

National Clinical Guidelines for Non-surgical Treatment
of Patients with Recent Onset Neck Pain
or Cervical RadiculopathyThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: European Spine Journal 2017 (Sep); 26 (9): 2242–2257 ~ FULL TEXT
Per Kjaer, Alice Kongsted, Jan Hartvigsen, Alexander Isenberg-Jřrgensen, Berit Schiřttz-Christensen, et. al.
Department of Sports Science and Clinical Biomechanics,
University of Southern Denmark,
Campusvej 55, 5230,
Odense M, Denmark.
pkjaer@health.sdu.dk
Purpose: To summarise recommendations about 21 selected non-surgical interventions for recent onset (<12 weeks) non-specific neck pain (NP) and cervical radiculopathy (CR) based on two guidelines from the Danish Health Authority.
Methods: Two multidisciplinary working groups formulated recommendations based on the GRADE approach.
Results: Twelve recommendations were based on evidence and nine on consensus. Management should include information about prognosis, warning signs, and advise to remain active. For treatment, guidelines suggest different types of supervised exercise and manual therapy; combinations of exercise and manual therapy before medicine for NP; acupuncture for NP but not CR; traction for CR; and oral NSAID (oral or topical) and Tramadol after careful consideration for NP and CR.
Conclusion: Recommendations are based on low-quality evidence or on consensus, but are well aligned with recommendations from guidelines from North America. The working groups recommend intensifying research relating to all aspects of management of NP and CR.
Keywords: Cervical radiculopathy; Clinical guideline; Conservative treatment; Neck pain; Non-surgical intervention; Recommendations.
From the Full-Text Article:
Background
Clinical guidelines assist clinicians’ decision-making by providing recommendations for clinical procedures and interventions. The demand for clinical guidelines is steadily growing due to increased focus on evidence-based prioritising of health care services. In recent years, rigorous methods for systematically selecting and appraising the available evidence have been developed and become generally accepted. [1, 2] In 2012, the Danish Finance Act appropriated approximately 11 million EUR for the preparation of evidence-based clinical guidelines. The Danish Health Authority (DHA) was asked to lead formation of the guidelines in collaboration with the country’s foremost experts in specific health areas representing a high burden of disease, high costs, large variability in care, new available technology, a change in indications for treatment, or doubt about the evidence base for established procedures and interventions. A total of 47 guidelines are now completed and in 2015 and 2016, Danish National Clinical Guidelines dealing with non-surgical treatment of recent onset (\12 weeks) non-specific neck pain (NP) [3] and recent onset (\12 weeks) cervical radiculopathy (CR) [4] were published in Danish.
Non-specific NP is defined as pain or discomfort in the neck and/or shoulder girdle with or without pain referred to the arms. [5] In most cases, a precise patho-anatomical cause for NP cannot be established, and therefore, most NP is classified as non-specific when there is no indication of specific pathology such as inflammatory rheumatic disease, osteoporosis, cancer, or radiculopathy.
CR is associated with reduced space in the nerve root canal and/or inflammatory reaction within the nerve root, which is most often triggered by a disc herniation or osseous degeneration of the facet joints. [6] Clinically, it is characterized by arm pain, in some cases paraesthesia and eventually reduced muscle strength, altered sensation and impairment of deep tendon reflexes. [7] The diagnosis of radiculopathy is based on clinical signs and symptoms, and CT scans or MRI can confirm anatomical compromise of the nerve root. [7] Establishing the diagnosis of cervical radiculopathy is, however, challenged by low diagnostic accuracy of clinical tests [8], by a weak association between imaging findings and symptoms [9, 10], and by the phenomenon of referred pain without involvement of a nerve root that can mimic CR. [11] Therefore, at present, there is no firm definition or uniform diagnostic criteria for cervical radiculopathy, and it is challenging to separate cervical radiculopathy fromnon-specific neck pain with referred arm pain. [3, 12]
NP is highly prevalent [13], and globally ranked number four as cause of years lived with disability. [14] Danes with NP visit their general practitioner substantially more often than people without and the costs for treatment and sick leave are approximately 400 million EUR. [15] The prevalence and incidence of CR are uncertain, but a yearly incidence of 0.83 cases per 1000 persons has been estimated in the US. [16]
This paper summarizes the Danish national clinical guidelines for non-surgical treatment of recent onset (\12 weeks) non-specific NP and recent onset (\12 weeks) CR published in Danish by DHA as full reports in Danish in 2015 and 2016. [3, 4] The mandates for the two working groups were to make recommendations concerning a maximum of ten selected interventions for NP and ten selected interventions for CR. The working groups were not asked to make recommendations for diagnostic procedures or care pathways.
Methods
Study design
The clinical guidelines were based on systematic reviews of the scientific literature and subsequent meta-analyses. The evidence of effect was balanced against the risk of harms and patient preferences tomake a recommendation related to each of the clinical questions. The method followed international standards for clinical guidelines [2], which were operationalized in a handbook from DHA and briefly summarized below. [17] This method was based on the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) approach. [1] The full clinical guidelines are available in Danish with all supportive material, including a detailed description of the methods on the DHA webpage. [3, 4, 17]
Organisation of the work
Each project group consisted of a chairman, a project manager, a search specialist, a methodologist, and a lead reviewer. Members of the two multidisciplinary working groups (12 people for NP and 10 people for CR) were appointed following recommendation from professional organisations and scientific societies. The working groups were involved in all parts of the process including formulating the clinical questions, data extraction, risk of bias evaluation, rating the quality of the evidence, and formulating the recommendations. Reference groups with representatives from stakeholders from the Danish health care system (municipalities, regions, and hospitals), and patient organisations discussed and gave feedback and recommendations regarding selection of clinical questions and on the recommendations. The lead reviewers coordinated the tasks of the working groups and drafted the reports. Potential conflicts of interest were declared by all involved and made publicly available on the DHA webpage. [18] Finally, drafts of the clinical guidelines were reviewed by two external peer-reviewers and in a public hearing. Comments and feedback were considered by the working groups and taken into consideration when formulating the final versions of the guidelines.
Formulating the clinical questions
Each clinical guideline addressed a maximum of ten focused clinical questions, which were structured using the patient, intervention, comparison, and outcome approach (PICO). [1]
Populations
The target populations were patients above the age of 18 years with less than 12 weeks of non-specific NP with or without associated arm pain and no signs of CR, or up to 12 weeks of symptoms and clinical signs of CR, respectively. It was assumed that the differentiation between nonspecific NP and radiculopathy is based on a clinical examination without the use of diagnostic imaging. The reasons for choosing interventions in the acute stages were for NP that most people have episodes of relative short duration. [13] Similarly, we consider effects of treatment up to 12 weeks after the initial CR of special interest as patients with CR are recommended to consult a surgeon in case of no improvement after 8–12 weeks. [19]
Interventions and comparisons
The mandate was restricted to non-surgical interventions. The working groups chose interventions based on perceived frequency of use, uncertainty about effectiveness, or uncertainty about superiority of one intervention over another. It was assumed that patients with either NP or CR would receive a basic intervention including information when seeking care. Therefore, the selected interventions for evaluation were to be considered a supplement to basic treatment with no further specification. Trials were, therefore, eligible for inclusion when a basic treatment was provided in both the intervention and control groups, and the intervention under scrutiny was added in one of the groups. By doing so, the effects of adding the interventions in question to the basic treatment were reviewed, and where this was not possible, we accepted placebo- or sham-controlled trials. Because the basic treatment would vary across eligible studies, the phrase ‘in addition to other treatment’ was used in the clinical questions and recommendations. Some of the questions addressed a head-to-head comparison of two treatments when it was assumed that there is frequently a clinical situation with a choice between the two.
Outcome measures
For each of the clinical question, two or more primary outcomes and their timing were chosen a priori. In the Danish version, these are referred to as critical outcomes. The primary outcomes in both guidelines were pain and pain-related activity limitations. For these outcomes, the absolute differences between the intervention and control groups on generally accepted and validated instruments such as a visual analogue scale (VAS), a numeric pain rating scale (NRS), or the neck disability index (NDI) should be available. For questions related to medication, primary outcomes also included serious adverse events, gastrointestinal side effects, and blood pressure increase. Secondary outcomes varied across the two guidelines and included worsening of neurological signs and symptoms, pain at the end of treatment, dropout rates, surgery during the following year, adverse effects, return to work, sick leave, and quality of life. In the Danish version, these are referred to as important outcomes.
Literature searches and inclusion criteria
The literature was systematically searched for each clinical question in three steps. First, Medline, Embase, Pedro, and a recognised national guideline database were searched for clinical guidelines 10 years back (2005 for NP and 2004 for CR). Then, Medline, Embase, Cinahl, Cochrane, and Pedro were searched for systematic reviews 10 years back, and finally, the same databases were searched for randomised clinical trials with no lower limit for the publication year. In case a high-quality systematic review would have covered earlier studies, the date for the last search for this review was used as the lower limit for the new search for primary literature. All the literature searches included studies published until and including March 2016 (NP) or December 2014 (CR), published in English, Norwegian, Swedish, or Danish. The search terms and strategies are available from the DHA homepage. [20, 21]
In case no RCTs were identified concerning recent onset NP, indirect evidence from populations with symptoms lasting more than 12 weeks was included in the guideline. This was not the case for patients with CR, because the condition of long-lasting CR symptoms was considered very different from recent onset CR.
The lead reviewer screened retrieved titles and abstracts. Potentially eligible papers were then collected in full text. Subsequently, the lead reviewer and a member of the working group independently screened the full text papers for inclusion or exclusion. Disagreements were resolved by discussion until consensus was reached.
Data extraction and quality assessment

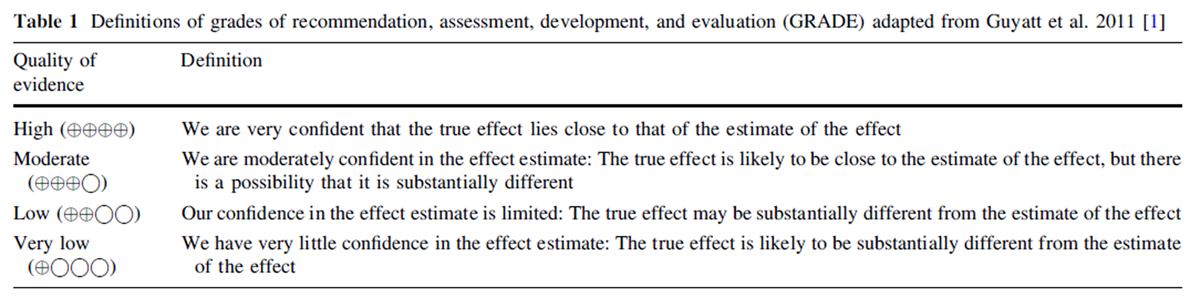
Table 1 The lead reviewers and a member of the working group or a scientific methods advisor independently assessed all included papers for quality and extracted data for each clinical question. If a high-quality systematic review was available, data were extracted from this. The quality was assessed using the AGREE-II tool [22] for clinical guidelines, the AMSTAR tool [23] for systematic reviews, and the Cochrane risk of bias tool for RCTs. [24] When a risk of bias assessment was available from a Cochrane review, it was transferred directly to the clinical guideline. The handling of references and data extractions was performed using the web-based software Covidence [25] fromwhich datawere exported to theRevMan software [26] for meta-analyses, the results of which were further transferred to MAGIC [27] or GradePro [28] for GRADE assessment. [29] Disagreements in data extraction and quality assessment were solved through consensus between the two evaluators. The quality of evidence was graded from high to very low according to the GRADE definitions (B>Table 1) for each of the outcomes. Downgrading was done following the standard definitions of risk of bias, inconsistency, indirectness, imprecision, publication bias, large effect, or plausible confounding. [17, 29] The overall level of evidence supporting the recommendation for each focused question was determined based on the quality for the primary outcome with the lowest quality supporting evidence.
From evidence to recommendations
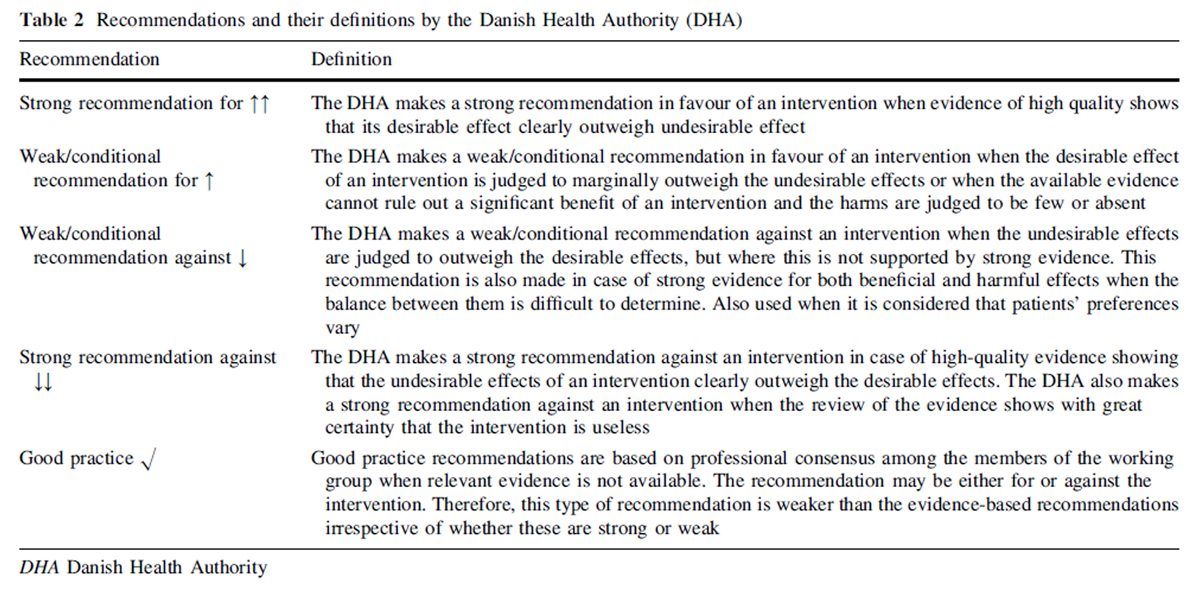
Table 2 The evidence was summarised in evidence tables, and forest plots were constructed when meta-analyses were feasible. Based on the available evidence, strong or weak recommendations for or against an intervention were proposed following the criteria outlined in Table 2. Each recommendation was annotated with the strength of the recommendation and the level of evidence according to GRADE. In case no evidence was available from randomised trials, a good practice recommendation was formulated based on indirect evidence, i.e., evidence from randomised trials in closely related patient populations, or consensus in the working group. Final recommendations were based on weighing the evidence of positive versus negative effects and included patient values and preferences as well as the working-groups’ perceptions and experience.
Results
Table 3 Altogether, the guidelines considered 19 clinical questions. Ten covered recent onset neck pain, while 9 were chosen for CR. Six interventions were covered by both clinical guidelines, namely, information/patient education, NSAIDs, opioids, manual therapy, massage, and acupuncture. Different types of exercise or combinations of exercise (individualised physical activity, motor control exercise, and directional exercise), manual therapy plus supervised exercise, and manual therapy versus medication were addressed slightly different in the two guidelines. An overview of the interventions and the general recommendations is shown in Table 3. None of the questions could be answered by existing clinical guidelines or systematic reviews and recommendations were based on RCTs in 11 of 19 questions and on consensus within the working group in eight of 19. The available evidence from RCTs was in all cases limited and of very low quality, mainly because of either high risk of bias, imprecision, small study samples, indirectness, or inconsistence. Flow charts of included literature [30], risk of bias assessments of clinical guidelines and systematic reviews, and evidence tables are available in Danish at the DHA website. [31, 32]
Specific recommendations
Both for treatment of patients with NP and CR, weak or good clinical practice recommendations were given for information and patient education, advice to stay physically active, different types of supervised exercise, manual therapy alone or in combination with exercise, and weak recommendations were given against massage. The expert groups recommended only using NSAID or tramadol after careful consideration and not as first choices. In patients with NP, the guideline recommends weakly for acupuncture, topical NSAID, and for exercise over NSAID. In patients with CR, there was a weak recommendation for traction and against acupuncture. A short description of eligible studies, primary outcomes, recommendations, and levels of evidence is provided in Tables 4 and 5. Forest plots and risk of bias assessment are provided in Appendix 1 for all outcomes.
General recommendations
Management of people with NP and CR should always contain information about the course of the condition, prognosis, and warning signs as well as encouragement to remain as physically active as possible. In patients with non-complicated or short duration (days to weeks) NP or CR, information and advice may be sufficient. The working groups recommend that choice of any treatment should be done in consideration of patient preferences and that the amount and the intensity of treatment should be proportionate with the duration and level of pain and disability to avoid unnecessary and lengthy treatment. Both patient and health care provider should closely monitor symptoms and clinical signs and adjust treatment plans accordingly. If one of the recommended interventions fails to provide adequate effects, other guideline recommended treatments could be considered. The specific recommendations are summarised in (Tables 4 and 5).
Discussion
Two Danish national clinical guidelines considered 19 clinical questions regarding the management of neck pain and cervical radiculopathy. None of the questions could be answered by referring to existing clinical guidelines or systematic reviews. Recommendations were based on RCTs in 11 of the 19 clinical questions and on consensus in the expert groups in eight of 19. The quality of the available evidence from RCTs was consistently downgraded to very low mainly due to high risk of bias, imprecision, small study samples, and indirectness.
We found a striking lack of evidence for the efficacy of many of the interventions studied, in particular in relation to interventions for CR. Thus, either none or only small and methodologically weak studies gave supportive evidence for the use of interventions, such as information and guidance, medication, directional exercise, massage, acupuncture, motor control exercises, joint mobilisation and manipulation, and cervical traction. Therefore, the CR guideline recommendations are based mainly on indirect evidence and consensus between the members of the working groups. New high-quality clinical research, focusing on these patient groups, is likely to influence future guideline recommendations greatly.
Our recommendations are comparable to those from newer guidelines released in the USA and Canada. [33-35] In 2008, The Orthopaedic Section of the American Physical Therapy Association published clinical practice guidelines relating to assessment of impairment, clinical examination, and interventions in people with NP with and without arm pain [33], which were recently updated. In spite of slightly different definitions of the patient groups, their recommendations for treatment of patients with recent onset NP and mobility deficits were similar to ours and endorse thoracic manipulation, a program of neck range of motion exercises, scapula-thoracic and upper extremity strengthening and eventually cervical manipulation and/or mobilisation. Acupuncture is not recommended in the acute stage of NP. For CR, the American guideline recommends the use of mobilising and motor control exercise as well as nerve mobilisation procedures but not the use of manual mobilisation techniques. Mechanical intermittent traction and acupuncture is now only recommended for the chronic stages. [33] Differences between their and our recommendations may be explained by publication of newer research, and the focus on long-term outcomes in the American guideline. In 2010, North American Spine Society released An evidence-based clinical guideline for the diagnosis and treatment of cervical radiculopathy from degenerative disorders [34] and a summary of the guideline was published in 2011. [7] This guideline included clinical questions about definitions, epidemiology, diagnosis, and a range of interventions, including physical therapy/exercise, manipulation/chiropractic, epidural steroid injections, ancillary procedures as well as a range of surgical interventions and is, therefore, not directly comparable to the new Danish guidelines. Nevertheless, for the interventions covered in both guidelines (exercise therapy and manipulation), comparable levels of evidence for effectiveness were found and recommendations were very similar indicating limited research progress between 2010 and 2015. Finally, the OPTIMa collaboration published an evidence-based guideline for the management of NP and associated disorders including CR. In this guideline structured patient education combined with range of motion exercise, multimodal care (range of motion exercise with manipulation or mobilisation), or muscle relaxants was recommended for patients with recent onset NP, and it was recommended that clinicians not offer structured patient education alone, strain-counterstrain therapy, relaxation massage, cervical collar, electro-acupuncture, electrotherapy, or clinic-based heat. For patients with recent onset CR, clinicians were recommended to consider supervised strengthening exercises in addition to structured patient education but not structured patient education alone, cervical collar, low-level laser therapy, or traction. [35]
In spite of the lack of evidence for benefit or harm for a particular intervention, physicians and professional societies look to expert groups and task forces for guidance. [2] The GRADE methodology has the potential to accommodate such circumstances, because it classifies evidence as either strong or weak and provides interpretations for patients, clinicians, and policy makers. [29] The informed clinician should choose intervention in recognition of how different choices may be appropriate for different patients and that each management decision is consistent with the patients’ values or preferences. [13] The GRADE Working group encourages panels to make recommendations wherever possible whether they are based on solid evidence or not. [17]
Strengths of this national clinical guideline include the commissioning and chairmanship by the DHA and the rigorous adherence to relevant scientific standards. [1, 2] Importantly, the guideline working groups were composed of clinicians and academics with a broad range of professional backgrounds and relevant professional societies and agencies were consulted during the process to ensure the involvement of relevant stakeholders. The guideline working groups were assisted by expert research librarians and by methodologists from the Nordic Cochrane Centre and DHA. Finally, the guideline was peer-reviewed by two international experts who provided detailed comments, which resulted in revisions and clarifications prior to release of the final report.
The main weakness of these national clinical guidelines relates to the lack of high-quality clinical trials in the area, and therefore, recommendations are based on only few studies with a high risk of bias or on consensus in the guideline working groups. In addition, the working groups were limited in the number of clinical questions that they could assess; thus, the influence of individual members of the working and reference groups may have excluded an evaluation of the evidence for other potentially effective interventions. Finally, the mandate prescribed that individual studies could only be included as supportive evidence if they assessed effectiveness of interventions in addition to usual care, which may have lead the working groups to exclude studies that could potentially have strengthened the evidence base of some of the recommendations. However, only 11 RCTs were excluded from the retrieved full text papers in the last step of the study selection process.
Conclusion
Two multidisciplinary working groups were commissioned by DHA to developed new Danish National Clinical Guidelines for non-surgical treatment in patients with recent onset of NP and CR. The recommendations are generally based on weak evidence or on consensus. However, they are well aligned with recommendations from similar guidelines from North America. The guideline working groups strongly recommend to intensify research efforts in relation to all aspects of the management of NP and CR.
Acknowledgements
The authors would like to acknowledge the following members of the project groups and working groups: Karsten Junker, chairman CR working group, research librarians Herdis Foverskov, Kirsten Birkefoss and Conni Skrubbeltrang; lead reviewer Frank Lřnberg; members of the working groups Hans Kristian Lauritsen, Jřrgen Korsgaard, Peter Kryger-Baggesen, and Anne Gram.
Funding
Funding was provided by The Danish Finance Act in 2012, and the DHA was commissioned to formulate the national clinical guidelines based on this. A salary was provided to members of the project groups, i.e., lead reviewers (AK, PK, and FL), project managers (BH and CH), methodologists (KJJ, MJ, and TP), search specialists, and chairmen. The funders had no role in the design, collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the article for public No funding was provided to the working or reference group members.
Conflicts of interest
Potential conflicts of interest have been declared by all involved partners and made publicly available on the DHA webpage (in Danish) [18].
References:
Guyatt GH, Oxman AD, Kunz R, Atkins D, Brozek J, Vist G, Alderson P, Glasziou P, (2011)
GRADE guidelines: 2. Framing the question and deciding on important outcomes.
J Clin Epidemiol 64:395–400.Qaseem A, Forland F, Macbeth F, Ollenschlager G, Phillips S, van der Wees P, (2012)
Guidelines International Network: toward international standards
for clinical practice guidelines.
Ann Intern Med 156:525–531.Sundhedsstyrelsen (2016)
National clinical guideline for the nonsurgical treatment of recent onset non-specific neck pain.
Danish Health Authority, Copenhagen SSundhedsstyrelsen (2015)
National clinical guideline for the nonsurgical treatment of recent onset
nerve root compromise in the neck with symptoms radiating to the arm (cervical radiculopathy).
Danish Health Authority, Copenhagen S, DenmarkFejer R, Kyvik KO, Hartvigsen J (2006)
The prevalence of neck pain in the world population:
a systematic critical review of the literature.
Eur Spine J 15:834–848.Woods BI, Hilibrand AS (2015)
Cervical radiculopathy: epidemiology, etiology, diagnosis, and treatment.
J Spinal Disord Tech 28:E251–E259.Bono CM, Ghiselli G, Gilbert TJ, Kreiner DS, Reitman C, Summers JT, Baisden JL, Easa J, Fernand R, Lamer T, Matz PG, Mazanec DJ, Resnick DK, Shaffer WO, Sharma AK, Timmons RB, Toton JF, North American Spine S (2011)
An evidencebased clinical guideline for the diagnosis and treatment
of cervical radiculopathy from degenerative disorders.
Spine J 11:64–72.Rubinstein SM, Pool JJ, van Tulder MW, Riphagen II, de Vet HC (2007)
A systematic review of the diagnostic accuracy of provocative tests
of the neck for diagnosing cervical radiculopathy.
Eur Spine J 16:307–319.Lee TH, Kim SJ, Lim SM (2013)
Prevalence of disc degeneration in asymptomatic korean subjects. Part 2: cervical spine.
J Korean Neurosurg Soc 53:89–95.Teresi LM, Lufkin RB, Reicher MA, Moffit BJ, Vinuela FV, Wilson GM, Bentson JR, Hanafee WN (1987)
Asymptomatic degenerative disk disease and spondylosis of the cervical spine: MR imaging.
Radiology 164:83–88.Cohen SP (2015)
Epidemiology, diagnosis, and treatment of neck pain.
Mayo Clin Proc 90:284–299.Thoomes EJ, Scholten-Peeters GG, de Boer AJ, Olsthoorn RA (2012)
Lack of uniform diagnostic criteria for cervical radiculopathy
in conservative intervention studies: a systematic review.
Eur Spine J 21:1459–1470.Hoy DG, Protani M, De R, Buchbinder R (2010)
The epidemiology of neck pain.
Best Pract Res Clin Rheumatol 24:783–792.DALYs GBD, Collaborators H (2016)
Global, regional, and national disability-adjusted life-years (DALYs)
for 315 diseases and injuries and healthy life expectancy (HALE), 1990–2015:
a systematic analysis for the Global Burden of Disease Study 2015.
Lancet 388:1603–1658.Flachs EM, Statens Institut fF, Sundhedsstyrelsen (2015)
Sygdomsbyrden i Danmark: sygdomme.
Sundhedsstyrelsen, KbhRadhakrishnan K, Litchy WJ, O’Fallon WM, Kurland LT (1994)
Epidemiology of cervical radiculopathy. A population-based study
from Rochester, Minnesota, 1976 through 1990.
Brain: J Neurol 117(Pt 2):325–335Sundhedsstyrelsen (2015)
Model for udarbejdelse af Nationale Kliniske Retningslinjer: Metodeha°ndbogen Version 2.1. Danish Health Authority.
https://www.sst.dk/da/nkr/metode/*/media/
B3A4A4BA131243ECA6339D6E46CE3536.ashx
Accessed 6 Jan 2017Sundhedsstyrelsen (2016)
Declarations of conflicts of interests: working group members. Danish Health Authority.
https://www.sst.dk/da/om-os/maal-og-opgaver/habilitet/soeg-
habilitetserklaering?search=%7B04EC71DC-8ED7-449B-B9CC-
FC0E13E97A50}
https://www.sst.dk/da/om-os/maal-og-opgaver/habilitet/soeg-habilitetserklaering
Accessed 27 April 2017Sundhedsstyrelsen (2014)
Specialevejledning for neurokirurgi,
Sagsnr. 41012-14/26.
In. SundhedsstyrelsenSundhedsstyrelsen (2015)
Search strategies recent onset cervical radiculopathy.
Danish Health Authority. Guidelines:
https://www.sst.dk/da/udgivelser/2015/*/media/1936A12325D34DAB 99398D5772D4A600.ashx.
Primary literature:
https://www.sst.dk/da/udgivelser/2015/*/media/
95EA1AF77DF74F809C8E33F5136512B1.ashx
Secondary literature:
https://www.sst.dk/da/udgivelser/2015/*/media/
F6A5E407C3194838B117C04814C26AD9.ashx
Accessed Dec 2015Sundhedsstyrelsen (2016)
Search strategies recent onset nonspecific neck pain.
Danish Health Authority. Guidelines:
https://www.sst.dk/da/udgivelser/2016/*/media/8162C4D0F3CA45A5 B29A8EAA79DFE4A0.ashx.
Primary literature:
https://www.sst.dk/da/udgivelser/2016/*/media/
44FECFF5685B447E8A8C54B7C5BA5B19.ashx
Secondary literature:
https://www.sst.dk/da/udgivelser/2016/*/media/
EBA7B432E173478A928B76555AFFE92D.ashx
Accessed April 2016Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, (2010)
AGREE II: advancing guideline development, reporting and evaluation in health care.
CMAJ 182:E839–E842.Shea BJ, Grimshaw JM, Wells GA, Boers M, Andersson N, Hamel C, Porter AC (2007)
Development of AMSTAR: a measurement tool to assess the methodological quality of systematic reviews.
BMC Med Res Methodol 7:10.Furlan AD, Malmivaara A, Chou R, Maher CG, Deyo RA, Schoene M, Bronfort G (2015)
Updated Method Guideline for Systematic Reviews in the Cochrane Back and Neck Group.
Spine (Phila Pa 1976) 40:1660–1673.Covicence [Online Software].
Covidence Team.
https://www.covidence.org/
Accessed 6 Jan 2017Review Manager (RevMan) [Computer program] (2014)
Version 5.3
In. Copenhagen: The Nordic Cochrane Centre, Cochrane CollaborationMAGIGapp [Online Software].
https://www.magicapp.org/
Accessed 6 Jan 2017GRADEpro [Online Software].
https://gradepro.org/
Accessed 6 Jan 2017Guyatt G, Oxman AD, Kunz R, Brozek J, Alonso-Coello P, Rind D, Devereaux P, Montori VM, Freyschuss B, Vist G (2011)
GRADE guidelines 6: rating the quality of evidence-imprecision.
J Clin Epidemiol. doi:10.1016/j.jclinepi.2011.01.012Sundhedsstyrelsen (2015)
Flowcharts of literature for recent onset cervical radiculopathy. Danish Health Authority.
https://www.sst.dk/da/udgivelser/2015/*/media/
098573A2395A4838BB8135977C83911F.ashx
Accessed 6 Jan 2017Sundhedsstyrelsen (2015)
Supporting material: National clinical guideline for the non-surgical treatment
of recent onset nerve root compromise in the neck with symptoms radiating
to the arm (cervical radiculopathy).
Danish Health Authority.
https://www.sst.dk/da/udgivelser/2015/nkr-cervikal-radikulopati
Accessed 8 Jan 2017Sundhedsstyrelsen (2016)
Supporting material: National clinical guideline for the non-surgical treatment
of recent onset nonspecific neck pain.
Danish Health Authority.
https://www.sst.dk/da/udgivelser/2016/nkr-nakkesmerter
Accessed 8 Jan 2017Childs JD, Cleland JA, Elliott JM, Teyhen DS, Wainner RS, Whitman JM, Sopky BJ (2008)
Neck pain: clinical practice guidelines linked to the international classification
of functioning, disability, and health from the orthopedic section of the American Physical Therapy Association.
J Orthop Sports Phys Ther 38:A1–A34.North American Spine S (2010)
Diagnosis and treatment of cervical radiculopathy from degenerative disorders.
North American Spine Society (NASS), Burr Ridge (IL)Cote P, Wong JJ, Sutton D, Shearer HM, Mior S, Randhawa K, Ameis A, Carroll LJ (2016)
Cote, P., Wong, J.J., Sutton, D. et al.
Management of Neck Pain and Associated Disorders: A Clinical Practice Guideline
from the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration
European Spine Journal 2016 (Jul); 25 (7): 2000-2022Traeger AC, Hubscher M, Henschke N, Moseley GL, Lee H, McAuley JH (2015)
Effect of primary care-based education on reassurance in patients
with acute low back pain: systematic review and meta-analysis.
JAMA Intern Med 175:733–743.Hasenbring MI, Pincus T (2015)
Effective reassurance in primary care of low back pain: what messages from clinicians are most beneficial at early stages?
Clin J Pain 31:133–136.Derebery J, Giang GM, Gatchel RJ, Erickson K, Fogarty TW (2009)
Efficacy of a patient-educational booklet for neck-pain patients
with workers compensation: a randomized controlled trial.
Spine (Phila Pa 1976) 34:206–213.Hoving JL, Koes BW, de Vet HC, van der Windt DA, Assendelft WJ, van Mameren H, et al.
Manual Therapy, Physical Therapy, or Continued Care by a General Practitioner
for Patients with Neck Pain. A Randomized, Controlled Trial
Annals of Internal Medicine 2002 (May 21); 136 (10): 713–722Andersen LL, Saervoll CA, Mortensen OS, Poulsen OM, Hannerz H, Zebis MK (2011)
Effectiveness of small daily amounts of progressive resistance training
for frequent neck/shoulder pain: randomised controlled trial.
Pain 152:440–446.Akhter S, Khan M, Ali SS, Soomro RR (2014)
Role of manual therapy with exercise regime versus exercise regime alone
in the management of non-specific chronic neck pain.
Pak J Pharm Sci 27:2125–2128Dusunceli Y, Ozturk C, Atamaz F, Hepguler S, Durmaz B (2009)
Efficacy of neck stabilization exercises for neck pain: a randomized controlled study.
J Rehabil Med 41:626–631.Franca DL, Senna-Fernandes V, Cortez CM, Jackson MN, Bernardo- Filho M, Guimaraes MA (2008) Tension neck syndrome treated by acupuncture combined with physiotherapy: a comparative clinical trial (pilot study). Complement Ther Med 16:268–277. doi:10.1016/j.ctim.2008.02.006
Helewa A, Goldsmith CH, Smythe HA, Lee P, Obright K, Stitt L (2007) Effect of therapeutic exercise and sleeping neck support on patients with chronic neck pain: a randomized clinical trial. J Rheumatol 34:151–158 (pii: 0315162X-34-151)
Rendant D, Pach D, Ludtke R, Reisshauer A, Mietzner A, Willich SN, Witt CM (2011) Qigong versus exercise versus no therapy for patients with chronic neck pain: a randomized controlled trial. Spine (Phila Pa 1976) 36:419–427. doi:10.1097/BRS. 0b013e3181d51fca
Revel M, Minguet M, Gregoy P, Vaillant J, Manuel JL (1994) Changes in cervicocephalic kinesthesia after a proprioceptive rehabilitation program in patients with neck pain: a randomized controlled study. Arch Phys Med Rehabil 75:895–899. doi:10. 1016/0003-9993%2894%2990115-5
Cleland JA, Childs JD, McRae M, Palmer JA, Stowell T (2005) Immediate effects of thoracic manipulation in patients with neck pain: a randomized clinical trial. Man Ther 10:127–135. doi:10. 1016/j.math.2004.08.005
Gonzalez-Iglesias J, Fernandez-de-las-Penas C, Cleland JA, Alburquerque-Sendin F, Palomeque-del-Cerro L, Mendez-Sanchez R (2009) Inclusion of thoracic spine thrust manipulation into an electro-therapy/thermal program for the management of patients with acute mechanical neck pain: a randomized clinical trial. Man Ther 14:306–313. doi:10.1016/j.math.2008.04.006
Gonzalez-Iglesias J, Fernandez-de-las-Penas C, Cleland JA, Gutierrez-Vega Mdel R (2009) Thoracic spine manipulation for the management of patients with neck pain: a randomized clinical trial. J Orthop Sports Phys Ther 39:20–27. doi:10.2519/jospt. 2009.2914
Pikula JR (1999) The effect of spinal manipulative therapy (SMT) on pain reduction and range of motion in patients with acute unilateral neck pain: a pilot study. J Can Chiropr Assoc 43:111–119
Celenay ST, Akbayrak T, Kaya DO (2016) A comparison of the effects of stabilization exercises plus manual therapy to those of stabilization exercises alone in patients with nonspecific mechanical neck pain: a randomized clinical trial. J Orthop Sports Phys Ther 46:44–55. doi:10.2519/jospt.2016.5979
Gert Bronfort DC, PhD; Roni Evans DC; Brian Nelson MD; Peter D. Aker DC, MSc; et al.
A Randomized Clinical Trial of Exercise and Spinal Manipulation
for Patients with Chronic Neck Pain
Spine (Phila Pa 1976). 2001 (Apr 1); 26 (7): 788–797Mejuto-Vazquez MJ, Salom-Moreno J, Ortega-Santiago R, Truyols-Dominguez S, Fernandez-de-Las-Penas C (2014) Shortterm changes in neck pain, widespread pressure pain sensitivity, and cervical range of motion after the application of trigger point dry needling in patients with acute mechanical neck pain: a randomized clinical trial. J Orthop Sports Phys Ther 44:252–260. doi:10.2519/jospt.2014.5108
Birch S, Jamison RN (1998) Controlled trial of Japanese acupuncture for chronic myofascial neck pain: assessment of specific and nonspecific effects of treatment. Clin J Pain 14:248–255
Ilbuldu E, Cakmak A, Disci R, Aydin R (2004) Comparison of laser, dry needling, and placebo laser treatments in myofascial pain syndrome. Photomed Laser Surg 22:306–311. doi:10.1089/ pho.2004.22.306
Irnich D, Behrens N, Gleditsch JM, Stor W, Schreiber MA, Schops P, Vickers AJ, Beyer A (2002) Immediate effects of dry needling and acupuncture at distant points in chronic neck pain: results of a randomized, double-blind, sham-controlled crossover trial. Pain 99:83–89 (pii: S0304395902000623)
Petrie JP, Hazleman BL (1986) A controlled study of acupuncture in neck pain. Br J Rheumatol 25:271–275
Seidel U, Uhlemann C (2002) A randomised controlled doubleblind trial comparing dosed lasertherapy on acupuncture points and acupuncture for chronic cervical syndrome. Deutsche Zeitschrift fur Akupunktur 45:258–269
Thomas M, Eriksson SV, Lundeberg T (1991) A comparative study of diazepam and acupuncture in patients with osteoarthritis pain: a placebo controlled study. Am J Chin Med 19:95–100. doi:10.1142/S0192415X91000156
White P, Lewith G, Prescott P, Conway J (2004) Acupuncture versus placebo for the treatment of chronic mechanical neck pain: a randomized, controlled trial. Ann Intern Med 141:911–919 (pii: 141/12/911)
Witt CM, Brinkhaus B, Reinhold T, Willich SN (2006) Efficacy, effectiveness, safety and costs of acupuncture for chronic pain— results of a large research initiative. Acupunct Med 24:S33–S39
Witt CM, Jena S, Brinkhaus B, Liecker B, Wegscheider K, Willich SN (2006) Acupuncture for patients with chronic neck pain. Pain 125:98–106. doi:10.1016/j.pain.2006.05.013
Cho JH, Nam DH, Kim KT, Lee JH (2014) Acupuncture with non-steroidal anti-inflammatory drugs (NSAIDs) versus acupuncture or NSAIDs alone for the treatment of chronic neck pain: an assessor-blinded randomised controlled pilot study. Acupunct Med 32:17–23. doi:10.1136/acupmed-2013-010410
Sherman KJ, Cherkin DC, Hawkes RJ, Miglioretti DL, Deyo RA (2009) Randomized trial of therapeutic massage for chronic neck pain. Clin J Pain 25:233–238. doi:10.1097/AJP. 0b013e31818b7912
Predel HG, Giannetti B, Pabst H, Schaefer A, Hug AM, Burnett I (2013) Efficacy and safety of diclofenac diethylamine 1.16% gel in acute neck pain: a randomized, double-blind, placebo-controlled study. BMC Musculoskelet Disord 14:250. doi: 10.1186/ 1471-2474-14-250
Institut for RF (2011) N02B Svage analgetika: Rekommandation
Institut for RF (2011) M01 og M09 NSAID, glukosamin og hyaluronsyre: Rekommandation
Institut for RF (2011) N02A Opioider: Rekommandation
Bronfort G, Evans R, Anderson AV, Svendsen KH, Bracha Y, Grimm RH (2012) Spinal manipulation, medication, or home exercise with advice for acute and subacute neck pain: a randomized trial. Ann Intern Med 156:1–10. doi:10.7326/0003- 4819-156-1-201201030-00002
Harboe KM, Jensen MP (2013) Akut uspecifikt lćndehold. Rationel Farmakoterapi 2013
Lćgemiddelstyrelsen (2000) Klinisk rationel smertebehandling. In. pp. 17 februar 2015. http://www.irf.dk/dk/publikationer/ratio nel_farmakoterapi/maanedsblad/2000/rationel_farmakoterapi_ nr_2014_juni_2000_2002.htm
Kay TM, Gross A, Goldsmith CH, Rutherford S, Voth S, Hoving JL, Bronfort G, Santaguida PL (2012) Exercises for mechanical neck disorders. Cochrane Database Syst Rev 8:CD004250. doi:10.1002/14651858.CD004250.pub4
Kuijper B, Tans JT, Beelen A, Nollet F, de Visser M (2009) Cervical collar or physiotherapy versus wait and see policy for recent onset cervical radiculopathy: randomised trial. BMJ 339:b3883. doi:10.1136/bmj.b3883
Ragonese J (2009) A randomized trial comparing manual physical therapy to therapeutic exercises, to a combination of therapies, for the treatment of cervical radiculopathy. Orthop Phys Ther Pract 21:71–76
McKenzie R, May S (2006) The cervical and thoracic spine: mechanical diagnosis and therapy, vol One. Waikanae Spinal Publications, New Zealand
BAPM (1966) Pain in the neck and arm: a multicentre trial of the effects of physiotherapy, arranged by the British Association of Physical Medicine. BMJ 1:253–258
Fritz JM, Thackeray A, Brennan GP, Childs JD (2014) Exercise only, exercise with mechanical traction, or exercise with overdoor traction for patients with cervical radiculopathy, with or without consideration of status on a previously described subgrouping rule: a randomized clinical trial. J Orthop Sports Phys Ther 44:45–57. doi:10.2519/jospt.2014.5065
Jellad A, Ben Salah Z, Boudokhane S, Migaou H, Bahri I, Rejeb N (2009) The value of intermittent cervical traction in recent cervical radiculopathy. Ann Phys Rehabil Med 52:638–652. doi:10.1016/j.rehab.2009.07.035
Young IA, Michener LA, Cleland JA, Aguilera AJ, Snyder AR (2009) Manual therapy, exercise, and traction for patients with cervical radiculopathy: a randomized clinical trial. Phys Ther 89:632–642. doi:10.2522/ptj.20080283

Return to RADICULOPATHY
Return to CHRONIC NECK PAIN
Return to SPINAL PAIN MANAGEMENT
Return to NECK DISORDER GUIDELINES Page
Since 4-23-2021

| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |