Pharmacol Sci 1998;2(1):10.Martelletti P, Stirparo G, Giacovazzo M, et al.
Proinflammatory cytokines in cervicogenic headache.
Funct Neurol 1999;14(3):159–62.Martelletti P.
Proinflammatory pathways in cervicogenic headache.
Clin Exp Rheumatol 2000;18(2 Suppl 19):S33–8.Freund BJ, Schwartz M.
Treatment of chronic cervical-associated headache
with botulinum toxin A: a pilot study.
Headache 2000;40(3):231–6.Wight S, Osborne N, Breen AC.
Incidence of ponticulus posterior of the atlas in migraine and cervicogenic headache.
J Manipul Physiol Ther 1999;22(1):15–20.Hack G.
Cervicogenic headache: new anatomical discovery provides the missing link.
Chiroprac Rep 1998;12(3):1–3.Mitchell BS, Humphreys BK, O’Sullivan E.
Attachments of the ligamentum nuchae to cervical posterior
spinal dura and the lateral part of the occipital bone.
J Manipul Physiol Ther 1998;21(3):145–8.Alix ME, Bates DK.
A Proposed Etiology of Cervicogenic Headache: The Neurophysiologic
Basis and Anatomic Relationship Between the Dura Mater
and the Rectus Posterior Capitis Minor Muscle
J Manipulative Physiol Ther 1999 (Oct); 22 (8): 534–539Bogduk N.
The anatomical basis for cervicogenic headache.
J Manipul Physiol Ther 1992;15(1):67–70.Pfaffenrath V, Dandekar R, Mayer ET, et al.
Cervicogenic headache: results of computer-based measurements
of cervical spine mobility in 15 patients.
Cephalalgia 1988;8(1):45–8.Jansen J, Vadokas V, Vogelsang JP.
Cervical peridural anaesthesia: an essential aid for the indication
of surgical treatment of cervicogenic headache triggered by
degenerative diseases of the cervical spine.
Funct Neurol 1998;13(1):79–81.Jansen J.
Laminoplasty—a possible treatment for cervicogenic headache?
Some ideas on the trigger mechanism of CeH.
Funct Neurol 1999;14(3):163–5.Fredriksen TA.
Cervicogenic headache: the forehead sweating pattern.
Cephalalgia 1988;8(3):203–9.Dieterich M, Pollmann W, Pfaffenrath V.
Cervicogenic headache: electronystagmography, perception of verticality
and posturography in patients before and after C2-blockade.
Cephalalgia 1993;13(4): 285–8.Jaeger B.
Are “cervicogenic” headaches due to myofascial pain and cervical spine dysfunction?
Cephalalgia 1989;9(3):157–64.Bansevicius D, Sjaastad O.
Cervicogenic headache: the influence of mental load on
pain level and EMG of shoulder-neck and facial muscles.
Headache 1996;36(6):372–8.Treleaven J, Jull G, Atkinson L.
Cervical musculoskeletal dysfunction in post-concussional headache.
Cephalalgia 1994;14(4): 257,273–9.Bovim G, Sjaastad O.
Cervicogenic headache: responses to nitroglycerin,
oxygen, ergotamine and morphine.
Headache 1993;33(5): 249–52.Vincent MB, Luna RA.
Cervicogenic headache: a comparison with migraine and tension-type headache.
Cephalalgia 1999;19(Suppl 25):11–6.Sjaastad O, Bovim G, Stovner LJ.
Laterality of pain and other migraine criteria in common migraine.
A comparison with cervicogenic headache.
Funct Neurol 1992;7(4):289–94.D’Amico D, Leone M, Bussone G.
Side-locked unilaterality and pain localization in long-lasting headaches:
migraine, tension-type headache, and cervicogenic headache.
Headache 1994;34(9):526–30.Blume HG.
Treatment of cervicogenic headaches: radiofrequency neurotomy to the
sinuvertebral nerves to the upper cervical disc and to the outer
layer of the C3 nerve root or C4 nerve root respectively.
Funct Neurol 1998;13(1):83–4.Blume HG.
Cervicogenic headaches: radiofrequency neurotomy and
the cervical disc and fusion.
Clin Exp Rheumatol 2000;18(2 Suppl 19):S53–8.Sjaastad O, Stolt-Nielsen A, Blume H, et al.
Cervicogenic headache. Long-term results of
radiofrequency treatment of the planum nuchale.
Funct Neurol 1995;10(6):265–71.van Suijlekom HA, van Kleef M, Barendse GA, et al.
Radiofrequency cervical zygapophyseal joint neurotomy for
cervicogenic headache: a prospective study of 15 patients.
Funct Neurol 1998; 13(4):297–303.van Suijlekom HA, Weber WE, van Kleef M, et al.
Radiofrequency cervical zygapophyseal joint neurotomy for
cervicogenic headache: a short term follow-up study.
Funct Neurol 1998;13(1):82–3.Jansen J.
Surgical treatment of non-responsive cervicogenic headache.
Clin Exp Rheumatol 2000;18(2 Suppl 19):S67–70.Jamison J.
Chiropractic referral: in search of criteria upon which
medical practitioners agree to refer for chiropractic care.
Chiroprac J Austral 1995;25(1):13–18.Droz J, Crot F.
Occipital headaches.
Swiss Ann Chiroprac 1985.; VIII.Ebrall P.
A description of 320 chiropractic consultations by Australian adolescents.
Chiroprac J Austral 1994;24(1):4–8.Nilsson N.
A Randomized Controlled Trial of the Effect of Spinal Manipulation
in the Treatment of Cervicogenic Headache
J Manipulative Physiol Ther. 1995 (Sep); 18 (7): 435—440Nillson N, Christensen HW, Hartvigsen J.
The Effect of Spinal Manipulation in the Treatment
of Cervicogenic Headache
J Manipulative Physiol Ther 1997 (Jun); 20 (5): 326–330Howe D, Newcombe R, Wade M.
Manipulation of the cervical spine—a pilot study.
J R Coll Gen Pract 1983;33:574–9.Bronfort G.
Efficacy of manual therapies of the spine.
Kopenhagen: Vrije Universiteit, 1997.Hurwitz EL, Aker PO, Adams AH, Meeker WC, Shekelle PG.
Manipulation and Mobilization of the Cervical Spine:
A Systematic Review of the Literature
Spine (Phila Pa 1976) 1996 (Aug 1); 21 (15): 1746–1760Coulter, I, Hurwitz, E, Adams, A et al.
The Appropriateness of Manipulation and Mobilization
of the Cervical Spine PDF
Santa Monica, CA: RAND Corporation; 1996 Document No. MR-781-CR.Sand T, Bovim G, Helde G.
Intracutaneous sterile water injections do not relieve pain in cervicogenic headache.
Acta Neurol Scand 1992;86(5):526–8.Martelletti P, Di Sabato F, Granata M, et al.
Epidural corticosteroid blockade in cervicogenic headache.
Eur Rev Med Pharmacol Sci 1998(1):31–6.Farina S, Granella F, Malferrari G, et al.
Headache and cervical spine disorders: classification and
treatment with transcutaneous electrical nerve stimulation.
Headache 1986;26(8):431–3.Cyriax J.
Rheumatic headache.
Br Med J 1938;2:1367–8.Skillern P.
Great occipital trigeminus syndrome as revealed by induction block.
Arch Neurol Psychiatry 1954;72:335–40.Mannen E.
The use of cervical radiography overlays to assess response
to manipulation: a case report.
J Can Chiroprac Assoc 1980; 24(3):108–10.Blume H, Atac M, Golnick J.
Neurosurgical treatment of persistent occipital mylagia-neuralgia syndrome.
In: Pfaffenrath V, Lundberg P, Sjaastad O, eds. Updating in headache.
Berlin: Springer-Verlag, 1985:24–34.Pollmann W, Keidel M, Pfaffenrath V.
Headache and the cervical spine: a critical review.
Cephalalgia 1997;17(8):801–16.Leone M, D’Amico D, Grazzi L, et al.
Cervicogenic headache: a critical review of the
current diagnostic criteria.
Pain 1998;78(1):1–5.Manzoni G, Zanferrari C, Cavallini A, et al.
Cervicoalgia e cefalee: rilievi clinico-epidemiologici.
In: Ruju A, Nappi G, eds. Cefalee cervicogenetiche.
Confinia cephalalgica, vol. 12. Milan, Italy:
Cluster Press, 1990:25–33.Drottning M, Staff P, Sjaastad O.
Cervicogenic headache after whiplash injury [abstract].
Cephalalgia 1997;17:288–9.Olesen JE.
Classification and diagnostic criteria for headache disorders,
cranial neuralgias and facial pain.
1st ed. Copenhagen: International Headache Society, 1990.Greiner-Perth R. Neubauer U, Bohm H.
[The cervicogenic headache from the spinal surgery
point of view—a pilot study] (German).
Der Schmerz 1999;13(6):398–402.Bansevicius D, Pareja JA.
The “skin roll” test: a diagnostic test for cervicogenic headache?
Funct Neurol 1998;13(2):125–33.Becser N, Sand T, Pareja JA, et al.
Thermal sensitivity in unilateral headaches.
Cephalalgia 1998;18(10):657,675–83.Bovim G.
Cervicogenic headache, migraine, and tension-type headache.
Pressure-pain threshold measurements.
Pain 1992;51(2):169–73.Bovim G, Sand T.
Cervicogenic headache, migraine without aura and tension-type headache.
Diagnostic blockade of greater occipital and supra-orbital nerves.
Pain 1992;51(1):43–8.Bovim G, Jenssen G, Ericson K.
Orbital phlebography: a comparison between cluster headache and other headaches.
Headache 1992; 32(8):408–12.Pikus HJ, Phillips JM.
Outcome of surgical decompression of the second cervical root
for cervicogenic headache.
Neurosurgery 1996; 39(1):63–71.Sand T, Zwart JA, Helde G, et al.
The reproducibility of cephalic pain pressure thresholds
in control subjects and headache patients.
Cephalalgia 1997;17(7):748–55.Sjaastad O, Bovim G, Stovner LJ.
Common migraine (“migraine without aura”):
localization of the initial pain of attack.
Funct Neurol 1993;8(1):27–32.Stovner LJ.
Headache associated with the Chiari type I malformation.
Headache 1993;33(4):175–81.Vincent MB, Luna RA, Scandiuzzi D, et al.
Greater occipital nerve blockade in cervicogenic headache.
Arq Neuropsiquiatr 1998;56(4): 720–5.Seaman DR, Winterstein JF:
Dysafferentation: A Novel Term to Describe the Neuropathophysiological
Effects of Joint Complex Dysfunction. A Look at Likely
Mechanisms of Symptom Generation
J Manipulative Physiol Ther 1998 (May); 21 (4): 267-280Jull G, Barrett C, Magee R, et al.
Further clinical clarification of the muscle dysfunction
in cervical headache.
Cephalalgia 1999;19(3): 179–85.Michler RP, Bovim G, Sjaastad O.
Disorders in the lower cervical spine. A cause of unilateral headache?
A case report.
Headache 1991;31(8):550–1.Jansen J, Bardosi A, Hildebrandt J, et al.
Cervicogenic, hemicranial attacks associated with vascular
irritation or compression of the cervical nerve root C2.
Clinical manifestations and morphological findings.
Pain 1989;39(2):203–12.Seletz E.
Headache of extracranial origin.
CA Med 1958;89:314–9.Fredriksen TA, Wysocka-Bakowska MM, Bogucki A, et al.
Cervicogenic headache. Pupillometric findings.
Cephalalgia 1988;8(2):93–103.Mihoglu H, Inan LE, Uysal H, et al.
Brain stem reflexes in cervicogenic headaches.
Funct Neurol 1998;13(1):87.Hinderaker J, Lord SM, Barnsley L, et al.
Diagnostic value of C2–3 instantaneous axes of rotation
in patients with headache of cervical origin.
Cephalalgia 1995;15(5):391–5.Watson D, Trott P.
Cervical Headache: An Investigation of Natural Head Posture
and Upper Cervical Flexor Muscle Performance
Cephalalgia 1993 (Aug); 13 (4): 272—284Sand T, Zwart JA.
The blink reflex in chronic tension-type headache,
migraine, and cervicogenic headache.
Cephalalgia 1994; 14(6):394–5,447–50.Vanagaite Vinigen J, Stovner LJ.
Photophobia and phonophobia in tension-type and cervicogenic headache.
Cephalalgia 199818(6): 313–8.Zwart JA.
Neck mobility in different headache disorders.
Headache 1997;37(1):6–11.Sjaastad O, Fredriksen TA, Sand Y.
The localization of the initial pain of attack.
A comparison between classic migraine and cervicogenic headache.
Funct Neurol 1989;4(1):73–8.Bovim G, Fredriksen TA, Stolt-Nielsen A, et al.
Neurolysis of the Greater Occipital Nerve in Cervicogenic Headache:
A Follow up Study
Headache 1992 (Apr); 32 (4): 175–179Edeling J.
Manual therapy rounds. Cervicogenic, tension-type headache
with migraine: a case study.
J Manual Manipul Ther 1997;5(1): 33–8.Martelletti P, LaTour D, Giacovazzo M.
Spectrum of pathophysiological disorders in cervicogenic headache
and its therapeutic interventions.
J Neuromusculoskel Syst 1995;3(4):182–7.Whittingham W, Ellis WB, Molyneux TP.
The Effect of Manipulation (Toggle Recoil Technique) for Headaches
with Upper Cervical Joint Dysfunction: A Pilot Study
J Manipulative Physiol Ther 1994 (Jul); 17 (6): 369–375Herzog J.
Use of cervical spine manipulation under anesthesia for management
of cervical disk herniation, cervical radiculopathy, and
associated cervicogenic headache syndrome.
J Manipul Physiol Ther 1999;22(3):166–70.Schoensee SK, Jensen G, Nicholson G, et al.
The effect of mobilization on cervical headaches.
J Orthop Sports Phys Ther 1995;21(4):184–96.Beeton K, Jull G.
Effectiveness of manipulative physiotherapy in the management
of cervicogenic headache: a single case study.
Physiotherapy 1994;80(7):417–23.Schöps P, Wiedesmann B, Seichert N, et al.
Vergleichende studies zur wirksamkeit krankengymnasischer
mobilisationstechniken bei cervicogenen kopfschmerzen.
Schmerz 1995;9(Suppl 1):60.Hobson DE, Gladish DF.
Botulinum toxin injection for cervicogenic headache.
Headache 1997;37(4):253–5.Tarhan C, Inan L.
TENS treatment in patients with cervicogenic headache.
Cervicogenic Headache International Study Group annual meeting. 1996.Sjaastad O, Fredriksen TA, Stolt-Nielsen A, et al.
Cervicogenic headache: a clinical review with special emphasis on therapy.
Funct Neurol 1997;12(6):305–17.
Return to CERVICOGENIC HEADACHE
Since 2-17-2023
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |