

The Chiropractic Vertebral Subluxation Part 10:
Integrative and Critical Literature From 1996 and 1997This section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Chiropractic Humanities 2018 (Dec); 25: 146–168 ~ FULL TEXT
Simon A.Senzon, MA, DC
School of Health and Human Sciences,
Southern Cross University,
Lismore, New South Wales, Australia.
Objective The purpose of this paper is to review and discuss the history of chiropractic vertebral subluxation (CVS) during 1996 and 1997. The literature during this period offered critical and integrative models emphasized by a need for research into operational and functional definitions.
Discussion Several integrative approaches emerged, from Rome’s 296 synonyms to Bergman’s Pain/Tenderness, Asymmetry/Alignment, Range of Motion Abnormality, Tissue Tone, Texture, Temperature Abnormality, and Special Tests (PARTS) analysis adopted by the profession in the United States. Other noteworthy contributions included Ruch’s Atlas of Common Subluxations, Epstein’s introduction of network spinal analysis, and Kent’s review of CVS models. Boone’s introduction of the Journal of Vertebral Subluxation Research was accompanied by his 3-part model with Dobson. These years also included the paradigm statement of the Association of Chiropractic Colleges, which was adopted by the American Chiropractic Association, International Chiropractors Association, and World Federation of Chiropractic. Two other papers included Nelson’s critique of the CVS paradigm and Keating’s 1996 “Hunt for the Subluxation.”
Conclusion The CVS reached a new stage of complexity and critique and offered new directions for research, integration, and development.
Key Indexing Terms Chiropractic, History
From the FULL TEXT Article:
Introduction
The theories of chiropractic vertebral subluxation (CVS) may have reached an apogee in the literature between 1996 and 1997. Several streams of discourse from preceding decades were captured in articles focused on criticism, [1] terminology, [2] integration, [3] consensus, [4] new vertebral models, [5–7] assessment procedures, [8] reviews of models, [9] and calls for various levels of research to study CVS. [7, 10, 11]
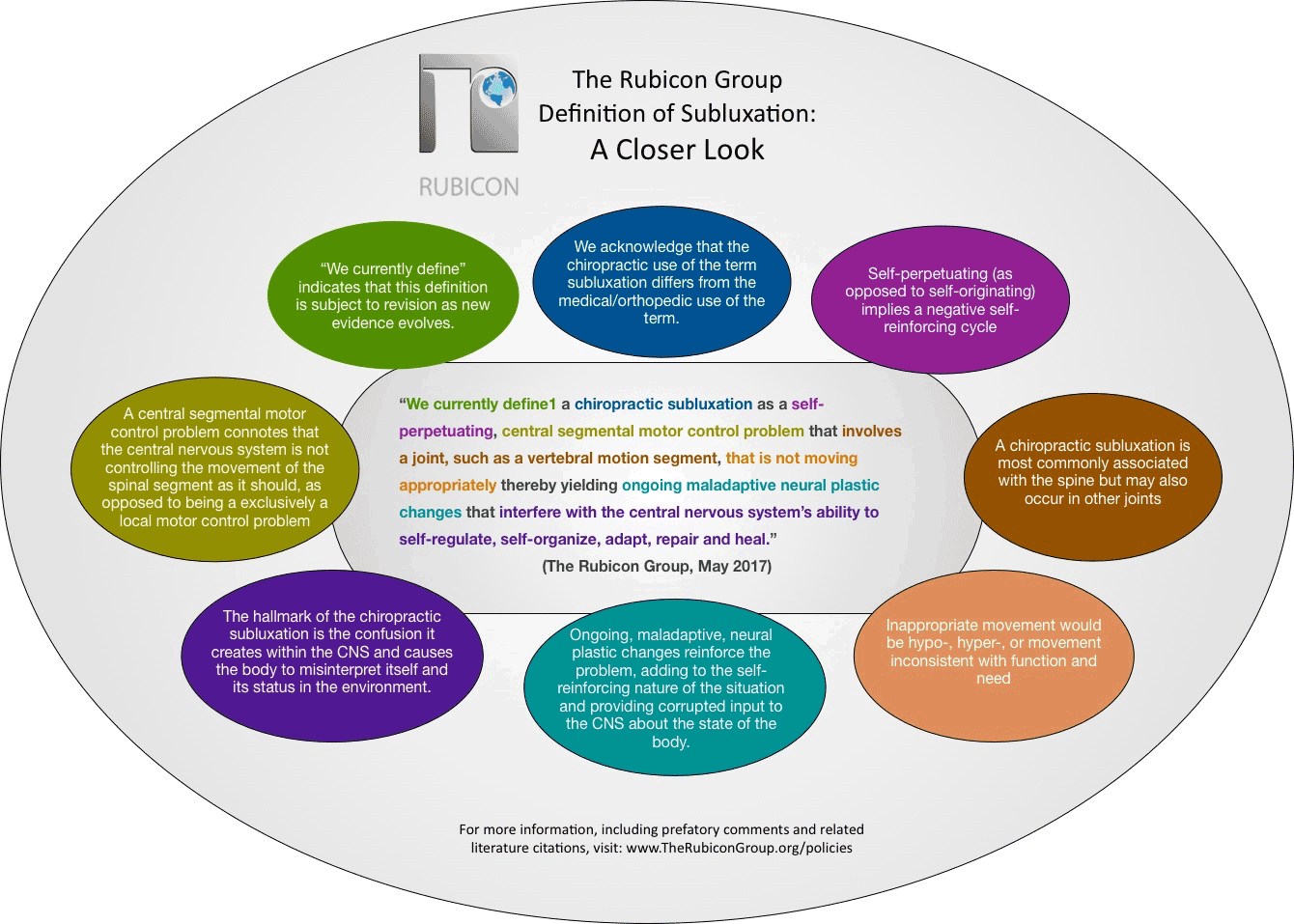
Events in chiropractic history are highlighted in this paper because of their relevance to CVS. The first was the trend to develop consensus statements that continued during this period. [12, 13] In 1996, the presidents of the chiropractic colleges in North America agreed to a definition of CVS, [41] which was endorsed by several national and international organizations. [14] During this period an “atlas of subluxations” was published, and develops a new perspective from the long tradition of dissection in chiropractic subluxation research. [15–20] Also, an assessment protocol became the methodology for CVS detection accepted by Medicare. [8, 21, 22] Debates in the profession about the lexicon continued during these years. As well, during this short period, increased calls were heard for research to include validity studies and reliability studies in chiropractic. [10] Keating also called for an operational definition for chiropractic, [10] which was answered by Owens, Boone, and Dobson. [5, 6, 7, 23]
During this time, the Journal of Vertebral Subluxation Research (JVSR) was developed originally to publish papers dedicated to research, theory, and models of CVS. [24] The JVSR was sponsored by the Council on Chiropractic Practice, [25] which was developing evidence-based guidelines for chiropractic during that time. [26] The JVSR was an outgrowth of that process and represented a school of thought, which was outside of the academic mainstream in chiropractic during this period. [27] It is possible that limited distribution, in addition to social and political forces within the profession, kept the wider profession from evaluating the articles in the journal on their own merits. The first 3 issues of the JVSR included Boone and Dobson’s Vertebral Subluxation Model (VSM); Kent’s review of subluxation models; and Epstein’s first peer-reviewed article, “Network Spinal Analysis: A System of Health Care Delivery Within the Subluxation-based Chiropractic Model.” [3, 5–9] These articles represent at least 4 different streams of the CVS literature and contribute to the context of this period. Boone and Dobson’s articles followed the trends to describe CVS as complex and proposed new research strategies for the profession. [5–7] Kent’s article reviewed the current literature, [9] and Epstein’s article demonstrated a practical integration of models and theories and was the culmination of more than a decade of clinical and theoretical development. [3, 28]
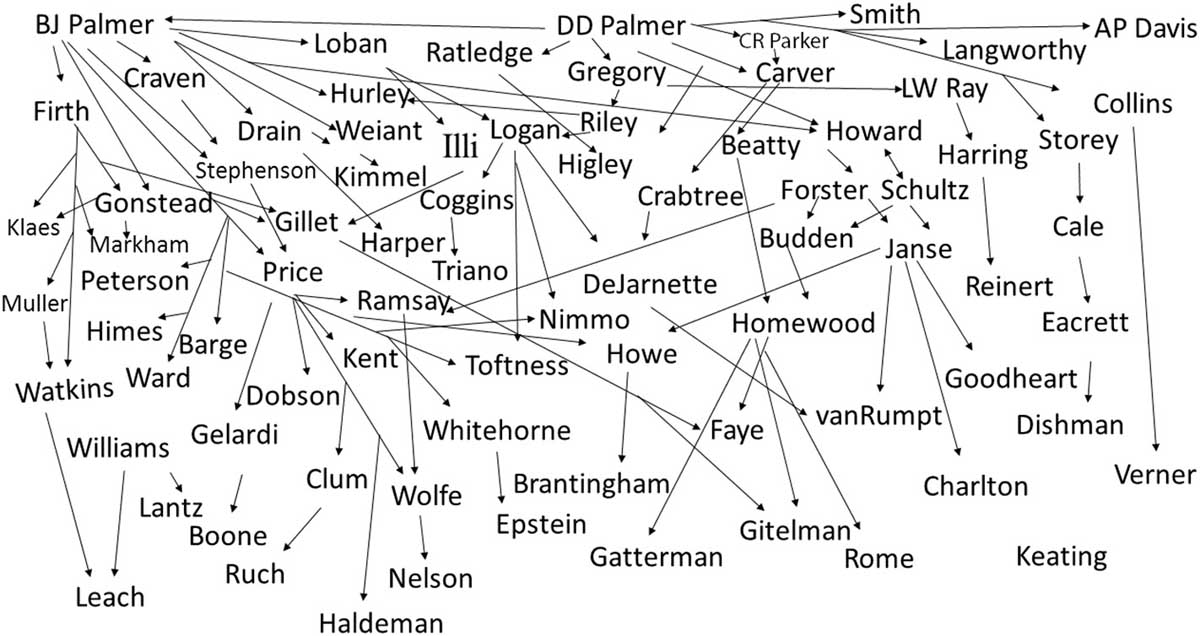
Figure 1 The purpose of this paper is to review and discuss CVS in chiropractic just before the turn of the century. The goal is to capture the culmination of a century of debate, consensus, and theory development on CVS (Figure 1). This paper aims to offer insights into the context of the period’s models, critiques, debates, and reviews.
Discussion
Consensus and Terminology
Three important publications in the literature during this period include the consensus statement by the Association of Chiropractic Colleges (ACC)4; Rome’s paper on CVS terminology [2]; and the Pain/Tenderness, Asymmetry/Alignment, Range of Motion Abnormality, Tissue Tone, Texture, Temperature Abnormality, and Special Tests (PARTS) method for CVS assessment and documentation. [8]
ACC Consensus (1996)
The ACC was formed in 1985 from an association of college presidents. In March 1994, an expanded ACC Educational Conference was held in Las Vegas, Nevada. The meeting led to a consensus statement published in July 1996, as part of the ACC Chiropractic Paradigm. The paradigm was signed by all college presidents and adopted by several organizations, including the International Chiropractic Association, American Chiropractic Association (ACA), and World Federation of Chiropractic. On May 23, 2001, at the World Federation of Chiropractic Congress in Paris, the ACC Paradigm was approved by the assembly. [29]
The ACC definition stated, “A subluxation is a complex of functional or structural or pathological articular changes that compromise neural integrity and may influence organ system function and general health.” [4] The definition captured the views based on the previous decades of research, model building, and theory in the literature. It was not designed as an operational definition to be tested, but as a consensus that could unify the many factions in the profession.
In a 4–part paradigm statement, part 4 reads:Chiropractic is concerned with the preservation and restoration of health, and focuses particular attention on the subluxation.
A subluxation is a complex of functional and/or structural and/or pathological articular changes that compromise neural integrity and may influence organ system function and general health.
A subluxation is evaluated, diagnosed, and managed through the use of chiropractic procedures based on the best available rational and empirical evidence. [4]The ACC paradigm statement might be viewed as the latest in a long line of consensus statements on CVS dating back to 196630 and 1905. [31]
Rome’s Synonyms (1996)

Figure 2
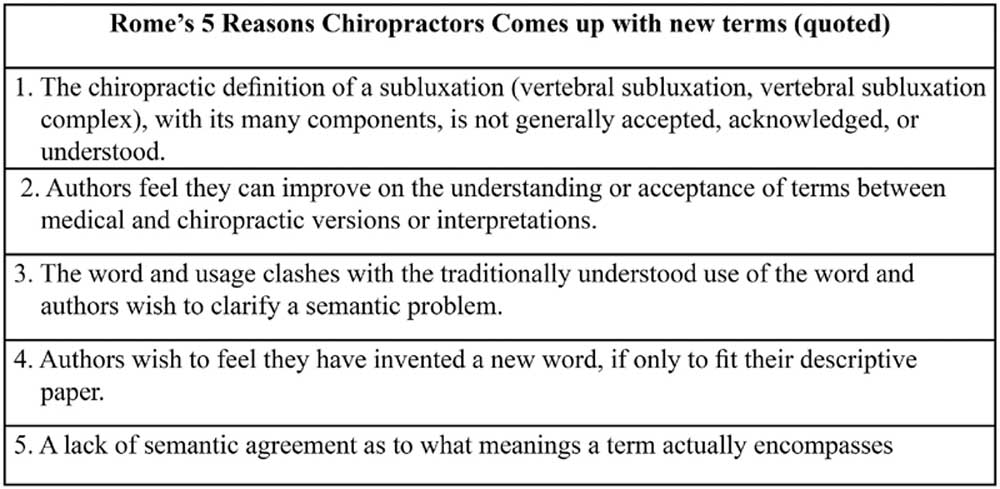
Figure 3 Peter Rome, an Australian chiropractor who graduated from Canadian Memorial Chiropractic College in 1969, published a literature review on as many CVS terms as he could catalog. [2] He eventually had a list of 296 terms from 1688 to 1996 and onward. The paper captured much of the chiropractic literature to date. [2] Rome came up with more than 500 terms since publication of the paper (Figure 2). [32, 33]
Rome offered 5 reasons for why chiropractors and other professions including the medical profession continue to come up with new words for subluxation, which included the need to create a new term, conflicts as to how the term should be defined, a lack of acceptance and understanding of the term, a need to build a bridge between the chiropractic definitions and medical definitions, and the semantic problem that the term subluxation already had a definition when chiropractors adopted it and gave it a new definition (Figure 3). [2] He wrote, “It is accepted that there is a defined scientific difference between a ‘medical subluxation’ and a ‘chiropractic subluxation.’” [2] Rome then described issues such as politics and communication surrounding terminology, and changing well-worn terminology. Rome explored the recent literature from Faye and Dishman’s subluxation complex to Gatterman’s subluxation syndrome, [34–36] to Brantingham’s somatic dysfunction,37 and to Leach’s segmental dysfunction and chronic neural dysfunction, [38] which included facilitation.
Rome argued that the disadvantage of trying to define new terms rather than retain an identifying term was detrimental to the profession’s identity. [2]
He wrote:Why create ambiguity by altering an established definition in the first place? Why confuse a reasonably well understood term? The effect of any major change can only dilute the identity of the chiropractic profession by questioning the very concept that it has been expounding for 100 years. [2]
He concluded that the term should be qualified but not discarded, as its historical use is rich for biology, clinical practice, and the history of the profession. [2] He suggested that there should be clarification between the term vertebral subluxation complex (VSC) for spinal dysfunction and subluxation complex for “articular derangements of the extremities.” [2] He also suggested there should be an explanation and dissemination of a broad and clear definition of the terms to other professions, publishers, medical dictionaries, journals, colleges, and associations.
Bergmann’s PARTS (1997)
In 1998, the ACA coordinated a consensus panel to develop guidelines for CVS diagnosis without the need for x-ray analysis [21] and to adequately document chiropractic services for Medicare as outlined in the Balanced Budget Act of 1997. The panel adopted Bergmann’s PARTS criteria, which included technique-specific tests. [8] The ACA panel adopted PART, not PARTS. [21] Medicare guidelines required 2 of the 4 PART criteria, 1 of which must be changes to asymmetry and alignment or abnormal range of motion. [21]
Bergmann and colleagues authored a textbook that included the PARTS concept. The book arose from the intercollegiate conferences around chiropractic technique, [39–41] which were linked to older conferences about the neurobiologic mechanisms of spinal manipulative therapy. [12, 41, 42] For example, at the 1977 workshop that followed the 1975 National Institute of Neurological Disorders and Stroke conference, Greenman, from the College of Osteopathic Medicine at Michigan State University, wrote,
“The three diagnostic findings of somatic dysfunction are(1) asymmetry,
(2) restricted motion, and
(3) tissue texture abnormality.” [43]His description of tissue texture is similar to previous chiropractic approaches to palpation and instrumentation. [44, 45] Bergmann’s analysis can be linked to osteopathic diagnostic procedures and chiropractic literature on clinical and empirical analysis.
Keating’s Influence on Discourse
Keating’s influential article “To Hunt the Subluxation”10 was published in 1996 and summed up his viewpoint by defining types of validity tests.10 The paper reflects his ideas and is still cited in the literature. [] 1, 10, 46, 47, 48, 49, 50, 51, 52 Keating’s arguments from the article laid the foundation for subsequent publications that are often cited in calls to dismiss the term subluxation from the chiropractic literature. [] 47, 52, 53, 54 By reviewing a chronology of Keating’s writings, we may more fully understand the perspective that he brought to his writings on chiropractic and better assess his work and impact.
Between 1984 and 1996, Keating published at least 25 articles on chiropractic. [10, 55–79] Keating’s first call for an operational definition for CVS came in the 1980s,59 followed by several papers and a textbook exploring the epistemological rationale for his position and mapping out several areas of potential research for the profession. [10, 67, 70]
In 1990, Keating wrote:But let us not continue to mistake private empirical support (even when recognized by governmental bodies, such as the NZC) nor basic science rationale (even when well referenced) for clinical research validation. Let us not confuse “science consistency” with scientific evidence of the effectiveness of a treatment, nor with scientific validation of a hypothetical construct (such as vertebral subluxation complex). The proof of the pudding in an applied discipline is the scientifically demonstrated utility of its theories and methods, and in that respect we are very much nearer the beginning than the end of our journey. There is great room for dialogue and debate. [80]
Keating’s references in this statement are to the Royal New Zealand Commission (NZC) Report and Kaminski’s proposed evaluation procedures for chiropractic practices. [81, 82] He argued for several levels of validity studies throughout his career. [10, 71]
Keating’s Background and First Roles in Chiropractic
Figure 4 Keating completed his PhD in clinical psychology from the State University of New York (SUNY) at Albany in 1981. His dissertation was a behavioral approach to nocturnal enuresis written when Behaviorism was at the end of its dominance in psychology. [83, 84] After completing a residency, Keating taught as an adjunct professor at the Behavioral Medicine Clinic in the department of psychology at the University of the Pacific in Stockton, California. [86] During that time, he was hired by Don Smallie to do research for the Stockton Foundation for Chiropractic Research. [55, 86] Smallie introduced Keating to Miller, the president of Palmer College of Chiropractic West (PCCW). [86] Keating was hired by PCCW in 1983 and was soon head of the research department. He eventually taught at several chiropractic colleges. Keating died on October 14, 2007 (Figure 4). [87]
Keating and Mootz (1986–1989)
Keating’s first review articles on chiropractic and CVS were coauthored with Robert Mootz, a 1980 Palmer College of Chiropractic (PCC) graduate who started working at PCCW in 1985 and later became dean.88, 89 They collaborated on several papers in the late 1980s, [60, 61, 66] some of which should be explored primarily in articles on philosophy and scope of practice and included discussion related to politics, medicine, and research. It seems that many of the arguments in these early writings formed the foundation for Keating’s later works.
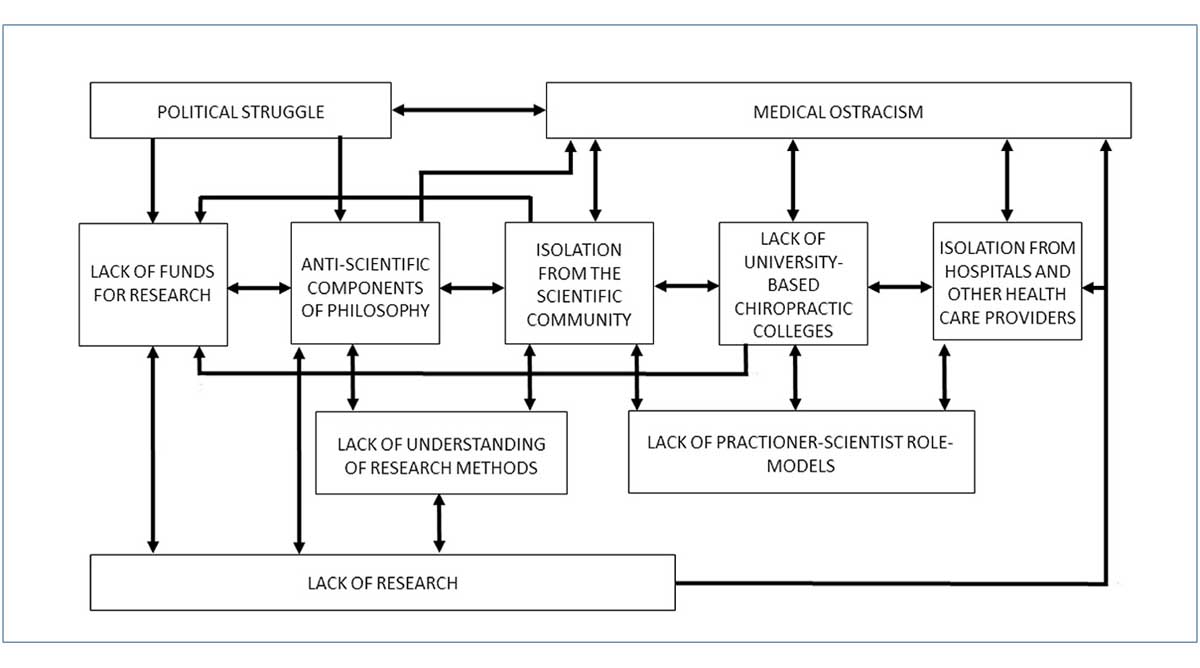
Figure 5 In 1986, Keating, Mootz, and Jim Nelson presented a model of clinical, scientific, and educational development at the Palmer Research Forum. [60] They suggested that research in chiropractic was limited for several interlocking reasons. They proposed that the limitations were related to political struggle, medical ostracism, and “lack of funds for research, anti-scientific components of the philosophy, isolation from the scientific community, lack of university based chiropractic colleges, isolation from hospitals and other healthcare providers, lack of understanding of research methods, and lack of practitioner-scientist role-models.” [88] They developed a chart to depict the “pattern of inter-locking impediments to the development of chiropractic science” (Figure 5). [88] In these articles, Keating and Mootz seemed to be guided by David Barlow’s scientist-practitioner paradigm. [90] Barlow was a psychology professor at State University of New York, and it is suspected he may have been one of Keating’s professors. [91]
In 1989, Keating and Mootz described the values of clinician-scientists that should be instilled into the profession as a way to develop a “research consciousness.” [66] They suggested that such a consciousness should be promoted through dialogue with the leadership of associations, colleges, and technique organizations. They proposed it could then spread to the colleges. They recommend an open-minded caution in relation to new ideas and claims for efficacy as well as counsel to the future scientists, to be wary of the perceived public relations threat they may pose to political medicine and the “traditionalists” within the profession. [66]
Keating and Mootz acknowledged the importance of model building and the understanding of CVS mechanisms to the future evolution of chiropractic, and they emphasized clinical research to evaluate chiropractic’s usefulness. [66] They stated that clinical trials should become a priority with a focus on placebo, neural circuitry, biomechanics, kinesiology, and prognostic indicators. However, they also emphasized that research was secondary to the promotion of health. Two examples they give are the lack of research on analgesic medications and hypnosis. Even though the mechanisms were not fully understood, both were recommended to patients. [66]
Keating and Mootz recognized that clinical trials would be difficult and costly for chiropractors, and so they proposed single-subject and small-group research designs. Each practitioner could do a clinical “trial of one” and critically evaluate the literature by replicating data trials and thereby add to the literature. They suggested that “Each new patient becomes the focus of a potentially new theory.” [66] Carefully controlled case studies could produce “field based descriptive clinical report(s).” [66] Their emphasis on well-designed case studies followed a similar recommendation made by Keating and Miller about the importance of case studies. [59]
Keating and Mootz suggested, based on the historical record, defensive dogmatism developed in chiropractic from the pressures from political medicine, accounted for much of the infighting within chiropractic. They concluded that rigidly adhering to theories that are untested equates to “dogma” and that dogmatic thinking has hindered scientific development in chiropractic. [66]
Keating’s Writings (1986–1995)
In 1986, Keating initiated calls for an operational definition for CVS that were renewed throughout his writings. [59, 67, 70] An operational definition could be used in randomized trials, placebo-controlled clinical trials, and other research designs. In 1992, Keating acknowledged that most of the chiropractic profession relied on CVS, but he did so by saying the “straights” believe in “subluxation” and the “mixers” believe in “spinal lesion.” [72] He wrote, “Straight chiropractors have traditionally adhered to an unswerving belief in the meaningfulness of subluxation as a clinical entity… the mixer community, an unswerving belief in the significance of the chiropractic lesion.” [72] Keating did not make the point that most of the leaders from the “mixer” side of the profession were CVS theorists and most of the profession was using the term subluxation, even though some were calling for new terminology and a new focus for the profession. [12, 13, 37, 92–101]
Keating concluded that CVS had questionable validity, was tentative, and was largely an untested hypothesis. He suggested that scientific development was impossible if CVS was defined as an “intrinsically deleterious clinical finding,” [72] if symptoms were not used as a primary factor in its detection. [72]
Keating summed up his ideas in his book Toward a Philosophy of the Science of Chiropractic: A Primer for Clinicians. [70] It is a thorough book in chiropractic on research design, philosophy, and the philosophy of science. It was published by the Stockton Foundation for Chiropractic Research. Keating built upon the scientist-practitioner paradigm and developed several detailed critiques and suggestions for the profession’s research agenda to move forward. [70]
Keating’s “To Hunt the Subluxation” (1996)
Keating’s 1996 article “To Hunt the Subluxation: Clinical Research Considerations” [10] has been cited 18 times in the indexed literature, according to Google Scholar, and 21 times in the Cumulative Index to Nursing & Allied Health Literature database. [102] Two documents that reference this paper include Nelson’s 1997 article and the preface to the fourth edition of Leach’s book, published in 2004. [1, 46] Both have been cited in papers, according to Google Scholar. [102]
This paper is also cited by Keating, Charlton, Grod, Perle, Sikorski, and Winterstein in “Subluxation: Dogma or Science?” to support this statement: “there is today no scientific ‘gold standard’ for detecting these reputedly ubiquitous and supposedly significant clinical entities.” [47]
For this statement to be accurate, the references for the 1996 article would need to be comprehensive enough to support that claim; however, I suggest that they are not. [10] Most references in the body of the paper point to reliability studies. [103–108] Based on these references, Keating claimed there is no hard evidence for the validity of an operational definition for CVS. [10]
He argued that chiropractic researchers have not established a relationship between CVS and health problems and that “the validity of the chiropractor’s ‘subluxation complex’ has not been studied by chiropractors or anyone else.” [10] Keating further stated that there was no standard to compare CVS detection methodologies.
Keating’s call for an operational definition is an important contribution to the literature. An operational definition of CVS that could meet the rigorous demands of the scientific method around many types of research questions was needed. [10] To address this issue, he proposed several types of research questions involving inter and intraexaminer reliability, concurrent validity, predictive validity, discriminant validity, and trial validity, and challenged the profession to operationalize CVS and begin to conduct validity research. [10]
Critique and Development of Theories
In 1997, Nelson published a critique on CVS and William Ruch an atlas. [1, 15] Nelson’s critique built on previous arguments to do away with subluxation as a term and emphasized the need for an operational definition. Ruch’s atlas bolstered previous models by establishing a new level of anatomical data to expand on CVS criteria.
Nelson’s Critique (1997)
Craig Nelson graduated from Northwestern Chiropractic College in 1974 and was a former instructor there. In 1997, Nelson wrote a critique of Gatterman’s book, [36] with some suggestions for future research. [1] Nelson’s references included chapters from Gatterman’s book, [36] Faye’s notes, [109] papers by Lantz, [110] the ACC paradigm, [4] and Keating’s 1996 article. [10] Most of the paper consisted of Nelson’s opinions and generalizations about the dichotomy in chiropractic around CVS along with some insightful suggestions for testing hypotheses. [1] The article explored the limitations of model building and the need for operational definitions. It is in part an attempt to discredit the extensive consensus processes that led up to Gatterman’s book and the ACC paradigm. [1, 4, 36]
Nelson criticized the semantic approach to deciding upon subluxation terminology and suggested that all of the models of the VSC are a tautology. He did not think that CVS should be described as more than one thing and certainly not as a complexity of many components or in terms of syndromes. [1] Nelson’s critique pointed to the need for strong theory building and hypothesis testing. He noted the need for the literature in the chiropractic profession to demonstrate the differences between hypothesis and theory, and how to test them.
Nelson suggested that any theory should “bear some resemblance to its historical antecedents.” [1] Further, he wrote, “Unless the profession is willing to declare that D. D. Palmer’s ideas have no current relevancy, any subluxation theory should retain some connection to Palmer’s formulation of subluxations. Otherwise, it’s more appropriate and honest to simply abandon the term.”
However, Nelson did not cite the current theories, which were built upon the models and research of Verner, [111] Homewood, [44] Watkins, [30] and Harper. [112] All of those theorists cited D. D. Palmer and integrated his theories into their models. [113] The paper did not contain this historical context. A similar critique of Nelson’s paper was written by Faye, who acknowledged that his own definition of the VSC in 1967 was inspired by the consensus definitions published in the Journal of the ACA in the 1960s. [114]
Ruch’s Atlas of Common Subluxations of the Human Spine and Pelvis (1997)

Figure 6 William Ruch graduated from Life Chiropractic College West in 1986 (Figure 6). Ruch dissected over 250 cadavers while teaching in the human spinal dissection laboratory at Life Chiropractic College West from 1987 to 1993. He has worked in the anatomy department as an adjunct faculty since 1997. [115] Ruch’s photo atlas was based on his dissection research. [15] The second edition was published in 2014. [15]
The atlas viewed CVS from the perspective of degeneration by including photographs, x-ray imaging, computed tomography scans, and magnetic resonance imaging. Ruch proposed that the degenerative process owing to changes in alignment of the spine leads to impaired blood and cerebral spinal fluid dynamics; pain; loss of neurological control; and alterations of the cord, brainstem, and central nervous system (CNS). The emphasis of the book is on the normal biomechanics of the CNS and how movements of the spine, cord, and associated tissues are affected by CVS. To help explain his extensive observational images, Ruch relied on the literature on spine and cord dynamics. [15, 116]
Ruch’s Atlas was written following the chiropractic tradition that started with D. D. Palmer’s osteological lab, [117] Swanberg’s work inspired by Smith, [17, 118] Forster’s early dissection research to define subluxation, [119] Janse and Illi’s study of the lumbars and pelvis, [19, 120] and Winterstein and Bachop’s intervertebral foramen studies. [20] Ruch developed a complex view of CVS that furthered the paradigm, integrating Breig’s biomechanics of the spinal cord and CVS. [15, 116, 121–124]
Epstein’s Integrative Approach
In 1996, Donald Epstein published his model and protocols related to his network spinal analysis (NSA). [3] Epstein referred to his approach with the term network, because it was his attempt to include a wide variety of models, theories, and techniques; to capture the idea of a distributed network; and to include Pert’s theory of a somatopsychic network, which included her observation of high concentrations of neuropeptides in the dorsal horn of the spinal cord. [125–127] Since 1996, Epstein has continued to develop his theory and methods. [128, 129]
Figure 7 Epstein graduated from New York Chiropractic College in 1977, during which time Napolitano (a Palmer graduate) was president (Figure 7). [88] In 1983, Epstein taught and published articles on his NSA. [124, 130–134] Between 1989 and 1996, Epstein’s model and clinical protocols evolved. [126–140]
In 1983, Epstein described using instrumentation, which included classic paraspinal thermal pattern work from the Palmer school, leg checks, and palpation. His intention was to develop an analysis that could be used with any chiropractic technique. [130] Central to his analysis was the differentiation between what he termed class A or structural subluxations and class B or meningeal subluxations, which he later termed the facilitated subluxation. He proposed that class A comprised primarily of fixations and meningeal subluxations because of more complex neurological phenomenon usually related to chemical and emotional etiology. He linked class B to B. J. Palmer’s concepts of torqued meningeal occlusion and multiple cord pressures by tension. [141]
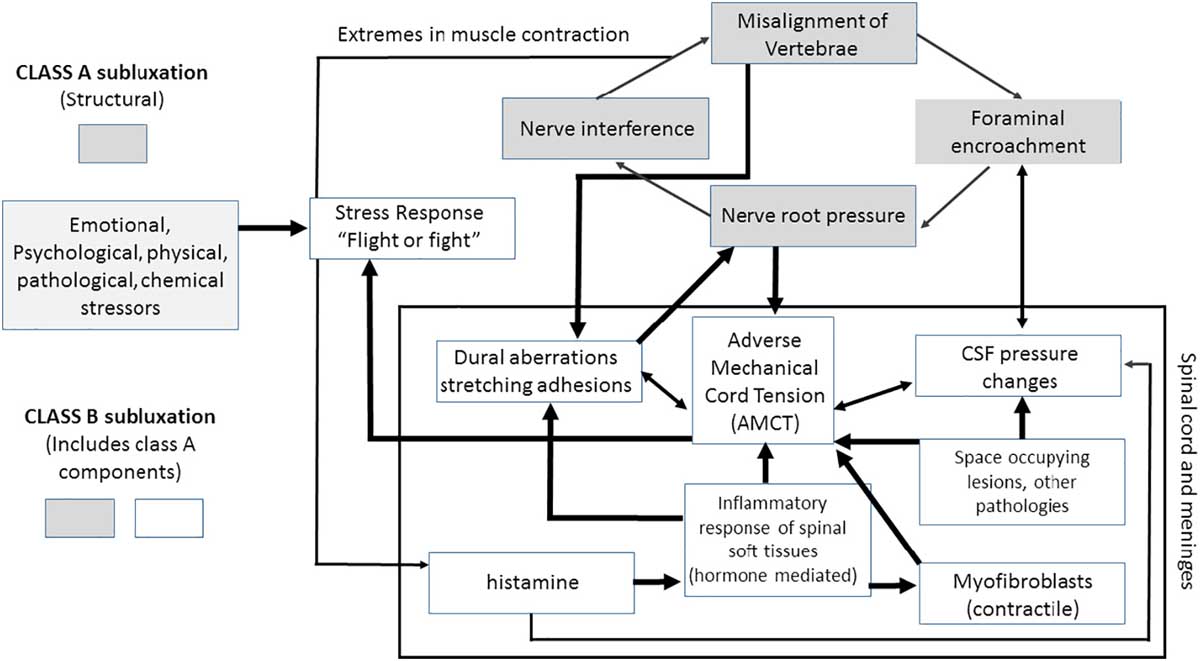
Figure 8 Epstein related the class B functionally to Speransky’s neurodystrophic process, [142] physiologically to a global CNS response affecting cerebrospinal fluid transport and circulation, and biomechanically to the meninges. [132] He hypothesized that the CNS response involved referred tension patterns throughout the spinal and meningeal system, which may relate to areas of pain and altered movement to “the major site of neurological insult” [124] (Figure 8). [3]
Network Chiropractic Analysis was a combination of reflex techniques such as Logan and Sacro-Occipital Technique, [143, 144] full-spine structural techniques such as Pierce-Stillwagon, [145] and upper cervical techniques. [146] It was thought that analysis had to do with sequence and force application in relationship to facilitation, dystrophic processes, and reflex patterns. [3, 35, 147]
Epstein believed that the meningeal subluxation caused a tension on both ends of the spine, which he thought could fluctuate from one end to the other. [124] He based this thought in part on Toftness’ incorporation of D. D. Palmer’s theory that the neuroskeleton is a tonal regulator of the tension frame. [148] Toftness believed that CVS moved through the frame as a type of stress response. [149] Epstein hypothesized that an area of critical tension could be determined. [132]
Thomas Faulkner wrote a letter to Epstein suggesting that he should include the works of Breig and Lowell Ward: [150] “I found your article regarding meningeal anatomy most interesting. I further commend you on your excellent anatomical exactness and thorough documentation of your report by listing medical references.” [151] Epstein later included Breig and Ward in his expanded writings, now referred to as Spinal Meningeal Functional Unit. [134]
Epstein described his theory in relation to the postural response to stress and how the meningeal tension was related to the central nervous stress response. [134] This developed from Ward’s Spinal-Column-Pelvic-Meningeal-Unit, [123] Breig’s pons-cord tract dynamics, [152] and several other neurological models from the Russian neurophysiology literature. [153] In 1987, he expanded on his theory by integrating Homewood’s dynamic subluxation mode [144] with Seyle’s stress cascade, [153] Korr’s facilitation hypothesis, [154] and Travell’s trigger point model. [155]
In 1989, Epstein was a speaker at the Academy for Research in the Chiropractic Sciences International symposium on Chiropractic Measurement and Methodologies for the 21st Century. The Academy for Research in the Chiropractic Sciences International was organized by several leading technic developers, such as Stillwagon, Toftness, Ward, Sweat, and Pettibon. This presentation integrated his analysis with the theories of Speransky, [142] Ukthomsky, [153] and Seyle in relation to palpation for pathologically dominant patterns in the CNS. [135, 156]
By 1996, Epstein developed his analysis into a 5–phase model of CVS patterns layered into 3 levels of care. [3] The phasing system of analysis was based in part on Grof’s theory of condensed experiences embedded as memory in the neurophysiology, [157, 158] tensegrity models of tension dissipation, [159] Coggins interpretation of Logan Basic, [143] Pierce-Stillwagon’s spinal analysis, Ward’s stressology, [123] B. J. Palmer’s perspective, and D. D. Palmer’s theory of the neuroskeleton. [127, 148] The proposed system included a sequential approach to the CVS patterns. [127] From this period of Epstein’s work, empirical studies of the spinal wave associated with NSA protocols and qualitative research on recipients of NSA care were attempted. These studies led to models of emergent health-related quality of life, wellness outcomes, and a reorganizational healing paradigm. [160–167]
The spinal wave behavior associated with NSA has been studied from 1997 until 2015 [168] at University of Southern California and other universities by engineers looking at the mathematical characteristics of the surface electromyography signals at 4 levels of the spine: sacrum, lumbar, thoracic, and cervical. [30, 128] Several papers, [169–171] conference presentations, [172–175] and a dissertation have explored its features. [176] It is proposed that the spinal wave associated with network care can be mathematically categorized as the first central pattern generator in the spinal cord apart from gait [171] and that coherence at a distance develops at the ends of the spine. [175] Different experiments conducted 10 years apart demonstrated similar mathematical signals, thus this mathematical approach to studying coherence in the spine may lead to a new measure for evaluating the CNS. [175]
Boone’s Journal of Vertebral Subluxation Research (1996–1997)
Figure 9 In 1996, Ralph Boone started the JVSR and continued as the editor until 2000. [24, 177, 178] He completed a PhD in biology from the University of Richmond in 1974. From 1980 to 1990, he was the director of research and computers at Sherman College of Chiropractic. He earned his chiropractic degree from Sherman College of Chiropractic in 1990. Boone was president of Southern California College of Chiropractic from 1990 to 1994, president of the Straight Chiropractic Accrediting Agency in the 1990s, acting head of the New Zealand School of Chiropractic from 1998 to 2000, director of research for the Association for Network Care from 2002 to 2004, and director of research at Sherman from 2004 to 2009. Boone died on November 21, 2010 (Figure 9). [179]
There is some confusion in the literature about JVSR being a journal and that articles are refereed. For example, McGregor-Triano writes, “the JVSR is not classified as a ‘journal' (Ulrich's Periodicals Directory)," and “is considered by Ulrich's Periodical Directory (2006) to be ‘academic' and ‘scholarly.' [180] In contrast to McGregor-Triano's claims, Ulrichsweb's Global Serials Directory in 2015 lists JVSR serial type as a refereed and peer-reviewed “journal." [25] Only the content type is described as “Academic/Scholarly." [25] Furthermore, queries to several of the early authors and reviewers from the first issues suggest that Boone was heavy-handed as an editor and perhaps even unusual in his approach to peer review but that he certainly sent papers out for review and requested revisions and resubmissions. [181, 169, 160, 179] According to Graham Dobson (personal correspondence, September 13, 2016), it was not Boone's intention to develop a top-tiered journal like Spine. Boone relied on his 2 decades as an academic and a scientist to shape his editorial style. [182–187]
In the first issue of JVSR, Boone summed up the mission of the journal and his hopes for CVS research. [24] He acknowledged there was plenty of research to do. He proposed that the etiology, biomechanics, physiology, and consequences of CVS justified the journal’s narrow focus. Boone believed that without a journal dedicated to publishing peer-reviewed literature on all aspects of the CVS, studies on spinal manipulative therapy for low back pain and musculoskeletal conditions may dominate the literature. He acknowledged that those research foci may be interesting, but if they were to dominate the literature we would not “expand our evidence base of vertebral subluxation further than it being a spinal lesion associated with various pathologies.” [24] He recommended a comprehensive research strategy including multiple theoretical and clinical perspectives.
Boone focused the journal on publishing articles describing investigative methodologies and appropriate paradigms through which to test various hypotheses. The first issue included 2 papers on CVS models with the hopes of expanding perspectives and reassessing CVS. [5, 9, 24]
The objective of the first volume was to include a wide range of methods to clarify and describe models of CVS and increasing public awareness of the benefits of CVS correction and to publish innovative research. Besides the papers on models, [5–7, 9] the first volume included technique papers, [3], 188 research on surface electromyography paraspinal normative data, [189, 190] case reports, [191–193] small research designs, [194–198] a survey report on guidelines, [11] and retrospective studies including the Blanks study, which was the largest chiropractic study on quality of life to date. [162]
In the second volume published in 1998, Boone reflected on the papers from 1996 and 1997. [178] He claimed that scientific evidence had accrued indicating positive health benefits after or concomitant with CVS correction. The 3 areas he noted were that health benefits accumulated, improved function was promoted, and physiological and neurological changes occurred. [11, 169, 161, 189–208] Boone acknowledged that some areas of CVS research were more difficult to study and concluded that the neurological components would take the most effort to elucidate. [177] He established relationships with social scientists, biological scientists, and engineers at the University of California, enlisting several PhDs to explore some of the more elusive phenomena. In 2000, Matthew McCoy, a Life Chiropractic College and Emory graduate, became editor, and in 2011 the journal changed its name to Annals of Vertebral Subluxation Research. [209–211]
Kent’s Models (1996)

Figure 10 Christopher Kent graduated from PCC in 1973. He joined the faculty upon graduation, worked in the research department, and was elected president of the faculty senate. He was invited as one of 11 chiropractic researchers to participate in the National Institutes of Health workshop on The Research Status of Spinal Manipulative Therapy in 1975. [42] After entering private practice in the 1980s, he focused on developing objective measures to monitor nerve interference related to CVS. In 2001, he was elected chair of the United Nations Non-Governmental Organization Health Committee. In 2010, he founded the Foundation for Vertebral Subluxation, of which he is president, with McCoy. In 2016, he was named director of evidence-informed curriculum and practice at Sherman College of Chiropractic (Figure 10). [212, 213]
In 1996, Kent’s article “Models of Vertebral Subluxation: A Review” was published in the first issue of the JVSR. [9] The article referenced the histories of Haldeman, [214] R. J. Watkins, [215] Terrett, [216] and Rome and concluded that such an entity must exist. [2] He defined Stephenson’s 4–component model based on B. J. Palmer’s work, otherwise known as MOPI or malposition, occlusion of an opening, pressure or impingement, and interference to the transmission of mental impulses. [217] Kent then described the models of Faye, Dishman, and Lantz. [34, 35, 218, 219]
Kent explored the major components of CVS by reviewing the basic science and clinical literature on the topic. He started with the joint degeneration model and the neurological consequences. These included cord compression, nerve root compression, local irritation, vertebral artery compromise, and autonomic dysfunction. The other models he reviewed included the nerve root compression model, the dysafferentation model, and the neurodystrophic model. After describing 15 references on the compression model, Kent concluded, “While some may criticize the ‘garden hose’ model as being overly simplistic, the nerve root compression hypothesis is far from obsolete.” [9] The dysafferentation model proposed by Kent involved the nociceptive and mechanoreceptive structures. The neurodystrophic model, according to Kent, relates directly to tone. It links neural dysfunction to pathogenesis via the intertwined nature of the nervous system, endocrine system, and immune system. [9]
Kent called for an operationalized model that accounted for the many neurobiological models and was broad enough for the many clinical operational models. [9] Outcomes assessments should be developed for conceptual models, analytic procedures, type of adjustment, and criteria for success or failure. Based on previous classifications, Kent adopted Dan Murphy’s 3 classes of CVS models: segmental models, postural models, and tonal models. [9]
Kent proposed that the methodologies for correcting CVS have a common neurological objective. [9] Models to demonstrate objective clinical outcomes could be developed for any method as long as they measure evidence for improved “functional integrity of the nervous system, and improvement in general health and quality of life indicators.” [9] He suggested that researchers focus their efforts on practice procedures that are efficient and predictable.
Boone and Dobson’s Vertebral Subluxation Model (1996–1997)

Figure 11
Graham Dobson
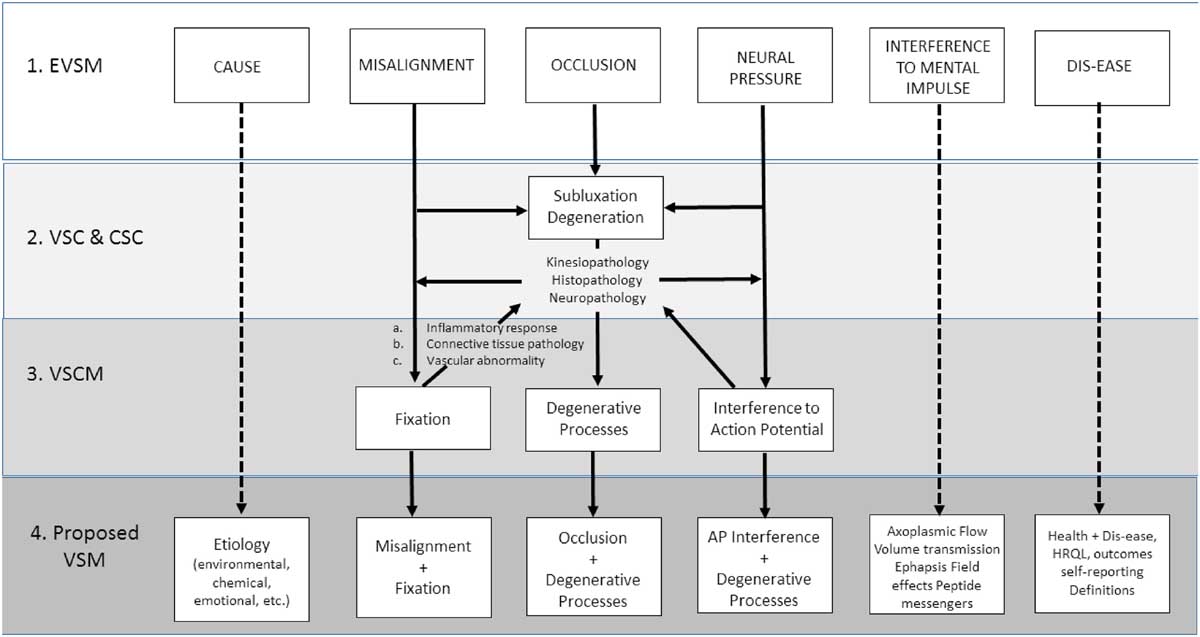
Figure 12 Ralph Boone and Graham Dobson wrote a 3–part article in the first 3 issues of JVSR. [5–7] They proposed the vertebral subluxation model (VSM) as a way to integrate all previous models and to research CVS on many levels of complexity. Dobson graduated from PCC in 1971. He was dean of clinical sciences at Sherman College from 1979 to 1982, vice president of the chiropractic program of Southern California College of Chiropractic from 1990 to 1994, and interim president of Southern California College of Chiropractic from 1994 to 1995, and has held various positions at the NZ New Zealand School of Chiropractic SC (now the New Zealand College of Chiropractic) since 1998 (Figure 11). [220] In the late 1990s, Dobson developed his own CVS analysis by integrating methods from Goodheart and Blair, as well as White and Panjabi. [221]
Boone and Dobson proposed the VSM to integrate the traditional concept of B. J. Palmer’s early vertebral subluxation model (EVSM), Faye’s VSC, Dishman’s chiropractic subluxation complex (CSC), and Lantz’s VSC model (VSCM). [5] The VSM integrated the models from the 1980s with the early model from B. J. Palmer, along with the literature on outcomes, health-related quality of life, and proposed neurological models of mental impulse (Figure 12). [5]
The papers by Boone and Dobson included quality of life. The articles explored the VSM in 3 parts: physiological and biomechanical, [5] health and etiology, [6] and interdisciplinary research methodologies appropriate for testing the VSM. [7] The articles were in part an answer to Keating’s call to put politics and propaganda aside and conduct serious research on CVS. [70]
In the first article, they quote from Keating’s 1992 book:What of subluxation? Will we ever set aside the political uses of these supposed spinal boo-boos long enough to operationally define and investigate their potential role in health and illness? If we were to cease propagandizing subluxation as “the silent killer” and study it as a serious scientific phenomenon, who knows what we might find? Yet, so long as we insist on emphasizing the chiropractic lesion as our political “raison d’etre,” the real “tragedy of the subluxation” will continue to be our ignorance of it. [70]
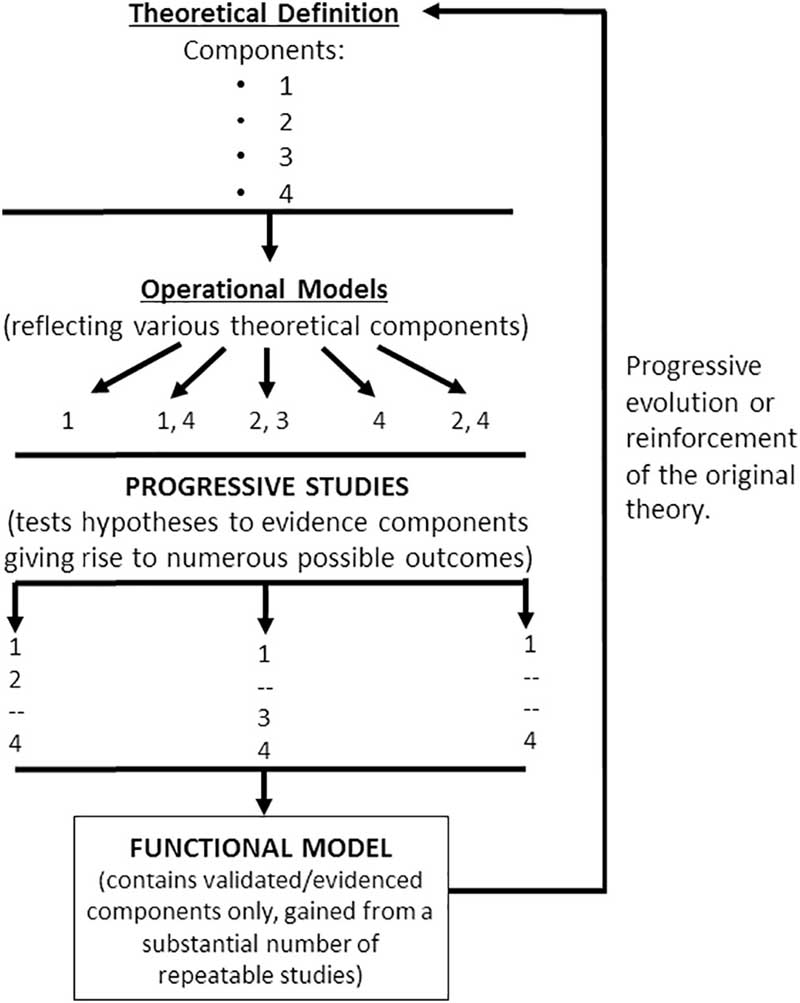
Figure 13 Boone and Dobson partially agreed with Keating. An operational definition was essential. They suggested that consensus definitions should arise from specific operational definitions tailored to test each component of CVS, followed by progressive studies, which might then be developed into a functional definition. From there, further operational definitions could emerge (Figure 13).
In response to this quote, they wrote:The present model is designed to accept this challenge. In doing so, it becomes necessary to develop a functional definition which also encompasses parameters dealing with etiology and health and to include, for scientific investigation, those aspects of the vertebral subluxation which are likely to impact on these phenomena. [5]
Boone and Dobson started by exploring aspects of the early CVS that had evidence and aspects of detection that were repeatable. [5] They did not accept the early theory outright. Rather, they focused on evidence for the theories associated with the early model, namely B. J. Palmer’s 4 components of CVS: misalignment of a vertebra, occlusion of a foramen, pressure on nerves, and interference with mental impulse flow. Included in their functional definition was the fourth component or the organizing information analogous to the mental impulse. Boone and Dobson pointed out that one of the failings of modern definitions is the exclusion of the mental impulse hypothesis. [5]
By expanding research questions, they suggested we might be able to test hypotheses that were previously thought untestable. They noted that it was a mistake to assume that mental impulse was adequately described as the action potential. For example, they suggested that the mental impulse theory, when viewed as a complex hypothesis, might be tested by examining factors that were involved with neurally mediated organizing coordination information. [5] These might include neural transmission outside of the action potential, such as growth factors, ephaptic transmission, axoplasmic transport, the propulsion of energy and information from nerve to nerve such as neurotransmitters, and alternative export of molecules for sliding filaments, bidirectional movements, and anterograde and retrograde flow. [5]
Boone and Dobson critiqued the recent trend in the profession of redefining the traditional theory without adequate testing and evidence to do so. For example, the mental impulse was equated to action potential by Haldeman and Drum in 1971. [222] Other theorists sought ways to integrate the mental impulse hypothesis. R. J. Watkins addressed this issue and emphasized the importance of the quality of the impulse in 1965; he related it to the neurology of the joint getting detuned, whereas the adjustment retunes the joint neurology. [30, 223] It was also proposed that research into subtle energy systems and energy medicine might be appropriate avenues to pursue research into the mental impulse concept. [224, 225]
Because of the variation in practice, philosophy, and definitions within the profession, Boone and Dobson suggested an encompassing functional definition of CVS, as follows:A vertebral subluxation is a potentially reversible and/or preventable alteration of the intervertebral relationships of one or more articulations of the spinal column or its immediate weight bearing components of the axial skeleton; accompanied by a change in the morphology of the tissue occupying the neural canal and/or intervertebral foramina; as well as an alteration of neural function sufficient to interfere with the transmission of organizing information, believed to be homologous to the mental impulse, thus contributing to negative health outcomes. [5]
This functional definition was designed to include many testable tenets and form a basis for several operational definitions.
Critical Analysis
Several important areas of discussion arise from an analysis of a sample of the literature from this period. The main areas to discuss include omissions of literature and lack of critical discourse, historical accuracy, questions about the reliance on reliability studies, and critiques of consensus.
Omissions of Literature and Lack of Critical Discourse From 1996 to 1997
Some papers during this time omitted literature that could have informed the authors and potentially led to different conclusions. Such oversights could have been due to limited distribution of literature, poor searching strategies, a lack of indexing of the source material, dismissivism, [226] intraprofessional politics, [27] gatekeeping, [227] or scholastic error. Any of these issues may have occurred in a single paper.
Sometimes references may have been omitted for the authors to support perspectives that were personally or politically motivated. McAulay pointed out problems in the chiropractic literature that stem from this dismissivist approach. [226] Villanueva-Russell claimed that some academics were staging a coup by using journals, lexicon cleansing, and evidence-based standards to control the profession’s identity. [227] This is related to the medicalization of “regular” chiropractic, mentioned by McAulay in 1995. [228] Dismissivism may include a lack of historical references to support positions.
A few articles important to the dialogue on CVS have not been well cited. It is not clear if this is because the sources were difficult to find, locate, or obtain in search engines. PubMed did not include many chiropractic publications until after 2002. Until that time, the Journal of Manipulative and Physiological Therapeutics was the only chiropractic journal included in MEDLINE starting from 1982. Few other indexing systems of the period indexed chiropractic periodicals or else they charged for the use of the service, placing barriers to access the information. Most of these search engines, other than PubMed, required a fee for use. The only search engine that focuses on chiropractic literature, the Index to Chiropractic Literature, was only in print format until 2001, and each issue was released for reference the year after research papers were published. This made it difficult to obtain papers for citation.
The Index to Chiropractic Literature was not released in a web-based and open-access format until 2001. For example, Ruch’s Atlas [15] was cited in only 4 chiropractic journals and 4 nonchiropractic journals, according to Google Scholar. [229–235] Epstein’s works are rarely cited in the literature. [3, 168] Kent’s 1996 review, [9] which proposed the dysafferentation approach to CVS, was followed by a paper by Seaman and Winterstein, titled “Dysafferentation: A Novel Term to Describe the Neuropathophysiological Effects of Joint Complex Dysfunction.” [236] The article references many of the same sources, such as Bogduk and Korr; however, the 1998 article did not cite Kent’s 1996 article. [9, 236]
Keating's and Nelson's articles from this time are well-cited in the literature, but the critiques of their articles are few. [1, 10, 114] This paucity could have many reasons, such as apathy, journal bias, gatekeeping, and possibly that the articles are considered well written and well referenced without the need for further critique. However, if 88 percent of the profession seemed happy to keep the term subluxation, [237] our profession might have lacked rigorous professional discourse. This was proved further when an article that was dismissive of the historical constructs of CVS [47] went without critical response publications or letters to the editor.
Not citing existing sources about CVS could weaken arguments for or against it. This is evident in Nelson’s article where he stated his opposition to the profession-wide, 3–year-long, consensus process. He wrote:The authors have begun the consensus process apparently assuming that agreement exists that there is a particular type of lesion that is the focus of the chiropractic profession. Obviously, some chiropractors believe in the existence of subluxations, but it is equally obvious that many do not.
Nelson provided no references for this contention, including the references about the widespread consensus across 30 years in the profession (through 1997) about subluxation. [12, 92, 98–100, 215, 238–240]
His critique was written 5 years after the consensus process was complete, suggesting that this information was available. The consensus included dozens of stakeholders from most schools and organizations. [12]
Missing the Neuropathic Perspective
Speransky’s neuropathic theories were integrated into CVS models starting in the 1930s. [241–244] This integration continued into the 1990s by chiropractors who found that the empirical evidence in Speransky’s research and theory was congruent with chiropractic’s central paradigm. [142, 241, 245] Theorists such as B. J. Palmer, [141] Watkins, [30] Janse, [240] Weiant, [246, 247] Verner, [111] Homewood, [44] and Harper included Speransky and other Russian neurophysiology in their models. [248] By the 1960s, the neuropathic perspective dominated the profession. This approach was explained by R. J. Watkins:Hence the classic chiropractic definition of a subluxation can be better stated as an “intervertebral subluxation with consequent neuropathy.” Since this is definitely not always the case there are the following combinations seen and described:
Subluxation—minor muscle imbalance with no consequent neuropathy,
(These usually clear quickly and easily—no vasodilation failure.)Subluxation with consequent neuropathy. (Classic chiropractic specialty.)
Subluxation as a symptom of a neuropathy. (Local or remote)
This type of subluxation as a symptom can initiate further
neuropathies to become a complex chain.Any neuropathy can also exist as a self-perpetuating vicious circle, after the original subluxation has physically disappeared. This emphatically illustrates the critical importance of the time factor. Each patient is the sum total of all prior neurological experience. [30]
Some of the literature of the late 1990s included a neuropathic approach. Epstein incorporated it into his models and also integrated several other Russian neuropathic perspectives from Kositsky, Ukhtomsky, Luria, and Bernstein. [134–136, 155, 249 This neuropathic perspective on the CVS is lacking in much of the recent critical literature. [47, 250–252, 253] This may be in part due to the 1970s research emphasizing pain disorders related to CVS rather than the pathophysiology associated with neurodystrophic and neuropathic processes. [42, 254, 255] Nevertheless, this element of theory should not be ignored and should be included in critical appraisals.
Keating’s body of work used little neuropathic literature. Based on his use of references, Keating’s descriptions of CVS in his early writings did not include a comprehensive review of chiropractic research literature that was published between 1928 and 1980, [59, 61, 256] such as theories about vertebrogenic reflexive pathophysiological processes of CVS theory; Speransky’s theory; or works of R. J. Watkins, B. J. Palmer, Verner, Harper, and Weiant. As Keating’s publications evolved and he eventually mastered some of the historical literature of chiropractic, he did not alter his initial assumptions. [47, 52, 54, 257, 258] His basic arguments remained the same over the course of 30 years of publishing even though he developed those arguments before having referenced a large portion of CVS theories. [59, 60] Keating stated that he did not know how CVS could be studied non-symptomatically or as an overall neural dysfunction. [72]
Keating et al critiqued the use of the term subluxation in the ACC consensus statement as “dogmatic.” [47] In the paper, the authors mentioned parallels to the Russian school of “nervism” in relation to the altered function attributed to CVS; however, they make this connection to dismiss models from “nineteenth century neurology and physiology.” [47] They do not link that line of thought to chiropractic literature classified as Speranskian subluxation theory, which made reference to 20th century neurophysiology research conducted in Russia. [245] Sechenov’s school of nervism was carried forward through research by his students Pavlov and Ukhtomsky, and also by other Russian neurophysiologists, most notably Speranksy. [259]
The paper critiqued the ACC paradigm as embracing “subluxation dogma,” not delineating a more precise definition of how “neural integrity” is compromised, and not demonstrating the empirical evidence about the clinical meaningfulness of CVS. [47] Beyond the lack of reference to the neuropathic perspective, the authors offered a limited viewpoint about what validity claims should be considered as adequate for testing hypotheses and lacked references to historical and recent literature. Including a full spectrum of historical references in modern discussions about CVS is important to ensure arguments are balanced and well cited. This could lead to more complete viewpoints and ideally to testable hypotheses that could be further studied.
Historical Inaccuracies in the Literature
Several of the articles in the literature cited during this time period contain historical inaccuracies. Some historical errors may have been due to barriers to accessing information, which left authors to make conclusions with missing information. Modern technology, such as powerful computer search engines, has allowed for historical facts to emerge from newspaper and archived databases. It is not too late to add updates to the literature by filling in gaps with historical facts.
Keating and Mootz proposed that chiropractors in the 1930s and 1940s were afraid to publicly criticize their own cherished ideas, which they argued led to a lack of reputable research on CVS. [66] The examples given were that chiropractors used the statement “chiropractic works” to prove efficacy and that chiropractors only researched the “how and why” but not effectiveness. [66] They referred to this as part of the insidious dogma. They proposed that chiropractors felt “That chiropractic is a science because it is rational (ie, consistent with basic science), that the validity of chiropractic theory is determined by its plausibility, and that the clinical value of the chiropractic healing art can be judged on the basis of private (unpublished) uncontrolled observations.” [66] The same argument was used by Keating in other articles but these have yet to be critiqued in the literature. [59, 61, 65, 67, 70, 260, 261, 262]
Although it may be true that D. D. Palmer wrote that chiropractic “makes a rational claim upon the afflicted,” [263] chiropractors did not only develop unpublished private models nor did they all suggest that chiropractic was valid only because it was congruent with science and rationale. Verner said it was both; he writes, “Chiropractic is truly scientific and truly rational.” [111] Chiropractors held conferences from the 1920s to the 1960s; tested hypotheses; established labs; published their thoughts on every element of chiropractic in both self-published texts and professional journals and magazines; and developed dozens of theoretical, analytic, diagnostic, and corrective methodologies. Keating and Mootz’s statement has some merit, but perhaps it should not be used to characterize all of the history of CVS research in chiropractic.
In a similar critique, Nelson attributed CVS theory from the early years of the profession, especially the bone-out-of-place model, to D. D. Palmer. [1] As Keating noted, this was not D. D. Palmer’s definition; rather, Palmer emphasized the subluxated joint impinging on a nerve. [71] Thus, Nelson’s conclusion that modern CVS theory should be abandoned if it does not link to D. D. Palmer’s theory may be based on a mistaken interpretation of Palmer’s original theory.
How historical facts are interpreted or presented may influence later publications. An example from the 1996–1997 literature is Keating’s quote of D. D. Palmer about relieving human suffering and how, according to Keating’s interpretation, this could imply that D. D. Palmer included other methods within chiropractic. [72] In writing about this topic in his 1992 paper, [82] Keating requoted and cited from a secondary source, which was page 272 of Rehm’s Necrology. [264] As did Rehm, Keating used the first part of the passage written by D. D. Palmer. Keating wrote about D. D.:His Port Perry, Ontario monument quotes him as saying: ‘I never considered it beneath my dignity to do anything to relieve human suffering’ ([16], p. 272).
Additionally, the founder of chiropractic probably continued in some of the clinical procedures involved in his magnetic healing days (ie, pre-1895)... [72]The original writing by Palmer was on page 322 of his tome in a chapter about adjusting for corns and bunions. D. D. Palmer wrote, “I never felt it beneath my dignity to do anything to relieve human suffering. The relief given bunions and corns by adjusting is proof positive that subluxated joints do cause disease.” [113]
When Keating first used the quote in 1992, [72] perhaps he was unaware of the full statement by D. D. Palmer. Rehm was referring to what was etched into a monument in Ontario, Canada that was dedicated to D. D. Palmer in Ontario. [264] Use of a partial quote placed it out of context.
Misuse of this quote had apparently been a contentious issue for decades. Even as far back as 1957, B. J. Palmer pointed out this matter. He wrote:Frequently, we find FIRST sentence ONLY, quoted, which, by itself, makes it appear that D.D. Palmer believed in and practiced “Anything to relieve human suffering,” such as air, light, heat, water, diet, exercise, vitamins, food supplements, physiotherapy, naturopathy, colonic irrigations, massage, ad infinitum, ad nauseum. The motive of quoting ONE sentence, apart from its text, pretext and context, it to think others justify things THEY do by what D.D. Palmer did NOT believe in and DID NOT do. [265]
Keating quoted from page 322 of Palmer’s original text the entire paragraph in a later publication. [266] However, to the best of this author’s knowledge, Keating never wrote about Palmer’s “felt it below my dignity” comment in its full context. [82] Even though Keating used the full quote in a later paper, he never corrected the literature or pointed out how the partial use of the quote led to inaccuracies in the literature.
In some literature, D. D. Palmer stated that he did not include other methods with chiropractic. For example, in a letter to B. J. in 1902, D. D. Palmer explained how his older methods actually would “undo” his chiropractic adjustment. He wrote:I have no use for those books on “Nature Cure,” as I have been over the whole field and have outgrown them. It is a positive fact that after we Chiropractics have done the right thing, that we should not undo what we have done. I.e. for e.g. Mama has me to treat her Chiro. Then I must treat her Magnetic and undo what I have done. By Chiro. I free the nerves and set them in action, by magnetic I soothe them and quiet them, give them ease. [267]
Documents from D. D. Palmer’s earliest days as a magnetic healer from 1886 until his death in 1913 are available. [148, 268–274] In the documents cited, Palmer did not indicate that chiropractic was anything more than adjusting the articulations to relieve nerve impingement to aid human suffering. Palmer stated that chiropractic was distinct from all methods he had previously studied. [113, 264]
Interpretations such as Keating’s may have led to a misunderstanding of D. D. Palmer’s paradigm, especially when Keating helped to shape historical interpretations of D. D. Palmer. [71] This has the potential to fuel the intraprofessional debates with information that may not be accurate.
In any literature there will be myriad interpretations of material and a continued need to update historical research. Some final points to consider are presented here. Papers by Kent, Boone, and Dobson lack reference to Faye’s earliest edition of his manual from 1980. [5, 9, 275] Faye originated the VSC. [114] Kent referred to Faye’s 1983 edition and assumed that Flesia’s 1982 description of the model predated Faye. [9] Also, Boone and Dobson acknowledged that they were not able to trace the origins of VSC and thus relied on Flesia. [5]
Relying on Reliability Studies
Keating advocated for validity studies as a standard that the profession should focus on regarding examination procedures, particularly those for CVS. [10] In his earlier writings, Keating emphasized the value of other types of research, from case studies to other designs. [59, 70, 276] His call for validity studies seemed to resonate with the profession. However, his references from these early years point to interexaminer reliability studies about low back pain, not to CVS correction.
In at least 3 of his writings, Keating referenced some reliability studies and time series studies from the 1980s to support his argument that CVS detection was not well researched. [56, 58, 103] He shared this perspective with the profession through the literature. For example, in 1988, Keating referred to 3 interexaminer reliability studies from the 1980s when he wrote, “We are not yet able to relate the palpable and manipulable lesion to subluxation theory, in part because we do not yet agree on how to find these spinal boo-boos. The black box of the clinical subluxation has yet to be located, let alone pried open.” [256] This conclusion was based on reliability studies that showed researchers could reproduce their own findings but not one another’s findings.
This shaped Keating’s perspective on CVS research. He continued:It may be that we find so little agreement among examiners in many reliability studies of subluxation-detection because subluxation is not a meaningful clinical entity. Perhaps the greatest value of subluxation theory may be to have encouraged chiropractors to probe for them, and therefore to adjust/manipulate. In this context the success of chiropractic palpators in reproducing their own examination findings and occasional agreement among doctors might be seen as sources of superstitious reinforcement for an erroneous theory of adjustment. [256]
Keating acknowledged in his 1992 book [70] that interexaminer studies were an important place to start even though validity studies are more important. He repeated much of the arguments from that book in his 1996 paper. [10] The limited references do not fully support the assertions Keating made in his paper. [10] There were not enough historical references on chiropractic’s history of CVS research and theory to support such broad assertions.
For example, the references in the introduction to Keating’s article related to low back pain research. [10] Most references in the body of the paper pointed to reliability studies. [103–108] Based on these references, Keating claimed there was no hard evidence for the validity of an operational definition for CVS. [10] He claimed that chiropractic researchers had not established a relationship between CVS and health problems and that “the validity of the chiropractor’s ‘subluxation complex’ has not been studied by chiropractors or anyone else.” [10] Keating stated that there was no standard to compare detection methodologies. In 2001, he continued this perspective when he stated that CVS as a reliably detectable and clinically meaningful phenomenon was untested. [261]
Reliability studies of the future might model the recent studies that emphasize the training and self-review of the examiners. [65, 260] Such studies may point the way to a new era in reliability research and raise the standard through which to assess the adequacy of previous studies. [277, 278]
These new studies may offer an opportunity to redo the research upon which Keating based his original claims. Such studies could be undertaken with new methodology, which was developed by Holt et al [277–279] and Cooperstein, et al. [280, 281] Cooperstein et al wrote:It may be possible to repeat many other interexaminer reliability studies, including studies of examination procedures other than motion palpation (thermography, x-ray line marking, etc.) with similar design modifications that may more meaningfully assess examiner agreement than the mostly discrete analysis that has been used up until now. [280]
Research and Critiques of Consensus Definitions
Calls during this period for more adequate and comprehensive operational definitions started with Keating and continued through Nelson, Kent, Boone, and Dobson. [1, 5–7, 9, 70] Various types of studies were proposed, including well-organized case reports, reliability studies, and other research designs. One common theme from this period was that consensus definitions were not valuable for research purposes and that operational and functional definitions were needed. [1, 5, 10] Perspectives on this vary. Boone and Dobson agreed with Keating that operational definitions should replace consensus definitions. [5, 10]
However, they felt investigations should start with functional definitions and then lead to more specific operational definitions to be tested. Consensus definitions should then arise from the research. [5] Kent suggested different operational definitions based on different models and methodologies. [9] Nelson critiqued the process of consensus in general, especially the process that led to Gatterman’s text and the ACC paradigm, while also calling for proposing and testing various hypotheses. [1, 4, 36]
Many types of perspectives could be used to study the myriad ways CVS may influence individuals. Boone and Dobson’s expanded VSM included research proposals that encompass many avenues of health-related quality of life in relation to CVS. [5–7] In 1999, I proposed integration of the VSM and systems science with a somatobiological and psychospiritual view of health. [160] The intent was to capture the emergent psychospiritual aspects of health-related quality of life expression traditionally associated with chiropractic and the adjustment of CVS. [160]
Limitations
This article reflects one person’s interpretation of historical writings and theories. This paper covers concepts and events that are modern enough that they can be reviewed from the perspective of current events, which leaves the historical interpretation open to bias by current perspective. A lack of clear inclusion and exclusion criteria for the material covered in this paper is a limitation that must be noted, as it influences the content, interpretations, and conclusions of the paper. Others may include additional literature or have other opinions that may potentially lead to different conclusions.
Conclusion
This brief period demonstrated that there were perspectives on CVS from streams of discourse in chiropractic’s history of ideas. Rather than focus on limited sets of ideas organized around a handful of practitioners, researchers, or scholars, future developers of the profession could draw upon the spectrum of chiropractic’s complex history. The challenge is to integrate the best from all historical and modern ideas with the rigors of science and the tools of philosophy.
The peak of chiropractic scholarship during this era rested upon prior research and theory. An accurate history of ideas could be used as a critical tool to evaluate the veracity of arguments set in their historical context. No models or theories appeared in a vacuum. Being informed by the history of ideas is a powerful method that we can use to evolve as a profession. In researching the CVS, we should consider exploring plausible hypotheses put forward from chiropractic history.
Practical Applications
This series of articles provides an interpretation of the history and development
of chiropractic vertebral subluxation theories.This series aims to assist modern chiropractors in interpreting the literature and
developing new research plans.Acknowledgments
The author acknowledges Brian McAulay, DC, PhD, David Russell, DC, Donald Epstein, DC, Stevan Walton, DC, and the Tom and Mae Bahan Library at Sherman College of Chiropractic for their assistance.
Funding Sources and Conflicts of Interest
The author received funding from the Association for Reorganizational Healing Practice and the International Chiropractic Pediatric Association for writing this series of papers. No conflicts of interest were reported for this study.
REFERENCES:
C Nelson
The subluxation question
J Chiropr Humanit, 7 (1997), pp. 46-55P Rome
Usage of chiropractic terminology in the literature:
296 ways to say “subluxation”: complex issues of the vertebral subluxation
Chiropr Tech, 8 (2) (1996), pp. 49-80D Epstein
Network spinal analysis: a system of health care delivery within the subluxation-based chiropractic model
J Vert Sublux Res, 1 (1) (1996), pp. 51-59Association of Chiropractic Colleges (ACC) Chiropractic Paradigm
(1996)W Boone, G Dobson
A proposed vertebral subluxation model reflecting traditional concepts and recent advances in health and science
J Vert Sublux Res, 1 (1) (1996), pp. 19-36W Boone, G Dobson
A proposed vertebral subluxation model reflecting traditional concepts and recent advances in health and science: part II
J Vert Sublux Res, 1 (2) (1996), pp. 23-32W Boone, G Dobson
A proposed vertebral subluxation model reflecting traditional concepts and recent advances in health and science: part III
J Vert Sublux Res, 1 (3) (1997), pp. 25-34T Bergmann
Toward a reliable, valid method of manual diagnosis: more than the sum of its P.A.R.T.S
ACA J Chiropr (1997;October), pp. 24-27C Kent
Models of Vertebral Subluxation: A Review
J Vert Sublux Res, 1 (1) (1996), pp. 1-7J Keating
To hunt the subluxation: clinical research considerations
J Manipulative Physiol Ther, 19 (9) (1996), pp. 613-619C Kent, T Rondberg, M Dobson
A survey response regarding the appropriateness of professional practice guidelines to subluxation-based chiropractic
J Vert Sublux Res, 1 (1996), pp. 13-22M Gatterman
Development of chiropractic nomenclature through consensus
J Manipulative Physiol Ther, 17 (5) (1994), pp. 302-309T Bergmann (Ed.),
Proceedings of the first consensus conference on validation of chiropractic methods,
J Chiropr Tech, No. 2 (1990)C Kent
An analysis of the General Chiropractic Council’s policy on claims made for the vertebral subluxation complex
Philos Dialogues (May 16, 2011), pp. 1-9W Ruch
Atlas of Common Subluxations of the Human Spine and Pelvis
Life West Press, Hayward, CA (2014)G Cramer, C Scott, N Tuck
The holey spine: a summary of the history of scientific investigation of the intervertebral foramina
Chiropr Hist, 18 (2) (1998), pp. 13-24H Swanberg
The Intervertebral Foramina in Man; The Morphology of the Intervertebral Foramina in Man,
Including a Description of Their Contents and Adjacent Parts,
With Special Reference to the Nervous Structures
Chicago Scientific Publishing Co., Chicago, IL (1915)A Forster
The White Mark: An Editorial History of Chiropractic
National Publishing Association, Chicago, IL (1921)J Janse
In memoriam: Fred W. Illi passes away
ACA J Chiropr (January 1984), pp. 94-95J Winterstein, W Bachop
The corporotransverse ligament at the L5/S1 intervertebral foramen: a gross anatomical-radiographic comparison
Anat Rec, 226 (4) (1990), p. 111aP.A.R.T. guidelines
ACA J Chiropr (December 1999), pp. 44-45T Bergmann, B Finer
Joint Assessment-PARTS
Topics in Clinical Chiropractic 2000; 7 (3): 1–10E Owens
Chiropractic subluxation assessment: what the research tells us
J Am Chiropr Assoc (2002;September), pp. 20-24WR Boone
Editor’s perspective
J Vert Sublux Res, 1 (1) (1996), p. 1Ulrichweb.
Ulrichweb’s global series directory.
Accessed September 24, 2016.Y Villanueva-Russell
Evidence-based medicine and its implications for the profession of chiropractic
Soc Sci Med, 60 (2005), pp. 545-561S Senzon
Chiropractic professionalism and accreditation:
an exploration of conflicting worldviews through the lens of developmental structuralism
J Chiropr Humanit, 21 (1) (2014), pp. 25-48S Senzon, D Epstein, D Lemberger
A historical perspective on network spinal analysis care:
A unique insight into the spine's role in healing and wellbeing
Chiropr J Aust, 45 (4) (2017), pp. 305-323WFC policy statement adoption of the ACC paradigm:
Approved by the Assembly of the World Federation of Chiropractic; Paris, May 23, 2001,
World Federation of Chiropractic (2001)S Walton
The Complete Chiropractor: RJ Watkins, DC, PhC, FICC, DACBR
The Institute Chiropractic, Asheville, NC (2017)J Drain
Chiropractic Thoughts
(3rd ed), Integral Altitude Inc, Asheville, NC (2013)PL Rome
Terminology relating to the vertebral subluxation complex and the manipulative sciences. Part 1
Chiropr J Aust, 45 (2) (2017), pp. 73-89PL Rome
Terminology relating to the vertebral subluxation complex and the manipulative sciences. Part 2
Chiropr J Aust, 45 (2) (2017), pp. 90-130LJ Faye
Motion Palpation of the Spine
Motion Palpation Institute, Huntington Beach, CA (1983)R Dishman
Review of the Literature Supporting a Scientific Basis
for the Chiropractic Subluxation Complex
J Manipulative Physiol Ther 1985 (Sep); 8 (3): 163–174M Gatterman
Foundations of Chiropractic Subluxation
Mosby, St. Louis, MO (1995)J Brantingham
A critical look at the subluxation hypothesis
J Manipulative Physiol Ther, 11 (2) (1988), pp. 130-132R Leach
The Chiropractic Theories: A Textbook of Scientific Research
(3rd ed.), Williams and Wilkins, Baltimore, MA (1994)Panel of Advisors ACA Council on Technic
Chiropractic terminology: a report
J Am Chiropr Assoc, 25 (9) (1988), p. 68D Peterson
Chiropractic glossary of commonly used terms
J Am Chiropr Assoc, 25 (10) (1988), p. 46B Green, C Johnson, J Keating, L Ted, DC Shrader
FICC: a gentle force for improvement in chiropractic.
1998 Lee-Homewood Chiropractic Heritage Award recipient
Chiropr Hist, 18 (1) (1998), pp. 59-66M Goldstein
The Research Status of Spinal Manipulative Therapy:
A Workshop Held at the National Institutes of Health, February 2-4, 1975
Vol. 15, U.S. Department of Health, Education, and Welfare, Bethesda, MD (1975)I Korr
The Neurobiologic Mechanisms in Manipulative Therapy
Springer Science & Business Media, Berlin, Germany (1978)AE Homewood
The neurodynamics of the vertebral subluxation
(3rd ed), Homewood, Wildwood, Canada (1981)E Kimmel
Electro analytical instrumentation: part 2
ACA J Chiropr, VI (S-42) (1972)Leach
The Chiropractic Theories: A Textbook of Scientific Research
(4th ed.), Lippincott Williams & Wilkins (2004)J Keating, K Charton, J Grod, S Perle, D Sikorski, J Winterstein
Subluxation: Dogma or Science?
Chiropractic & Osteopathy 2005 (Aug 10); 13: 17J Grod, D Sikorski, J Keating
Unsubstantiated claims in patient brochures from the largest state, provincial, and national
chiropractic associations and research agencies
J Manipulative Physiol Ther, 24 (8) (2001), pp. 514-519A Fuhr, J Menke
Status of activator methods chiropractic technique, theory, and practice
J Manipulative Physiol Ther, 28 (2) (2005), pp. e1-e20C Good
The Subluxation Syndrome:
A Condition Whose Time Has Come?
J Chiropractic Humanities 2004; 11: 38–43P Huijbregts
The chiropractic subluxation: implications for manual medicine
J Manipulative Physiol Ther, 13 (3) (2005), pp. 139-141J Keating
B.J. of Davenport: The Early Years of Chiropractic
Association for the History of Chiropractic, Davenport, IA (1997)J Keating
The specter of dogma
J Can Chiropr Assoc, 45 (2) (2001), p. 76J Keating
Philosophy in chiropractic.
In: Haldeman S, ed. Principles and Practice of Chiropractic
McGraw Hill Companies, Inc., New York (2005), pp. 77-97J Keating, D Smallie
The science of chiropractic: current status and future directions
Calif Chiropr Assoc J, 28 (1984), pp. 20-21J Keating, K Giljum, M Menke, R Lonczak, W Meeker
Toward an experimental chiropractic: time-series designs
J Manipulative Physiol Ther, 8 (4) (1985), pp. 229-238J Keating, K McCarron, J James, J Gruenberg, R Lonczak
Urobehavioral intervention in the rehabilitation of lower urinary tract dysfunction: a case report
J Manipulative Physiol Ther, 8 (3) (1985), pp. 185-189J Keating, J Seville, W Meeker, et al.
Intrasubject experimental designs in osteopathic medicine: applications in clinical practice
J Am Osteopath Assoc, 85 (3) (1985), pp. 192-203J Keating, C Miller
The science of chiropractic and the big idea
Dyn Chiropr (1986)J Keating, J Nelson, R Mootz
A model for clinical, scientific and educational development
Res Forum, 2 (4) (1986), pp. 103-104J Keating, R Mootz
Five contributions to a philosophy of the science of chiropractic
J Manipulative Physiol Ther, 10 (1) (1987), pp. 25-29J Keating
C.O. Watkins, D.C.: grandfather of the Council on Chiropractic Education
J Chiropr Educ, 2 (3) (1988), pp. 1-9J Keating
Beyond the theosophy of chiropractic
J Manipulative Physiol Ther, 12 (1989), pp. 147-150J Keating
A survey of philosophical barriers to research in chiropractic
J Can Chiropr Assoc, 33 (4) (1989), p. 184J Keating
Philosophical barriers to technique research in chiropractic
Chiropr Tech, 1 (1) (1989)J Keating, R Mootz
The influence of political medicine on chiropractic dogma: implications for scientific development
J Manipulative Physiol Ther, 12 (5) (1989), pp. 393-397J Keating
Rationalism and empiricism vs. the philosophy of science in chiropractic
Chiropr Hist, 10 (2) (1990), pp. 23-27J Keating
Introducing the neurocalometer: a view from the Fountain Head
J Can Chiropr Assoc, 35 (3) (1991), p. 165J Keating, R Brown, P Smallie
TF Ratledge, the missionary of straight chiropractic in California
Chiropr Hist, 11 (2) (1991), pp. 27-38J Keating
Toward a Philosophy of the Science of Chiropractic: A Primer for Clinicians
Stockton Foundation for Chiropractic Research, Stockton, CA (1992)J Keating
The evolution of Palmer’s metaphors and hypotheses
Philos Constructs Chiropr Prof, 2 (1) (1992), pp. 9-19J Keating
Shades of straight: diversity among the purists
J Manipulative Physiol Ther, 15 (3) (1992), pp. 203-209J Keating, R Brown, P Smallie
One of the roots of straight chiropractic: Tullius de Florence Ratledge
J Sweere (Ed.), Chiropractic Family Practice:
A Clinical Manual, Aspen Publishers, Inc.,
Gaithersburg, MD (1992)J Keating, W Rehm
The origins and early history of the National Chiropractic Association
J Can Chiropr Assoc, 37 (1) (1993), pp. 27-51J Keating
Purpose-straight chiropractic: not science, not health care
J Manipulative Physiol Ther, 18 (6) (1995), pp. 416-418J Keating, B Green, C Johnson
“Research” and “Science” in the first half of the chiropractic century
J Manipulative Physiol Ther, 18 (6) (1995), pp. 357-378J Keating, W Rehm
William C. Schulze, MD, DC (1870-1936): From mail-order mechano-therapists to scholarship and
professionalism among drugless physicians
Chiropr J Aust, 25 (1995), pp. 122-128J Keating
The short life & enduring influence of the American Chiropractic Association, 1922-1930
Chiropr Hist, 16 (1) (1996), pp. 50-64J Keating
Letter to the editor
Chiropr Hist, 16 (1) (1996), pp. 13-14J Keating
A critical look at the subluxation hypothesis: to the editor
J Manipulative Physiol Ther, 13 (6) (1990), pp. 350-351M Kaminski, R Boal, R Gillette, D Peterson, T Villnave
A model for the evaluation of chiropractic methods
J Manipulative Physiol Ther, 10 (2) (1987), p. 61Chiropractic in New Zealand:
Report of the Commission of Inquiry
Govt. Printer, Wellington, N.Z. (1979)R Roediger
What happened to behaviorism
APS Obs, 17 (5) (2004), pp. 40-42J Keating
The Effect of Setting and Therapist Contact With Child in Dry Bed Training
for Childhood Nocturnal Enuresis [dissertation].
Psychology, State University of New York, Albany, NY (1981)P Huijbregts
Dr. Joseph C. Keating, PhD, Litt. D (hon), FICC (hon)
J Manipulative Physiol Ther, 15 (4) (2007), pp. 250-251Smallie D.
Email correspondence with Simon Senzon on November 19, 2015.KJ Young
Joseph C. Keating, Jr., Ph.D., Litt. D.(hon), 1950-2007
Clin Chiropr, 10 (4) (2007), pp. 220-221J Keating, A Callender, C Cleveland
A History of Chiropractic Education in North America
Association for the History of Chiropractic (1998)Palmer.edu
Alumni: West campus graduates 30 doctors
https://www.palmer.edu/insights/issue.aspx?v=4&n=1&a=13
(September 23, 2015)D Barlow, S Hayes, R Gray-Nelson
The Scientist Practitioner: Research and Accountability in Clinical and Educational Settings
Pergamon Press, New York (1984)BU.edu
BU: psychological and brain sciences: David H. Barlow, PhD
(September 23, 2016)J Howe
A contemporary perspective on chiropractic and the concept of subluxation
ACA J Chiropr, X (S-165) (1976)AS Gregory
Spinal Adjustment: An Auxillary Method of Treatment
Self-published, Oklahoma City, OK (1910)A Forster
Principles and Practice of Chiropractic
(3rd ed.), The National Publishing Association, Chicago, IL (1923)J Howard
Encyclopedia of Chiropractic (The Howard System)
National School of Chiropractic, Chicago, IL (1912)J Janse, RH Houser, BF Wells
Chiropractic Principles and Technic: For Use by Students and Practitioners
(2nd ed), National College of Chiropractic, Chicago, IL (1978)R Phillips
Joseph Janse: The Apostle of Chiropractic Education
R. Phillips, Los Angeles, CA (2006)Phillips
The irritable reflex mechanism
ACA J Chiropr, VIII (S-9) (1975)H Bittner, W Harper, A Homewood, J Janse, C Weiant
Chiropractic of today
ACA J Chiropr, VII (S-82) (1973)ACA
Chiropractic terminology: a report of the ACA Council on Technic
ACA J Chiropr (October 1988), pp. 46-75International Chiropractor’s Association definition of subluxation,
ICA, Washington, DC (1987)Internet Search of and CINAHL Database and Pubmed archives (October 5, 2015)
P Boline, J Keating, J Brist, G Denver
Interexaminer reliability of palpatory evaluations of the lumbar spine
Am J Chiropr Med, 1 (1) (1988), pp. 5-11K Deboer, R Harmon Jr., C Tuttle, H Wallace
Reliability study of detection of somatic dysfunctions in the cervical spine
J Manipulative Physiol Ther, 8 (1) (1985), pp. 9-16K J, P Boline
Inter- and intra-examiner reliability of motion palpation for the thoracolumbar spine
J Manipulative Physiol Ther, 11 (53-56) (1988)MR Wiles
Reproducibility and interexaminer correlation of motion palpation findings of the sacroiliac joints
J Can Chiropr Assoc, 24 (2) (1980), p. 59Z Zachman, AD Traina, J Keating, S Bolles, L Braun-Porter
Interexaminer reliability and concurrent validity of two instruments of the measurement of cervical ranges of motion
J Manipulative Physiol Ther, 12 (3) (1989), pp. 205-210P Boline, J Keating, M Haas, A Anderson
Interexaminer reliability and discriminant validity of inclinometric measurement of lumbar rotation
in chronic low back pain patients and sbujects without low back pain
Spine, 17 (1992), pp. 335-338LJ Faye
Spinal Motion Palpation and Clinical Considerations of the Lumbar Spine and Pelvis: Lecture Notes
Motion Palpation Institute, Huntington Beach, CA (1986)C Lantz
Vertebral subluxation complex: basic model and clinical application
Dyn Chiropr, 11 (1997)J Verner
The Science and Logic of Chiropractic
(8th ed), Dr. P.J. Cerasoli, Brooklyn, NY (1956)W Harper
Anything Can Cause Anything: A Correlation of Dr. Daniel David Palmer’s Priniciples of Chiropractic
(2nd ed), WD Harper, San Antonio, TX (1974)DD Palmer
The Science, Art, and Philosophy of Chiropractic
Portland Printing House, Portland, OR (1910)LJ Faye
The Subluxation Complex
Journal of Chiropractic Humanities 1999; 9 (1): 1-4About Dr. Ruch
Available at: http://www.williamruchdc.com/index.php/about/
Accessed 28th Sep 2016M McCoy
Book review: Atlas of common subluxation of the human spine and pelvis by William J Ruch, DC
JVSR, 4 (1) (2000), p. 1DD Palmer, BJ Palmer
The Science of Chiropractic
The Palmer School of Chiropractic, Davenport, IA (1906)R Gibbons
Solon Massey Langworthy: keeper of the flame during the ‘lost years’ of chiropractic
Chiropr Hist, 1 (1) (1981), pp. 15-21A Forster
Principles and Practice of Spinal Adjustment
The National School of Chiropractic, Chicago, IL (1915)F Illi
The Vertebral Column: Life-line of the Body
National College of Chiropractic, Lombard, IL (1951)A Breig
Biomechanics of the Central Nervous System: Some Basic Normal and Pathologic Phenomena
Almqvist & Wiksell, Stockholm, Sweden (1960)LJ Faye
L. John Faye articles: 1996-1999
Dyn Chiropr (1999)L Ward
The dynamics of spinal stress: spinal column stressology
(3rd ed.), SSS Press, Long Beach, CA (1980)D Epstein
Network chiropractic explores the meningeal critical. Part 2:
“The disc syndrome” and the ultimate release
Dig Chiropr Econ, 89 (1984;Mar/Apr), pp. 144-146C Pert, M Ruff, R Weber, M Herkenham
Neuropeptides and their receptors: a psychosomatic network
J Immunol, 135 (1985), pp. 820s-826sD Epstein
Clinical origin of Network Chiropractic
Paper presented at: Network Chiropractic Modules A B C Intensive.
July 19-21, 1991; Orlando, FL (1991)D Epstein
Theoretical Basis and Clinical Application of Network Spinal Anaylsis (NSA) and Evidence Based Document, Rev. XI
(8th ed), Innate Intelligence, Longmont, CO (2005)S Senzon, D Epstein, D Lemberger
The Network Spinal Wave as a Central Pattern Generator
Paper presented at: International Research and Philosophy Symposium. 2014;
Spartanburg, SC (2014)D Epstein, S Senzon, D Lemberger
Reorganizational healing: a paradigm for the advancement of wellness, behavior change, holistic practice, and healing
J Altern Complement Med, 15 (5) (2009), pp. 475-487D Epstein
Network analysis part I: a unified application of chiropractic principles
Dig Chiropr Econ, 57-58 (1983;March/April), pp. 138-139D Epstein
Network analysis part 2: general review of class B subluxations
Dig Chiropr Econ (1983;July/Aug), pp. 18-23D Epstein
Network chiropractic explores the meningeal critical part I:
anatomy and physiology of the meningeal functional unit
Dig Chiropr Econ, 78-80 (1984;Jan/Feb), p. 82D Epstein
Network Notes: The Network Chiropractic Seminar Your Passport to Excellence
Network Lifeline, Inc., Bellmore, NY (1986)D Epstein
The spinal meningeal functional unit tension and stress adaptation
Dig Chiropr Econ, 29 (3) (1986), pp. 58-60D Epstein
Palpation as a critical tool to detect, classify, and understand central nervous system
pathological dominance and the correlation of these findings to various models of vertebral subluxation
Paper presented at: Academy for Research in the Chiropractic Sciences.
November 4-5, 1989; Philadelphia, PA (1989)D Epstein
The chiropractic clear out: establishing the non-dominant dominant
Wiseworld Seminars Archives (unpublished) (1990)D Epstein
The human organism as a dissipating structure
Paper presented at: Network Chiropractic Seminar: Module F.
April 1990; Monterey, CA (1990)D Epstein
Dynamic fluctuations between self and non-self as influenced by the Somatopsychic and Respiratory Waves,
the Network Chiropractic Infinity Model Paper presented at: Certification Level Intensive.
October 1992; Longmont, CO (1992)D Epstein
Network Chiropractic Parameters
Network Chiropractic Module B, Innate Intelligence Inc (1992)D Epstein
Spinal system integrity
Paper presented at: Network Spinal Analysis: Basic Level Intensive.
April 1996; San Francisco, CA (1996)BJ Palmer
Clinical Controlled Chiropractic Research
Vol. 25, Palmer School of Chiropractic, Davenport, IA (1951)A Speransky
A Basis for the Theory of Medicine
International Publishers, New York, NY (1936)H Logan
Logan Basic Methods
Logan, St. Louis, MO (1950)De Jarnette
Sacro Occipital Technic
DeJarnette, Nebraska City, NE (1933)R Cooperstein, B Gleberzon
Technique Systems in Chiropractic
Churchill Livingstone, Philadelphia, PA (2004)BJ Palmer
The Subluxation Specific the Adjustment Specific
Vol. 18, Palmer School of Chiropractic, Davenport, IA (1934)I Korr
The Collected Papers of Irvin M. Korr
American Academy of Osteopathy (1979)DD Palmer
The Chiropractor
Press of Beacon Light Printing Company, Los Angeles, CA (1914)I Toftness
Philosophy of Chiropractic Correction
I.N. Toftness, DC, PhC (1977)LE Ward
The Spinal Column Stressology Manual of Standard Practices
(2nd ed), SSS Press, Long Beach, CA (1980)T Faulkner
Letter to Donny Epstein
Wise World Seminars Archives (unpublished) (1984)A Breig
Adverse Mechanical Tension in the Central Nervous System: An Analysis of Cause and Effect
Almqvist & Wiksell International,
Stockholm, Sweden (1978)G Kositskiy, V Smirnov
The Nervous System and “Stress” (The Principle of Dominance in Pathology)
Nauka Press/NASA, Moscow/Washington, DC (1970/1972)
NASA Technical Translation 653.
Washington, DC: NASA; March 1972.IM Korr
The spinal cord as organizer of disease processes: some preliminary perspectives
J Am Osteopath Assoc, 76 (1) (1976), pp. 35-45D Epstein
The stress connection: gauging the role of the nervous system
Dig Chiropr Econ (1987;Dec/Jan), pp. 58-60H Selye
Stress and Disease
McGraw-Hill, New York (1956)S Grof
Realms of the Human Unconscious
Viking Press, New York (1975)D Epstein, S Senzon, D Lemberger
The seasons of wellbeing as an evolutionary map for transpersonal medicine
Int J Transpers Psychol, 33 (1) (2014), pp. 102-130D Ingber
Tensegrity and mechanotransduction
J Bodyw Mov Ther, 12 (3) (2008), pp. 198-200S Senzon
Causation related to self-organization and health related quality of life expression
based on the vertebral subluxation model, the philosophy of chiropractic, and the new biology
J Vert Sublux Res, 3 (3) (1999), pp. 104-112R Blanks, T Schuster, M Dobson
A retrospective assessment of network care using a survey of self-rated health, wellness and quality of life
J Vert Sublux Res, 1 (4) (1997), pp. 11-27W Boone, R Blanks, T Schuster, B Dobson
An evolving model reflecting Network Spinal Analysis (NSA) research
(1999)R Blanks, T Schuster, M Dobson, M Jaurequi
Assessment of network spinal analysis in retrospective and prospective research design formats
+using a survey of self-reported health and wellness [abstr] Paper presented at: Association for Network Care: Scientific Research Conference.
November 17-18, 2001; Como, Italy (2001)T Schuster, M Dobson, M Jauregui, R Blanks
Wellness lifestyles II: modeling the dynamics of wellness, health lifestyle practices, and network spinal analysis
J Altern Complement Med, 10 (2004), pp. 357-367T Schuster, M Dobson, M Jauregui, R Blanks
Wellness lifestyles I: a theoretical framework linking wellness, health lifestyles,
and complementary and alternative medicine J Altern Complement Med, 10 (2004), pp. 349-356R Blanks
Reorganizational healing: a health change model whose time has come
J Altern Complement Med, 5 (2009), pp. 461-464S Senzon, D Epstein, D Lemberger
Reorganizational healing as an integrally informed framework for integral medicine
J Integr Theory Pract, 6 (4) (2011), pp. 113-130S Senzon, D Epstein, D Lemberger
The network spinal wave as a central pattern generator
J Altern Complement Med, 22 (7) (2016), pp. 544-556S Bohacek, E Jonckheere
Chaotic modeling in network spinal analysis: preliminary report.
Nonlinear canonical correlation with alternating conditional expectation (ACE)
J Vert Sublux Res, 2 (4) (1998), pp. 188-195E Jonckheere, P Lohsoonthorn, V Mahajan
Sensory motor instability and Central Pattern Generator in spinal oscillations
Asian J Control (special issue) (2005)E Jonckheere, P Lohsoonthorn, S Musuvathy, V Mahajan, M Stefanovic
On a standing wave Central Pattern Generator and the coherence problem
Biomed Signal Process Control, 5 (4) (2010), pp. 336-347E Jonckheere, S Bohacek, P Lohsoonthorn
Dynamic modeling of spinal EMG activity
Paper presented at: NSF Southwest Regional Workshop on New Directions in Dynamical Systems,
University of Southern California,
Los Angeles, CA (November 16-19, 2000)E Jonckheere, P Lohsoonthorn, W Boone
Dynamic modeling of spinal electromyographic activity during various conditions
[Session WA-13-3, Biomedical Applications]
Paper presented at: American Control Conference;
June 4-6, 2003; Denver, CO (2003)E Jonckheere, P Lohsoonthorn, V Mahajan
ChiroSensor: an array of noninvasive sEMG electrodes
Paper presented at: Medicine Meets Virtual Reality. January 26-29, 2005; Long Beach, CA (2005)R Martin-del-Campo, E Jonckheere
Stationary regime for standing wave Central Pattern Generator
Paper presented at: 3rd IEEE Global SIP 2015: Symposium on Signal Processing and Mathematical Modeling
of Biological Processes with Applications to Cyber-Physical Systems for Precise Medicine
December 14-16, 2015; Orlando, FL (2015)S Musuvathy
Coherently Interacting Dynamics in the Neuromuscular System
[Dissertation]: Electrical Engineering, University of Southern California (2011)W Boone
Editor’s perspective: the journey ahead
J Vert Sublux Res, 2 (1) (1998), pp. 1-2W Boone
The role of vertebral subluxation
J Vert Sublux Res, 3 (2) (1999), pp. 55-56Editor (Ed.),
In Memoriam: William Ralph Boone, Ph.D., D.C,
Sherman Shares (2010;Dec)M McGregor-Triano
Jurisdictional Control of Conservative Spine Care: Chiropractic Versus Medicine [dissertation]
The University of Texas at Dallas, Dallas, TX (December 2006)G Dobson, R Pistolese
An impairment rating analysis of asthmatic children under chiropractic care
J Vert Sublux Res, 1 (4) (1997), pp. 41-48W Boone
The Effect of Low Salinity on Amino Acid Metabolism in the Tissues of the Common Mud Crab,
Panopeus Herbstii (Milne-Edwards) [dissertation]
Dissertation, University of South Carolina, Columbia, SC (1973)W Boone, D Claybrook
The effect of low salinity on amino acid metabolism in the tissues of the common mud crab,
Panopeus herbstii (Milne-Edwards)
Comp Biochem Physiol A, 57 (1) (1977), pp. 99-106W Boone, E Schoffeniels
Hemocyanin synthesis during hypo-osmotic stress in the shore crab Carcinus maenas (L.)
Comp Biochem Physiol B, 63 (2) (1979), pp. 207-214L Briggs, W Boone
Effects of a chiropractic adjustment on changes in pupillary diameter:
a model for evaluating somatovisceral response
J Manipulative Physiol Ther, 11 (3) (1988), pp. 181-189K Waters, W Boone
The relationship of spinal misalignment elements to muscle imbalance in dance performance
Chiropractic, 1 (2) (1988), pp. 49-58M Stewart, D Riffle, W Boone
Computer-aided pattern analysis of temperature differentials
J Manipulative Physiol Ther, 12 (5) (1989), pp. 345-352M Kale, T Keeter
A mechanical analysis of the side posture and knee-chest specific adjustment techniques
J Vert Sublux Res, 1 (1997), pp. 35-42P Gentempo, C Kent, B Hightower, S Minicozzi
Normative data for paraspinal surface electromyographic scanning using a 25-500 Hz bandpass
J Vert Sublux Res, 1 (1996), pp. 43-50C Kent
Surface electromyography in the assessment of changes in paraspinal muscle activity associated
with vertebral subluxation
J Vert Sublux Res, 1 (1997), pp. 15-24G Dobson
Structural changes in the cervical spine following spinal adjustments in a patient with os odontoideum:
a case report
J Vert Sublux Res, 1 (1) (1996), pp. 1-4M Weber, CS Masarsky
Cervico-thoracic subluxation and hot flashes in a perimenopausal subject: a time series case report
J Vert Sublux Res, 1 (1996), pp. 33-40J Hart
Persistence of vertebral misalignments detected on radiographs of the cervical spine during chiropractic care
J Vert Sublux Res, 1 (1997), pp. 49-53M Shaikewitz
A demographic and physical characterization of cervical spine curvature and degeneration
J Vert Sublux Res, 1 (1996), pp. 41-48HG McCoy, M McCoy
A multiple parameter assessment of whiplash injury patients undergoing subluxation based chiropractic care:
a retrospective study
J Vert Sublux Res, 1 (1997), pp. 51-61R Kessinger
Changes in pulmonary function associated with upper cervical specific chiropractic care
J Vert Sublux Res, 1 (1997), pp. 43-50RL Graham, RA Pistolese
An impairment rating analysis of asthmatic children under chiropractic care
J Vert Sublux Res, 1 (4) (1997), p. 1J Schwartzbauer, J Kolber, M Schwartzbauer, J Hart, J Zhang
Athletic performance and physiological measures in baseball players following upper cervical chiropractic care:
a pilot study
J Vert Sublux Res, 1 (1997), pp. 33-40T Morter, TL Schuster
Changes in salivary pH and general health status following the clinical application of
Bio-Energetic synchronization
J Vert Sublux Res, 2 (1998), pp. 35-42R Kessinger, D Boneva
Changes in visual acuity in patients receiving upper cervical specific chiropractic care
J Vert Sublux Res, 2 (1998), pp. 43-49JM Evans
Differential compliance measured by the function recording and analysis system in the
assessment of vertebral subluxation
J Vert Sublux Res, 2 (1998), pp. 15-22E Miller, P Redmond
Changes in digital skin temperature, surface electromyography, and electrodermal activity in
subjects receiving network spinal analysis care
J Vert Sublux Res, 2 (1998), pp. 1-9P Vanquaethem, J Gould
The use of a numerical point system in the assessment of clinical progress in patients under
subluxation-based chiropractic care: a case study
J Vert Sublux Res, 2 (2) (1996), p. 97G Lee, C Jenson
Remission of hepatocellular carcinoma in a patient under chiropractic care
J Vert Sublux Res, 2 (1998), pp. 125-130JM Evans, DL Collins
The clinical application of differential compliance methodology to joint fixation identification
and resolution using the PulStarFRAS [TM]
J Vert Sublux Res, 2 (1998), pp. 131-136G Stillwagon, K Stillwagon
Vertebral subluxation correction and its affect on thermographic readings:
a description of the advent of the visi-therm as applied to chiropractic patient assessment
J Vert Sublux Res, 1 (4) (1998), pp. 1-2S Kelly, W Boone
The clinical application of surface electromyography as an objective measure of change in
the chiropractic assessment of patient progress: a pilot study
J Vert Sublux Res, 2 (1998), pp. 175-181M Behrendt
Reduction of psoriasis in a patient under network spinal analysis care: a case report
J Vert Sublux Res, 4 (1998), pp. 1-5M McCoy
Editor’s perspective: what role for chiropractic?
4 (1-2) (2000)Chirofutures.
Our founders. Accessed September 24, 2016.M McCoy
Editor’s perspective: research, scholarship & the future of the chiropractic profession
Ann Vertebral Sublux Res (1-2) (2011;Jan)Foundation for Vertebral Subluxation:
Leadership - Christopher Kent DC, JD, PresidentSherman Staff directory:
Christopher Kent D.C., J.DS Haldeman, K Hammerich
The evolution of neurology and the concept of chiropractic
ACA J Chiropr, VII (S-57) (August 1973), p. 60RJ Watkins
Subluxation terminology since 1746
J CCA (Fall 1968)
S Walton (Ed.), The Complete Chiropractor: RJ Watkins, DC, PhC, FICC, DACBR,
The Institute Chiropractic,
Asheville, NC (2017), pp. 271-279A Terrett
The search for the subluxation: an investigation of medical literature to 1985
Chiropr Hist, 7 (1) (1987), pp. 29-33R Stephenson
Chiropractic Textbook
Vol. 14, Palmer School of Chiropractic, Davenport, IA (1927)C Lantz
The Vertebral Subluxation Complex PART 1:
An Introduction to the Model and Kinesiological Component
Chiropractic Research Journal 1989; 1 (3): 23-36C Lantz
The Vertebral Subluxation Complex PART 2:
The Neuropathological and Myopathological Components
Chiropractic Research Journal 1990; 1 (4): 19-38GJ Dobson
Curriculum vitae (2016)GJ Dobson
Manual muscle testing combined with specific head positions and other articular challenges
as an assessment of vertebral subluxation: A descriptive paper
J Vert Subluxation Res, 3 (2) (1999), pp. 58-64S Haldeman, D Drum
The compression subluxation
J Clin Chiropr Arch, 7 (1971), pp. 10-21A Peterson, RJ Watkins, H Himes, College CMC
Segmental Neuropathy: The First Evidence of Developing Pathology
Canadian Memorial Chiropractic College (1965)S Senzon
Chiropractic and energy medicine: a shared history
J Chiropr Humanit, 15 (2008), pp. 27-54S Senzon
A history of the mental impulse: theoretical construct or scientific reality?
Chiropr Hist, 21 (2) (2001), pp. 63-76B McAulay
Rigor in the philosophy of chiropractic: beyond the dismissivism/authoritarian polemic
J Chiropr Humanit, 12 (2005), pp. 16-32Villanueva-Russell Y.
Caught in the Crosshairs:
Identity and Cultural Authority Within Chiropractic
Soc Sci Med. 2011 (Jun); 72 (11): 1826–1837B McAulay
Neo-institutionalization and professional socialization: the medicalization of “regular” chiropractic
J Straight Chiropr, 1 (1995), pp. 1-7SP Cohen
Sacroiliac joint pain: a comprehensive review of anatomy, diagnosis, and treatment
Anesth Analg, 101 (5) (2005), pp. 1440-1453DE Harrison, R Cailliet, DD Harrison, SJ Troyanovich, SO Harrison
A review of biomechanics of the central nervous system—part III:
spinal cord stresses from postural loads and their neurologic effects
J Manipulative Physiol Ther, 22 (6) (1999), pp. 399-410PL Rome
Neurovertebral influence upon the autonomic nervous system:
some of the somato-autonomic evidence to date
Chiropr J Aust, 39 (1) (2009), p. 2WJ Ruch, BM Ruch
An analysis of pubis symphysis misalignment using plain film radiography
J Manipulative Physiol Ther, 28 (5) (2005), pp. 330-335JD Andrés Ares, G Roca Amatriaín, A Perucho González, C Nieto, D López
Bloqueo y radiofrecuencia de la articulación sacroilíaca
Revista Sociedad Espańola Dolor, 19 (6) (2012), pp. 335-345P Oakley
Influence of axial rotation on chiropractic pelvic analysis
J Manipulative Physiol Ther, 30 (1) (2007), pp. 78-79SJ Panchal Sacroiliac joint injection and radiofrequency denervation
TR Deer, MS Leong, A Buvanendran, V Gordin, PS Kim, SJ Panchal, AL Ray (Eds.),
Comprehensive Treatment of Chronic Pain by Medical, Interventional, and Integrative Approaches,
Springer (2013), pp. 535-542D Seaman, J Winterstein
Dysafferentation: A Novel Term to Describe the Neuropathophysiological
Effects of Joint Complex Dysfunction. A Look at
Likely Mechanisms of Symptom Generation
J Manipulative Physiol Ther 1998 (May); 21 (4): 267-280McDonald W.P., Durkin K.F., Pfefer M.
How Chiropractors Think and Practice:
The Survey of North American Chiropractors
Seminars in Integrative Medicine 2004; 2 (3): 92–98RJ Watkins
Subluxation terminology
J Am Chiropr Assoc (1968;Sept)Committee on Standardization of Chiropractic Principles,
ACA J Chiropr (July 1956), p. 27J Janse
History of the development of chiropractic concepts: chiropractic terminology
M Goldstein (Ed.), The Research Status of Spinal Manipulative Therapy:
A Workshop Held at the National Institutes of Health, February 2-4, 1975,
Vol. 15, U.S. Department of Health, Education, and Welfare,
Bethesda, MD (1975), pp. 25-42H Wright
Take your choice
Chiropractor, 33 (11) (1936)BJ Palmer
Precise, Posture-Constant, Spinograph, Comparative Graphs
Vol. 14, Palmer School of Chiropractic, Davenport, IA (1938)B Lubka
Prof. A.D. Speransky’s research and chiropractic
Chiropractor, 35 (1) (1939), p. 5J Verner
The Science of Chiropractic and Its Proper Place in the New Health Era
Venard Press, Closter, NJ (1939)S Senzon
Chiropractic and systems science
Chiropr Dialogues (2015;December 25), pp. 9-20C Weiant
Medicine and Chiropractic
Chiropractic Institute, New York (1958)C Weiant
Lessons from Speransky: some specific applications of chiropractic
J Natl Chiropr (1942)W Harper
Anything Can Cause Anything: A Correlation of Dr. Daniel David Palmer’s Priniciples of Chiropractic
WD Harper, San Antonio, TX (1964)D Epstein
Treatment of neuromuscular pain syndromes and its production of and exacerbation of central nervous
system pathological dominance
Paper presented at: Network Chiropractic Seminar: Module D -
Neuromuscular treatment. April 11-14, 1990;
Monterey, CA (1990)R Carter
Subluxation-the silent killer
J Can Chiropr Assoc, 44 (1) (2000), p. 9T Mirtz, L Morgan, L Wyatt, L Greene
An epidemiological examination of the subluxation construct using Hill’s criteria of causation
Chiropr Osteopat, 17 (1) (2009), p. 1S Perle
Foundation for anachronistic chiropractic pseudo-religion
New York State Chiropractic Association Newsletter (August 2012), p. 11Reggars J.
Chiropractic at the Crossroads or Are We Just Going Around in Circles?
Chiropractic & Manual Therapies 2011 (May 21); 19: 11IM Korr
The Neurobiologic Mechanisms in Manipulative Therapy
Plenum Press, New York (1977)S Haldeman
Modern Developments in the Principles and Practice of Chriropractic
Appleton-Century-Crofts, New York (1980)J Keating
Science and politics and the subluxation
Am J Chiropr Med, 1 (3) (1988), pp. 107-110J Keating
William D. Harper, Jr., MS, DC: anything can cause anything
J Can Chiropr Assoc, 52 (1) (2008), p. 38J Keating
A brief history of the chiropractic profession
S Haldeman (Ed.), In Principles and Practice of Chiropractic,
McGraw Hill Companies, Inc.,
New York, NY (2005)L Sokolova, A Batuev
A.A. Ukhtomsky and I.P. Pavolov: A controversy or a dialog?
Zhurnal Vysshey Nervnoy Deyatel’nosti im. I.P. Pavlova, 50 (4) (2000), pp. 581-586J Keating
Chiropractic: science and antiscience and pseudoscience side by side
Skeptical Inquirer, 21 (4) (1997), pp. 37-43J Keating
Philosophy and science in chiropractic: essential, inseperable and misunderstood
Eur J Chiropr, 46 (2001), pp. 51-60J Keating
Letter to the editor: Keating comments to Villanueva-Russell
Chiropr Hist, 27 (1) (2007), pp. 7-8DD Palmer
Is chiropractic an experiment?
The Davenport Tmes; (June 14, 1902)W Rehm
Necrology
Who’s Who in Chiropractic (1980)
In: Who's Who in Chiropractic, International. Dzaman F, ed. Littleton, CO:
Who's Who in Chiropractic International Publishing Co.BJ Palmer
History in the Making
Vol. 35, Palmer College, Davenport, IA (1957)J Keating
Early chiropractic education in Oregon
J Can Chiropr Assoc, 46 (1) (2002), p. 39DD Palmer
Letter to B.J. Palmer (May 4, 1902)
T Faulkner (Ed.), The Chiropractor's Protégé:
The Untold Story of Oakley G. Smith's Journey with D.D. Palmer in Chiropractic's Founding Years,
Association for the History of Chiropractic,
Rock Island, IL (2017), p. 103T Waters
Chasing D.D.: D.D. Palmer in the News 1886-1913
Lulu, Inc., Raleigh, NC (2013)T Waters
Fishing for Palmer in What Cheer: D.D. Palmer 1882-1886
Lulu, Inc., Raleigh, NC (2015)T Waters
Chips from Sweet Home: Writings of D.D. Palmer 1869-1881
Lulu, Inc., Raleigh, NC (2013)DD Palmer
Cured by magnetism
The Burlington Daily Hawkeye: Sunday Morning (October 9, 1887)DD Palmer
Cripples cured! The sick get well by magnetism
Ed, Borchert, Printer (1889;June 20)DD Palmer
The Magnetic Cure (1896)DD Palmer
The chiropractic Number 17 (January 1897)LJ Faye
Course Lecture Notes
Motion Palpation Institute, Huntington Beach, CA (1981)J Keating, J Nelson, R Mootz
A model for clinical, scientific and educational development
Res Forum, 2 (4) (1986), pp. 103-104K Holt, D Russell, R Cooperstein, M Young, M Sherson, H Haavik
Inter-examiner reliability of the detection of vertebral subluxation using continuous
measures and confidence levels
Paper presented at: International Research and Philosophy Symposium.
Oct 10-11, 2015; Spartanburg, SC (2015)K Holt, D Russell, N Hoffmann, B Bruce, P Bushell, H Haavik
Interexaminer reliability of a leg length analysis procedure among novice and experienced practitioners
J Manipulative Physiol Ther, 32 (3) (2009), pp. 216-222K Holt, D Russell, R Cooperstein, M Young, M Sherson, H Haavik
Inter-examiner reliability of the detection of vertebral subluxation
using continuous measures and confidence levels Paper presented at: ACC-RAC 2016: Best Practices. March 16-17, 2016;
Orlando, FL (2016)R Cooperstein, M Young, M Haneline
Interexaminer Reliability of Cervical Motion Palpation
Using Continuous Measures and Rater Confidence Levels
J Can Chiropr Assoc. 2013 (Jun); 57 (2): 156–164R Cooperstein, M Haneline, M Young
Interexaminer Reliability of Thoracic Motion Palpation
Using Confidence Ratings and Continuous Analysis
J Chiropractic Medicine 2010 (Sep); 9 (3): 99–106

Return to SUBLUXATION THEORY
Since 4-15-2019

| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |