

The Webster Technique:
A Chiropractic Technique
With Obstetric ImplicationsThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Manipulative Physiol Ther 2002 (Jul); 26 (6): E1–9 ~ FULL TEXT
OPEN ACCESS Pistolese, RA
3201 Ridge Ave, Suite 2,
Point Pleasant, NJ 08742-3468OBJECTIVE: To survey members of the International Chiropractic Pediatric Association (ICPA); regarding the use of the Webster Technique for managing the musculoskeletal causes of intrauterine constraint, which may necessitate cesarean section.
METHODS: Surveys were mailed to 1047 US and Canadian members of the ICPA.
RESULTS: One hundred eighty-seven surveys were returned from 1047 ICPA members, constituting a return rate of 17.86%. Seventy-five responses did not meet the study inclusion criteria and were excluded; 112 surveys (11%) provided the data. Of these 112 surveys, 102 (92%) resulted in resolution of the breech presentation, while 10 (9%) remained unresolved.
CONCLUSION: The surveyed doctors reported a high rate of success (82%) in relieving the musculoskeletal causes of intrauterine constraint using the Webster Technique. Although the sample size was small, the results suggest that it may be beneficial to perform the Webster Technique in month 8 of pregnancy, when breech presentation is unlikely to spontaneously convert to cephalic presentation and when external cephalic version is not an effective technique. When successful, the Webster Technique avoids the costs and/or risks of external cephalic version, cesarean section, or vaginal trial of breech.In view of these findings, the Webster Technique deserves serious consideration in the health care management of expectant mothers exhibiting adverse fetal presentation.
The Full-Text Article:
Introduction
Intrauterine constraint is defined as any force external to the developing fetus that obstructs the normal movement of the fetus. Intrauterine constraint has been casually related to a number of structural defects of the peripheral and craniofacial skeleton of the fetus. [1–10] Taylor [11] and others [12, 13] have described how the forces of intrauterine constraint adversely affect the spine during the prenatal and perinatal periods. Moreover, intrauterine constraint can prevent the developing fetus from attaining a head-down vertex position and achieving a vaginal birth, thereby necessitating a cesarean section delivery.
Nearly 13% of all cesarean deliveries are performed as a result of breech presentation. [14] In the United States, 86% of infants with breech presentation are delivered by cesarean section. [15]
Approximately 3% to 4.6% of all singleton pregnancies result in a breech presentation. [16, 17] The incidence of perinatal mortality with breech presentation is approximately 4 times that of a vertex presentation. [18]
The importance of preventing intrauterine constraint and subsequent cesarean section delivery is apparent, considering current statistics. The United States and Canada have some of the highest rates of obstetric interventions in the world, which boosts the already high cost of obstetric intensive care. [19–21] In Canada, the incidence of cesarean section ranges from 15% to 22%, depending on the province. [19] In the United States, approximately 22% of all births in 1999 were cesarean section deliveries. [20, 22] Cesarean rates varied from 14.8% in Alaska to 27.3% in Mississippi. This marks the third consecutive increase in cesarean rates in as many years. [22, 23] The US rate for primary cesarean delivery increased for the second consecutive year to 15.5%. Even though the percentage of women beginning prenatal care in the first trimester of pregnancy has increased to 83.2%, the low-birth-weight rate has remained unchanged at 7.6%. [22] In addition, the national rate of vaginal birth after cesarean delivery has fallen 17% since 1996. [22, 24]
In 1985 the World Health Organization (WHO) proposed 15% as the highest acceptable limit for cesarean section rates. [25] This figure was based on the cesarean section rates of countries with the lowest perinatal mortality rates. [26] In 1991, this figure was adopted as a goal for the year 2000 by the United States Department of Health and Human Services. [27] Several reports have cited reducing the number of cesareans for breech presentation as a strategy for reaching the Healthy People 2000 goal of a 15% cesarean section rate, [26, 28, 29] a goal the United States failed to reach and a goal which was again adopted as a Healthy People 2010 goal by the Centers for Disease Control and Prevention (CDC) and the United States Department of Health Resources and Services Administration. [30]
While many fetuses in breech presentation before 34 weeks' gestation will convert spontaneously to a cephalic presentation, few will do so after 34 weeks. [31] Reports of the rates of spontaneous version have varied from 0% to 33%, with an average of approximately 9%. [32–44] The number of cesarean sections performed due to breech presentation and dystocia has increased, whereas those attributable to fetal distress have not changed significantly, and elective repeat cesarean delivery rates have declined. [14]
Anecdotal reports [45–49] indicate that the Webster Technique, a chiropractic technique designed to relieve the musculoskeletal causes of intrauterine constraint, has been successful in converting breech presentations to cephalic presentation.
The purpose of this study was to gather information on how widely this technique is used by chiropractors who routinely care for pregnant women, and their reported success rates.
Methods
Study population
Surveys were sent to 1047 members of the International Chiropractic Pediatric Association, Inc (ICPA), throughout the United States and Canada. Members of the ICPA were chosen based on their interest in the care of pregnant women and children.
Intervention
The Webster Technique [45] is a chiropractic technique designed to relieve the musculoskeletal causes of intrauterine constraint. Formerly known as Webster's In-Utero Constraint Technique or Webster's Breech Turning Technique, the Webster Technique was developed by Dr Larry Webster in 1978 and has been described in several texts and professional publications. [46, 49–54] In addition, the technique is taught in several chiropractic colleges and postgraduate chiropractic education programs.
Performance of the Webster Technique involves analysis of the functional and spatial relationship of the bones of the pelvis, and manual correction of aberrant biomechanics through the employment of a light-force chiropractic adjustment of the sacrum (Step 1). The Webster Technique further involves analysis and relief of abdominal muscle tension or spasm (Step 2). Both steps are intended to relieve the potential musculoskeletal causes of intrauterine constraint that may lead to cesarean section or breech delivery.
It is important to stress at this time that the Webster Technique is not to be misconstrued as the practice of obstetrics. The Webster Technique is a specific chiropractic technique intended to relieve a specific musculoskeletal condition, and is well within the chiropractor's scope of practice. [55–60] At no time does the chiropractor attempt to change the position of the fetus, as is done with external cephalic version (ECV), by applying pressure to the mother's abdomen in an attempt to turn the fetus in either a forward or a backward somersault to achieve a more vertex presentation. The chiropractor only attempts to correct a potential cause of intrauterine constraint. Untrained individuals should not attempt the Webster Technique.
Survey instrument
The survey involved 16 questions (Appendix), which provided responses concerning the respondent's practice characteristics (Questions 1 to 4) and knowledge and use of the Webster Technique in the previous 6 months (Questions 5 and 6). Questions 7 to 9 ascertained information regarding the diagnosis of the breech presentation. Questions 10 to 16 required respondents to provide information regarding their use of the technique and the outcome. Breech presentation was considered resolved when the fetus turned to a head-down vertex presentation. Respondents were asked to submit the results of all documented cases, regardless of outcome.
Content validity was initially established by having practitioners certified in the use of the Webster Technique validate the content of the survey relative to its intended purpose. The content was approved unanimously by these practitioners as reflecting the type of issues pertinent to the application of the Webster Technique. Following the study, practitioners reported that they found the questionnaire to be clear and complete, both of which are primary attributes of content validity. [61]
Data analysis
Returned surveys were numerically coded and entered into a spreadsheet program (Microsoft Excel 2000, Version 9.0.2720; 1985 to 1999). Responses were analyzed for percentages of outcomes.
Results
One hundred eighty-seven surveys were returned from 1047 US and Canadian members of ICPA, constituting a return rate of 17.86%. The sample size was sufficient to allow estimation of the probability that practitioners would respond in the affirmative or negative with an error of less than 5% (P < .05). [62]
Of the 187 responses, 25 were excluded because the practitioners did not provide care for pregnant women with a breech presentation (Questions 3 and 4). Eight respondents were excluded because they did not know the Webster Technique (Questions 5), and 18 were excluded because they did not use the Webster Technique in their practices in the prior 6 months (Question 6). Five subjects were excluded because they underwent ECV after having the Webster Technique performed (Question 12). In addition, 19 were excluded because they had a condition that physically prevented the fetus from turning, such as oligohydramnios, placenta previa, short umbilical cord, twins, uterine anomalies, etc (Questions 14 and 15) (Table 1).
Table 1. Summary of excluded responses
Reason responses were excluded # Answered No to question #3—Did not provide care for pregnant women. 25 Answered No to question #5—Did not know the Webster Technique. 8 Answered No to question #6—Did not use the Webster Technique. 18 Answered Yes to question #12—Required further intervention (ECV) to resolve the breech presentation. 5 Answered Yes to question #14—Oligohydraminos 4 Answered Yes to question #14—Placenta previa 1 Answered Yes to question #14—Short umbilical cord 5 Answered Yes to question #14—Twins 7 Answered Yes to question #14—Uterine anomalies 2 Total Excluded 75 This left a pool of 112 respondents from which to derive data (11%).
Of these 112 responses, all indicated that they were licensed chiropractors, graduates of accredited chiropractic colleges, and provided care for pregnant women with a breech presentation (Questions 1–4). All 112 respondents reported they were knowledgeable in the use of the Webster Technique and had performed the technique in the previous 6 months (Questions 5 and 6). Of the 112 cases of breech presentation, 92 were medically diagnosed, 12 were not medically diagnosed, and in 8 cases it was unknown if the diagnosis was made medically (Question 7). Furthermore, 104 respondents indicated that diagnosis of breech presentation was made by a certified nurse/midwife or other health care provider, while 3 were not diagnosed by such a professional, and in 5 cases it was unknown who made the diagnosis (Question 9). In 53 reported cases, fetal ultrasound confirmed the diagnosis of breech presentation, while 31 did not use ultrasound, and in 28 cases it was unknown if ultrasound was used in the diagnosis (Question 8). The discrepancy between the number of diagnoses made by a nurse/midwife and those diagnosed medically (Questions 7 and 9) led us to believe that in some cases lay midwives were consulted in lieu of certified nurse midwives or other health care professionals.
All 112 respondents indicated that they employed the Webster Technique (Question 10), of which 102 (92%) resulted in resolution of the breech presentation, while 10 (9%) remained unresolved (Question 12). The Webster Technique was performed on 16 patients in month 7 of pregnancy, on 51 patients during month 8, and on 45 patients during month 9. The Webster Technique resulted in resolution of the breech presentation in 14 of 16 responses when performed in month 7 of pregnancy, in 50 of 51 when performed in month 8, and in 38 of 45 when performed in month 9 of pregnancy (Table 2).
Table 2. Analysis of responses of resolution status
Month performed Number of responses Percent of responses Number resolved Number unresolved 7 16 14.3 14 2 8 51 45.5 50 1 9 45 40.2 38 7 Total 112 100 102 10 The surveyed doctors reported 98 cases of a subsequent vaginal unassisted birth, 12 reported cases of cesarean section delivery, 1 reported that birth was achieved with the additional use of forceps, and 1 reported that birth was achieved with the additional use of vacuum extraction (Question 13). Lastly, 34 reported that the fetus had achieved a head-down vertex position within 24 hours of performance of the Webster Technique, while 24 converted within 2 to 6 days, and 41 converted within 1 to 2 weeks. In 3 cases, the interval between use of the technique and conversion was unknown, and in 10 cases there was no conversion (Question 16).
Discussion
The pelvic bowl consists of the two innominate bones, the sacrum and the coccyx, and connective tissues. [66, 67] The sacroiliac joint is described as both diarthrotic and amphiarthrotic [66–68] and moves with rotation around a Y-axis. [69–71] During pregnancy and parturition, the ligaments of the pelvis relax in order to permit a spreading of the bones. [72] Throughout this period the movement of the sacrum is multidirectional for 1 to 3 mm.70 When the sacrum is in a neutral position relative to the right and left innominates, the pelvic bowl has a uniform, symmetrical opening (Figure 1).
However, when the sacrum is rotated, its position in relationship to the innominates is altered and the normal perimetry of the pelvic bowl is distorted. Due to the unique diarthrotic and amphiarthrotic nature of the sacroiliac joint, as the sacrum rotates the adjacent ilium moves along one axis of motion either posteroinferiorly or anterosuperiorly. [73–75] This movement is denoted by the change in the position of the posterosuperior iliac spine (PSIS).
In addition, the innominates can rotate around a second axis either externally or internally. [74–76] Internal and external rotation of the ilia with respect to the sacrum is characterized by the changed position of the posterosuperior iliac spine either toward or away from the midline.
Figure 1 is a superior to inferior (S to I) radiographic view of a model demonstrating normal pelvic perimetry. Notice the symmetry and relative roundness of the pelvic bowl with respect to the midline. A model was used for the radiography because of the inherent risk associated with the use of radiography during pregnancy. Moreover, radiographs of nonpregnant patients were not used because it is believed that they would not exhibit the 1– to 3–mm multidirectional movement in the sacroiliac joints that occurs in pregnancy and parturition as described by Schafer. [70]
Figure 2 is an S to I radiographic view of a model demonstrating pelvic perimetry when the ilia have rotated posteroinferiorly and anterosuperiorly, as described above.
Note the lack of symmetry and distortion of the roundness of the pelvic bowl. Observe also the differences in space from the centerline through the pubic symphysis to each lateral aspect of the pelvic bowl. Figure 3 is an S to I radiographic view of a model demonstrating pelvic perimetry when the ilia have rotated externally and internally, as previously described.
Figure 1. Normal unsubluxated
female pelvic bowl.
(Model) S to I view. Note symmetry
and relative roundness of opening.
(Radiograph provided courtesy of
Cherie Goble, DC.)
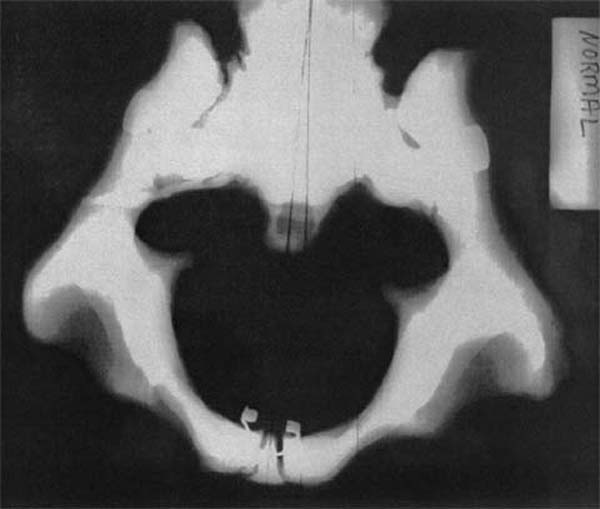
Figure 2. PI/anterosuperiorly
subluxated female pelvic bowl.
(Model) S to I view. Note lack of
symmetry and distortion of
roundness of opening.
Also note difference in
space from centerline
through pubic symphysis.
(Radiograph provided courtesy
of Cherie Goble, DC.)
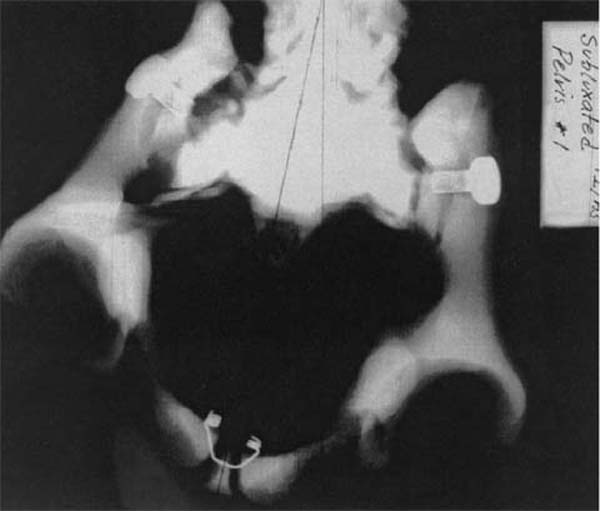
Figure 3. Ex/In subluxated
female pelvic bowl.
(Model) S to I view. Note lack of
symmetry, and distortion of
roundness of the opening.
Also note difference in space
from centerline through
pubic symphysis to right ilium.
(Radiograph provided courtesy of
Cherie Goble, DC.)
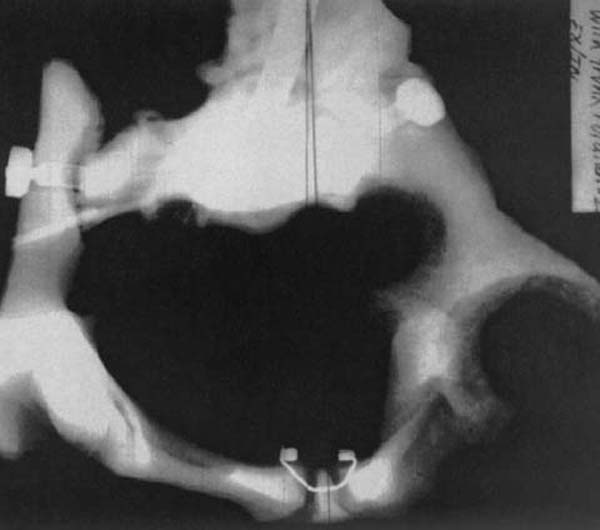
Again, notice the lack of symmetry and distortion of the roundness of the opening. Contrast the difference in space from the centerline through the pubic symphysis to the right ilium as opposed to the left ilium.
There are 3 major ligaments suspending the uterus: the uterosacral, ovarian, and round ligaments. The location of the uterus is dynamically positioned by the stretch of these ligaments.
The uterosacral ligament arises from the posterior wall of the uterus and it inserts on the anterior face of the sacrum at the S2–S3 level. It exerts tension on the cervix in dorsal direction, preventing the body of the uterus from displacing anterior and inferiorly. [63] Uterosacral ligament laxity is almost always associated with uterine prolapse. When the sacrum rotates as described above, it may torque the uterus out of its proper juxtaposition via the change in tension of the uterosacral ligament, resulting in intrauterine constraint.
The low force sacral chiropractic adjustment performed in Step 1 of the Webster Technique is intended to relieve the tension exerted on the uterus due to sacral rotation. Moreover, it is intended to restore the proper perimetry and biomechanics of the pelvic bowl.
The round ligament arises from the fundus of the uterus and proceeds inferolaterally to the labia major, joining up with the inguinal ligament about halfway through its course. [63] The round ligament plays a major role in uterine support as it limits posterior movement of the uterus, thus, maintaining the normal anterior uterine position.
Myofascial trigger points are hyperirritable areas in a muscle or its fascia. The presence of trigger points (myofibrositis) indicates possible nutritional deficiencies to the area resulting from such things as postural and skeletal abnormalities, overloading, fatigue, and/or psychological stress. [77] Myofascial trigger points prevent the full lengthening of a muscle or other fascia and may be latent, eliciting pain only upon palpation. [78] The presence of a myofascial trigger point, as evidenced by a palpable nodule in the area of the round ligament is thought to further torque the uterus out of its proper juxtaposition. This also contributes to the forces of intrauterine constraint.
In the second step of the Webster Technique, the woman's lower abdomen is palpated for nodules, taut bands, edema, adhesions, or tenderness in the area of the round ligament as it passes inferomedially of the anterosuperior iliac spine. Upon location, light effleurage trigger point therapy is performed to release latent or acutely painful muscle nodules. The efficacy of trigger point therapy is well supported by the medical literature and appears in many physical medicine and rehabilitation texts. [77, 79–81] It should be noted that the Webster Technique does not employ the use of cryogenics, electrotherapy, ultrasound, or pharmaceuticals as the effect of these modalities on the developing fetus remains largely undetermined.
Conversely, ECV involves applying pressure to the mother's abdomen in order to turn the fetus in either a forward or a backward somersault to achieve a more vertex presentation. The goal of ECV is to increase the proportion of vertex presentation in fetuses that were formerly in breech position near term. With selective screening, ECV has been reported to be 38.4% to 65% effective. [28, 82–84] External cephalic version before term, at less than 37 weeks, has not been shown to be effective. [83, 85]
The additional use of tocolytic agents during ECV improves the success rate only slightly. [86–88] However, most studies involving tocolysis are not randomized trials, [40] and the benefits of tocolysis remain unproven. [89, 90] Moreover, the safety of tocolytic agents remains controversial at best. [91]
Even with the use of tocolysis, ECV has been associated with abruptio placentae, [84, 92] fetal bradycardia, [88–93] prenatal cranial hemorrhage, [94] umbilical cord prolapse, [33, 95] vaginal bleeding, [84] and even death. [96, 97] While the incidence of serious complication associated with ECV may be low, the potential is present. Currently, the American College of Obstetricians and Gynecologists recommends that ECV only be attempted in settings in which cesarean delivery services are readily available. [90]
Conclusion
The doctors surveyed in this study reported a high rate of success with the Webster Technique (82%). Although the sample size was small, the results suggest that it may be beneficial to perform the Webster Technique in month 8 of pregnancy, when breech presentation is unlikely to spontaneously convert to cephalic presentation31 and when ECV is not effective. [83, 85]
This study has some limitations. The response rate of 17.86% is low, and the 11% response rate is inherently subject to bias. In 59 reported cases, the breech presentation was not confirmed with ultrasound, which introduced the potential for medical misdiagnosis. Furthermore, there was no way to objectively confirm how long after employment of the Webster Technique that the resolution of breech presentation occurred (Question 16). Because this was a retrospective trial, the results are subject to recall bias and, consequently, respondents may have reported more socially desirable results, particularly with respect to selection of cases reported. I attempted to limit self-report bias and recall bias by asking respondents to report the results of all documented cases in which the Webster Technique was used in the previous 6 months, regardless of outcome. However, because I relied on retrospective self-report data, the sample size was small, and there were potential design weaknesses, these results should be tempered with caution. Nonetheless, when successful, the Webster Technique avoids the costs and/or risks of ECV, cesarean section, or vaginal trial of breech. In view of these findings, the Webster Technique deserves serious consideration in the management of expectant mothers exhibiting adverse fetal presentation.
I am not suggesting that chiropractic care is a substitute for prudent, proper obstetric care for the expectant mother. Moreover, not all chiropractors are trained in the performance of the Webster Technique. Currently, the ICPA maintains a database of chiropractors certified in the proper performance of the technique.
The results of this study warrant a larger, more extensive observational study on this promising noninvasive technique. Furthermore, it is suggested that the Webster Technique be further investigated regarding its role in the overall health care of pregnant patients.
Return to PEDIATRICS
Since 8–31–2003
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |