

Recognizing Drug Induced Nutrient Depletion
in Chiropractic PracticeThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: The American Chiropractor ~ November 2009
By James B. LaValle, R.Ph., M.S., N.D., C.C.N.Detrimental effects of drugs on nutrition status are a common occurrence but, because they usually occur over time (vs. what is considered an adverse event or allergic reaction, which occurs quickly), they are seldom recognized or corrected. Chiropractic treatment, however, takes place over a much longer time frame. Because of this, doctors of chiropractic are in a unique position to recognize the interactions of medication and nutritional status and, if knowledgeable in the area of drug induced nutrient depletion, they have an opportunity to help their patients recover nutritional adequacy and restore metabolic homeostasis.
Investigational studies on drugs were once tested in locked metabolic wards under the watchful eye of the full range of hospital staff. In the modern era of cost-cutting, clinical trials of new medications almost always involve short-term observations of healthy outpatient volunteers with labs drawn in a fasting state. [1]
Since there is no baseline nutritional analysis in clinical trials of new medications, interactions of medication and nutritional status go undiscovered until after the drug has already been released and is in use. Furthermore, since known existing drug induced nutrient depletions are not taught in medical school curriculums, only a limited number of nutrition related side effects of drugs are ever likely to be observed by a medical practitioner.
In the mainstream literature of pharmacology, drug-nutrient interactions are typically placed in three categories: drug-alcohol interactions, drug-food incompatibility, and drugs affecting nutritional status. [2] Interference of diet with drugs is more likely to be noticed by physicians than interference of drugs with nutrient status. When a medication is expected to be effective in a specified dosage for a specified condition and it is not, the cause is quickly investigated.
For instance, when a patient placed on warfarin (Coumadin) for a few weeks does not test for a longer prothrombin (PT) time, either the doctor or the pharmacist is likely to inquire immediately whether the patient is eating large quantities of green leafy vegetables rich in phylloquinone (vitamin K). The effects of nutrition on medication result in symptoms quickly and are corrected quickly.
The effects of medication on nutrient status, however, can take place more slowly. For example, the liver may require additional nutrient(s) to clear a drug, and this extra demand for the nutrient(s) depletes them over time. If there are no other unusual demands for the nutrients, they may not be depleted while the patient is under a doctor's care. [3] Only when a new stressor is encountered does nutrient depletion become obvious. Likewise, if nutrient status of a person is compromised or marginal, but not deficient before drug therapy is initiated, it may not produce obvious symptoms until after the disease the drug is used to treat has run its course or the patient is on a maintenance dosage.
In addition to the fact that chiropractors tend to have longer term relationships with their patients, chiropractors are trained in nutrition, and many of the nutrient depletions that can occur with different medications have significant impact on issues related to chiropractic care. For example:
Medications may cause electrolyte imbalances, leading to muscle spasm, cramping, palpitations, headaches and muscle weakness.
Mineral and vitamin D deficiencies can lead to osteopenia and osteoporosis.
Several categories of drugs deplete CoQ10, which can affect genetic expression of muscle fibers, neural integrity and energy production.
Nutrient depletion issues can pose as problems in coordination and balance.
So doctors of chiropractic should be keenly aware of these basic principles of nutrient depletion by pharmaceuticals:
Drug Induced Nutrient Depletion (DIND) can alter synthesis, storage, transport, metabolism and excretion of essential vitamins, minerals, fatty acids and amino acids as well as vitamin cofactors.
The amount of each nutrient depleted by drug therapy is dependent on complex factors, such as gender, genetics, absorption, intake and individual lifestyle choices.
Functional deficiencies may not be observed as symptoms, conditions or disease progression for a period of months or years after initiation of drug therapies.
Chronic prescription or over the counter drug use may result in single nutrient or complex vitamin, mineral and cofactor deficiencies.
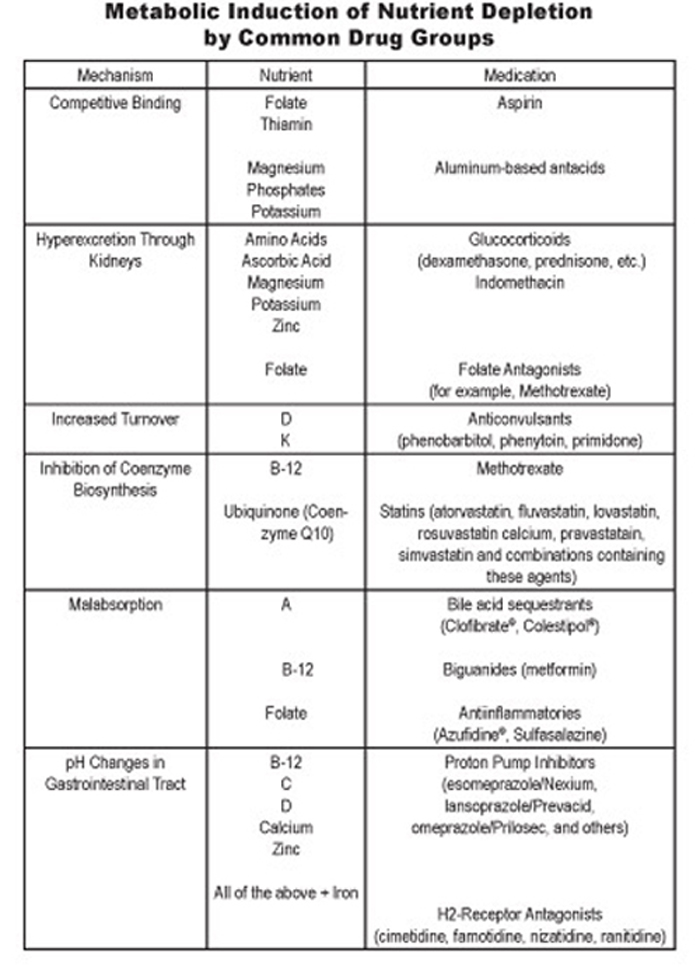
You may also want to refer to our NUTRIENT DEPLETION CHARTS
Examples of Drug Induced Nutrient Depletion
Statin Drugs
I first started educating medical professionals about the ability of statin drugs to deplete CoQ10 back in 1995. While the idea was met with a lot of resistance initially, this has actually become probably the most widely known drug nutrient depletion. CoQ10 is important for cellular energy production; therefore, the effects of depletion of this nutrient are very far reaching. Any organ or tissue that is lacking proper ability to produce adenosine triphosphate (ATP) can be affected, whether it's the large skeletal muscles of the body or an organ, like the heart. CoQ10 is also an important intracellular antioxidant; and, finally, it has been found that CoQ10 is an important nutrient in blood pressure regulation.
I have found that many chiropractors are already well aware of this drug nutrient depletion and have observed effects (like muscle weakness) on many occasions in their patients. So, I will now discuss other lesser-known depletions.
Analgesics
Primary care physicians almost never monitor changes in nutritional status caused by analgesics, and many patients of chiropractors have used analgesics long term. Aspirin and other salicylates deplete folate and thiamin through the mechanism of competitive binding. Folate depletion can go on to influence many areas of health, but one of the most immediate is that it can cause anemia. In addition, folate is one of the key B vitamins needed to recycle and, therefore, to reduce homocysteine.
Most of us know that severe thiamin deficiency results in beriberi, which is typically now only seen in alcoholics. However, since thiamin is critical for ATP production in cells, milder deficiencies can result in tiredness, irritability, and reduced appetite. Moderate deficiency can contribute to neuropathy symptoms like tingling or burning feet and muscle tenderness.
Glucocorticoids and indomethacin cause depletion of ascorbic acid, magnesium, potassium, and zinc through induction of renal hyperexcretion. [4] Ascorbic acid (vitamin C) is needed for collagen building and for immunity. If depleted, a person may notice bleeding gums and increased susceptibility to colds and flu.
Loop Diuretics
Furosemide (Lasix) is well known to deplete potassium, but it also depletes magnesium, thiamin (vitamin B-1), riboflavin (vitamin B-2) and pyridoxine (vitamin B-6). Recent research has found that, not only do patients treated with any dosage of furosemide (Lasix) for any duration typically show deficiency symptoms of these B vitamins, but, providing them with just the Dietary Reference Intake (DRI) did not result in improved vitamin status. [5] People who are on furosemide could begin to have problems with coordination, muscle tremors, double vision and, it has been my experience, they often have immediate improvement just by taking a [higher dose] B complex supplement in addition to taking magnesium and potassium, which are also depleted.
These drugs are just the tip of the iceberg, but are some of the most common drugs used today, and already you can see how profoundly these drugs may be affecting your patients. In the second part of this article, I will discuss three more commonly used drugs and provide a chart that summarizes the nutrient depletions of some of these as well as other prescription and over the counter drugs.
Thiazide Diuretics
Hydrochlorothiazide (HCTZ) depletes magnesium, zinc, CoQ10 potassium and sodium. Side effects of the drug include the development of back pain, anxiety and leg weakness. And long term, it can even contribute to development of Type 2 diabetes. The depletion of magnesium alone can lead to all of the above-mentioned side effects. CoQ10 depletion significantly impacts energy production in cells because it is needed to shuttle carnitine into cells. Since heart cells are very dependent on that constant source of energy, CoQ10 depletion can really affect the heart, in addition to other large muscles. People experiencing CoQ10 depletion will often have noticeable muscle weakness. For example, I have had patients report much more difficulty getting up off the floor or even out of their chair.
I make it a regular practice to put any patients on HCTZ for high blood pressure on magnesium and CoQ10 at the very least; however, it is best if a multi vitamin includes some zinc and that they eat a high potassium diet. The CoQ10 is especially important to prevent the development of congestive heart failure, the very problem you are trying to prevent from the high blood pressure for which this drug is used.Antacids
Proton Pump Inhibitors (PPI's) such as Prilosec (omeprazole), Prevacid (lansoprazole), Aciphex (rabeprazole), and Protonix (pantoprazole) have long been known to deplete vitamin B12 and folic acid. The H2 blocking drugs like Tagamet (cimetidine) and Zantac (ranitidine) also deplete B12 and folate in addition to vitamin D and, because this category of drugs reduces stomach acid, it affects the absorption of the minerals, calcium, iron, and zinc.
These are the second leading category of drugs sold in the United States. While these drugs were intended only for short-term use, many people remain on these drugs for years without monitoring vitamin D status or other symptoms. Studies have now clearly shown a link between use of these drugs and increased risk of osteoporosis. In fact, PPI's now actually carry a warning that they can cause osteoporosis. Typically, women are considered to be a greater risk of osteoporosis; but the studies found that these drugs also dramatically increased the risk in men, as well. So, it is important to be on the lookout for both men and women who are at risk of developing osteoporosis through long-term use of this category of drugs.
Oral Contraceptives
Oral contraceptives, likewise, cause significant chronic nutritional imbalances. In the past, we warned women that oral contraceptives depleted B vitamins, including folate, vitamin C, magnesium, selenium, zinc, and the amino acid tyrosine. Newer studies have found that oral contraceptives also deplete CoQ10. While it is well known that young women need to replace folate after being on birth control before trying to get pregnant, to prevent neural tub defects, it has been my observation that many young women undergo mood changes after going on oral contraceptives, in addition to noticing that they are very tired. Several studies have reported that the B6 depletion results in depression because of the reduced synthesis of serotonin in a subset of women. However, these depletions can lead to a host of problems including anemia, cervical dysplasia, bleeding gums, lowered immunity, and elevated homocysteine.
It has been discussed that these nutrient depletions were observed in older studies in which higher dosages of hormones were used. While I have noticed the effects of lower dosage birth control are not as pronounced as they used to be in the higher hormone dosage pills, depending on the woman's nutritional habits prior to starting the pill, they can still have significant side effects.
The contraceptive Yaz (ethinylestradiol + drospirenone) gets tremendous interest from women and huge ad dollars. This medication has been approved in Europe long enough that the Belgian government financed post-release impact studies. Yaz causes a relative deficiency of zinc by causing accumulation of copper. [7] Other contraceptives are also noted to cause a less severe accumulation of copper, but are better known for the depletions I mentioned above, as well as the disruption of the metabolism of the carotenes and tocopherols. Specifically, oral contraceptives frequently result in depletion of beta-carotene and gamma- (although not alpha-) tocopherol. [8] Depletion of these important anti oxidants could increase a person's risk of any of the diseases related to increased internal inflammation such as heart disease and cancer.
These are just a few examples of how important it is to consider drug actions on metabolism. Doctors of chiropractic are in an enviable position, because they can stop the downward spiral in their patients' health by counseling on drug-induced nutritional depletions and, in so doing, can build patient trust and satisfaction. While this endeavor will require professional supervision of a carefully considered program of nutritional supplementation, appropriate care for nutritional balance will greatly enhance the ability to deliver the results patients expect and deserve.
Dr. James B. LaValle is a clinical pharmacist and board certified clinical nutritionist. He is co-founder of the LaValle Metabolic Institute and an adjunct professor of pharmacy practice at the University of Cincinnati College of Pharmacy and University of South Florida College of Medicine. He is the author of 16 books and has 25 years of clinical experience in pharmaco-nutrition and therapeutics.

Return to PHARMACY
Return to NUTRIENT DEPLETION CHARTS

| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |