

A Prospective Cohort Study of the Impact of Return-to-Work
Coordinators in Getting Injured Workers Back on the JobThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Occup Rehabil. 2018 (Jun); 28 (2): 298–306 ~ FULL TEXT
Tyler J. Lane, Rebbecca Lilley, Sheilah Hogg-Johnson, Anthony D. LaMontagne, Malcolm R. Sim, Peter M. Smith
Department of Epidemiology and Preventive Medicine,
School of Public Health and Preventive Medicine,
Monash University, Level 2,
553 St Kilda Road,
Melbourne, VIC, 3004, Australia.
tyler.lane@monash.edu
BACKGROUND: Work disability is a major personal, financial and public health burden. Predicting future work success is a major focus of research.
OBJECTIVES: To identify common prognostic factors for return-to-work across different health and injury conditions and to describe their association with return-to-work outcomes.
METHODS: Medline, Embase, PsychINFO, Cinahl, and Cochrane Database of Systematic Reviews and the grey literature were searched from January 1, 2004 to September 1, 2013. Systematic reviews addressing return-to-work in various conditions and injuries were selected. Eligible studies were critically appraised using the Scottish Intercollegiate Guidelines Network criteria to identify low risk of bias reviews.
RESULTS: Of the 36,193 titles screened and the 94 eligible studies reviewed, 56 systematic reviews were accepted as low risk of bias. Over half of these focused on musculoskeletal disorders, which were primarily spine related (e.g., neck and low back pain). The other half of studies assessed workers with mental health or cardiovascular conditions, stroke, cancer, multiple sclerosis or other non-specified health conditions. Many factors have been assessed, but few consistently across conditions. Common factors associated with positive return-to-work outcomes were higher education and socioeconomic status, higher self-efficacy and optimistic expectations for recovery and return-to-work, lower severity of the injury/illness, return-to-work coordination, and multidisciplinary interventions that include the workplace and stakeholders. Common factors associated with negative return-to-work outcomes were older age, being female, higher pain or disability, depression, higher physical work demands, previous sick leave and unemployment, and activity limitations.
CONCLUSIONS: Expectations of recovery and return-to-work, pain and disability levels, depression, workplace factors, and access to multidisciplinary resources are important modifiable factors in progressing return-to-work across health and injury conditions. Employers, healthcare providers and other stakeholders can use this information to facilitate return-to-work for injured/ill workers regardless of the specific injury or illness. Future studies should investigate novel interventions, and other factors that may be common across health conditions.
KEYWORDS: Absenteeism; Intervention; Presenteeism; Prognosis; Return to work; Sick leave; Work disability
From the FULL TEXT Article:
Introduction
In 2010, an estimated 313 million people worldwide experienced an occupational injury or disease requiring at least 4 days off work, with a total estimated cost of 4% of global GDP. [1] Time off work due to injury is associated with poorer physical, mental, and social health outcomes, while good quality work—even for those who are ill or recovering — promotes recovery, improves health, and reduces the negative effects of long-term work absence. [2–5] We investigated whether workplace-based return-to-work (RTW) Coordinators can reduce the burden of occupational injury by improving the likelihood of RTW among injured workers.
Throughout North America, Europe, and Australasia, Coordinators manage injured workers’ transition back to the job [6, 7] and are regarded as an important component of successful RTW interventions. [8–10] Known by various titles including rehabilitation coordinator, injury management coordinator, and case manager [11, 12], their common feature is management of the RTW process through workplace assessment, RTW planning, and fostering communication, negotiation, and conflict resolution between injured workers, employers, and other stakeholders. [7, 8, 11–14] Coordinators may be located in the workplace, a government agency, hospital or other healthcare organisation, or be an independent consultant. [6, 7] Interventions that include a Coordinator have shorter disability durations, lower costs, and may improve functioning and quality of life. [8, 9, 15] A recent Cochrane review of 14 randomised controlled trials suggested that compared to usual practice, Coordinators do not improve RTW outcomes. [16] However, the studies in the review were rated at low- to moderate- quality and did not account for different Coordinator activities, which may be an important factor in their impact. For instance, recent research suggests that both management and interpersonal skills are essential for success in the Coordinator role [6, 11, 14, 17], but to our knowledge their impact on RTW outcomes has not been quantitatively assessed.
This paper describes a study of Coordinators in Victoria, Australia, where employers are required to appoint a workplace-based Coordinator from within the organisation. Selection criteria for Coordinators include having sufficient seniority within the organisation and competence to speak on the employer’s behalf and assist them in meeting their RTW obligations. [13] We developed the following research questions to guide this study: do Coordinators’ interpersonal and functional activities improve RTW outcomes? Do their effects vary over time? And are they observed over and above other workplace factors? We hypothesised that better Coordinator interpersonal activities and fulfilment of functional obligations would be associated with better RTW outcomes, and that these associations would be observed over time and over and above other workplace factors.
Methods
Eligibility Criteria
We investigated workplace-based Coordinators’ impact on RTW outcomes using prospective cohort survey data from injured workers in Victoria, Australia. Eligible participants were workers’ compensation claimants with an upper-body musculoskeletal (MSK) or mental health condition who had received at least ten days of workers’ compensation wage-replacement payments, were at least 18 years old, and gave responses to both baseline and 6 month follow-up surveys. Condition type was classified using VCode, the injury and disease classification system for workers’ compensation claims in Victoria. [18] VCode is based on the Type of Occurrence Classification System, which was designed for injury coding in workers’ compensation claims in Australia and incorporates elements of ninth revision of the International Classification of Diseases. [19]
Sampling Strategy and Data Collection
WorkSafe Victoria (WSV), the OHS and workers’ compensation agency for Victorian employers, identified eligible claimants in their claims database beginning in May 2014, at around 5 weeks after their claim had been submitted. Each was sent a primary approach letter informing them of the study and providing an opportunity to opt-out. Contact details of those who did not opt-out were sent to an interviewing agency for data collection. At least six attempts were made to establish contact with eligible claimants over a 2–month period.
Data were collected at two time points: a baseline survey, administered around 4 months post-injury, and a follow- up, administered 6 months later. Baseline interviews were conducted between June 2014 and July 2015 and follow-up interviews between January 2015 and February 2016. The lag between injury and baseline interview was due to time to report injury and lodge claim, time to make claim liability decision, employer excess period (ten working days), the opt-out window, and transfer of information from WSV to interviewing agency. Participants were interviewed using Computer-Assisted Telephone Interviewing. To protect participant privacy, responses were stored in a secure physical location. The final data files were de-identified and stored in a password-protected electronic system. The research team received the de-identified version, which was stored on a password-protected server.
VariablesOutcomes The outcome was whether the participant achieved sustained RTW at the time of interview, assessed at both baseline and follow-up interview. We defined sustained RTW as being back at work for at least 1 month at time of interview (28 days/4 weeks/1 month, depending on the time unit reported) following 10 days of compensated work absence. Sustained RTW was preferred over simple RTW (i.e., being back at work for any duration at time of interview) due to high rates of relapses/failed RTW attempts. [20] Our definition of sustained RTW is based on clinical observations that work disability relapses tend to occur within a month of first RTW [21], and was recommended by the Cochrane review of Coordinator impact on RTW. [16]
Main Exposures The main exposures for this study were the stressfulness of Coordinator interactions and whether the participant had a RTW plan. Both were captured at baseline interview.
Stressfulness of interactions was considered a proxy for Coordinators’ interpersonal activities. Ability to deal with stress has been identified as a “very important” or “essential” Coordinator competency. [17] Participants rated Coordinator interactions on a five-point scale, which ranged from “extremely stressful” to “not at all stressful”. Interactions were categorised as poor if participants rated them as either “quite a bit” or “extremely stressful” and good if rated as “not at all”, “not very”, and “a bit stressful”. Those who reported no contact with a Coordinator served as the reference group.
Having a RTW plan was considered a proxy for Coordinators’ fulfilment of their functional activities. RTW planning involves collecting information about the worker, their injury, their pre-injury job, current work capacity, reasonable accommodations and modifications, consulting with the worker and their health care practitioner, communicating with the worker, and reaching agreement about the plan [13], and is considered an important Coordinator activity [14] and part of best practice for managing work absence and RTW. [10]
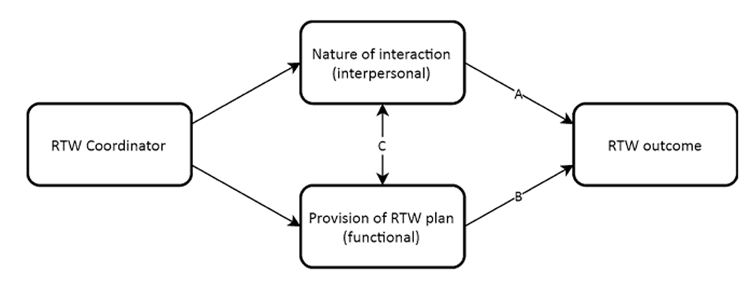
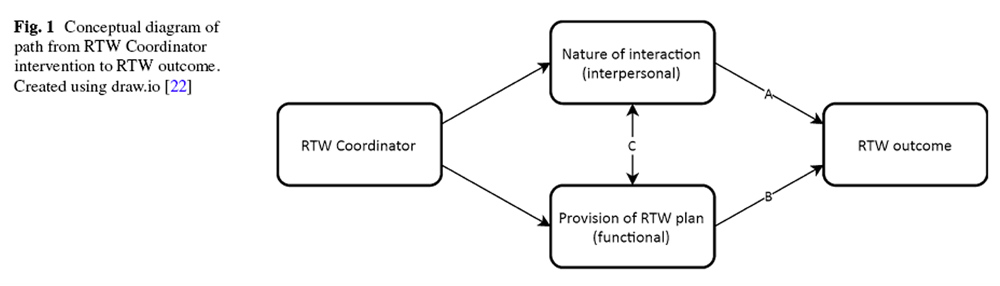
Figure 1 Figure 1 presents a conceptual diagram illustrating these Coordinator activities and their hypothesised impact on RTW outcomes (paths A and B). We anticipated that as measured, the two activities would overlap (path C). For instance, injured workers may be more likely to rate their Coordinator interactions as good if the Coordinator fulfilled their functional role (i.e., provided a RTW plan). Further, Coordinators may be more likely to fulfil their functional activities when the interactions are good. As such, we anticipated unadjusted path A and B would capture effects of both interpersonal and functional activities, while adjustment in multivariable models would isolate direct effects.
Potential Confounders The following were identified as potential confounders of the association between Coordinator activities and RTW outcomes. All were captured at baseline survey. Demographic variables included participant gender and age. Age was categorised into three groups (18–34, 35–54, and 55+) to account for the non-linear relationship observed between age and disability duration among claims with at least 10 days of compensated time loss. [23] Condition type was classified as either a mental health or MSK condition. Workplace factors were assessed using standardised measures. These included supervisor and co-worker response to injury [24, 25], supervisor and co-worker social support, sense of community, and workplace size [26], physical [27] and mental [28, 29] workplace demands, and job autonomy. [30] We also included participant recovery expectations. [24, 25]Analysis
Participant demographics and survey responses were summarised with frequencies or means for each variable, in addition to the proportion of missing values. Attrition analysis was conducted using Pearson’s Chi square on several characteristics (Coordinator interactions, RTW status at baseline, age, gender, and condition type) to determine whether those lost to follow-up differed significantly from those who participated in both surveys.
Associations between Coordinator activities and RTW outcomes were evaluated via logistic regression models for each time point. These included crude (unadjusted) for each activity, separate adjusted for each activity, and adjusted for both activities. Potential confounders were included in adjusted regression models if they had a substantial effect on the association between Coordinator activities and RTW outcomes, which was considered changing main exposure coefficients by at least 10% when added to crude regression models. [31] While this methodology is vulnerable to a high false-positive rate [32], it is considered superior to significance testing in exposure models. [31] Demographic variables and injury type variables were included in adjusted regression models regardless of whether they met the 10% threshold. Missing scale values were imputed with person scale means, provided at least 50% of the participant’s scale items were complete. Person scale means are a reliable method of imputing missing scale values. [33] While the missing threshold is higher than typically used, previous research has found that as long as the total number of missing items and cases is low (>20%), person scale mean imputation can accurately reflect the original data and does not seriously increase scale reliability (i.e., reducing variance and increasing the likelihood of a Type I Error). [34] Further, each non-imputed scale was highly reliable [lowest α = 0.834 (mental demands), complete baseline sample of n = 869], had low missing rates [maximum missing = 14 (2%), analysable sample of n = 632], and was transformed into tertile groups, minimising the impact of bias. Otherwise, cases with missing data were listwise deleted from regression analysis. All independent variables were evaluated for multicollinearity by assessment of Variance Inflation Factor (VIF). Statistical significance was set at p ≤ 0.05. Analyses were conducted in SPSS 23 (IBM Corp., Armonk, New York).
Results
Response Rates
A total of 2,95 claimants were identified as eligible for inclusion in the survey, of whom 321 (13%) opted out. Of the 2,74 for whom contact was attempted, 869 responded to the baseline survey (40%) and 632 (73% of baseline) to follow-up. The most common reason for not participating following contact was refusal (n = 769). Attrition analysis found that baseline participants lost to follow-up were not significantly different in baseline rating of Coordinator interactions, RTW status, gender, or condition type. There were significant differences between age groups, with the youngest (18–34 years) being lost to follow- up at the highest rate (38%, n = 81) and the proportion decreasing with each successive age group: 27% (n = 125) of those aged 35–54 and 17% (n = 31) of those 55+. The majority of those lost to follow-up could not be recontacted (59%; n = 139).
Participant Characteristics

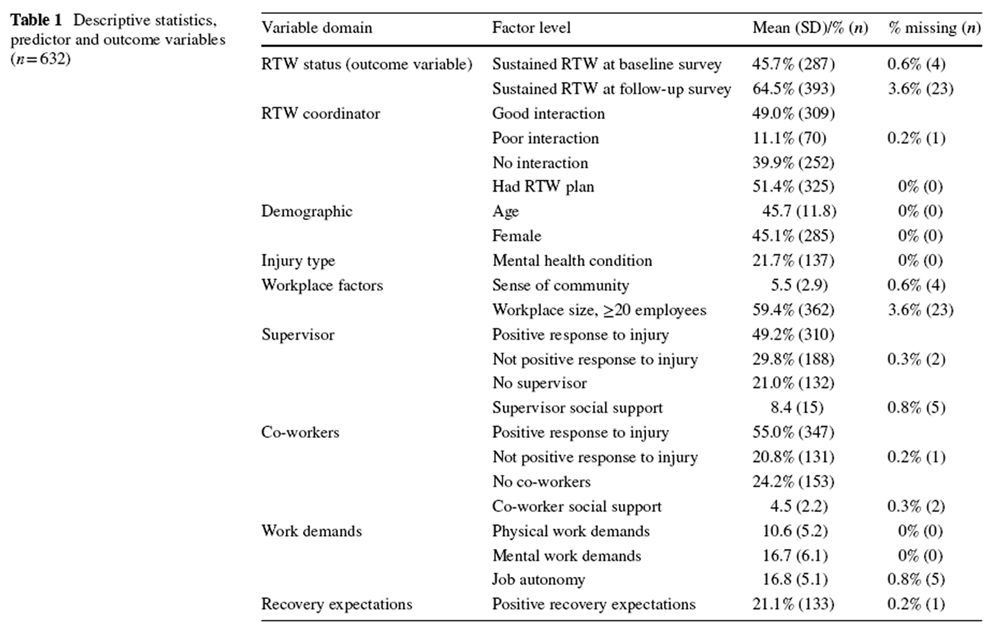
Table 1 Participant characteristics are summarised in Table 1. Average participant age was 46 years. The sample was 45% (n = 285) female. Just over one-fifth were claiming for a mental health condition (22%; n = 137). The median time between injury and baseline interview was four months (inter-quartile range: 3–5 months). Forty-six percent (n = 287) of participants had achieved sustained RTW at baseline and 65% (n = 393) at follow-up. Half the sample rated their Coordinator interactions as good (49%; n = 125), one in ten as poor (11%; n = 70), and 40% (n = 252) had no contact with a Coordinator. The majority of those with no contact reported they did not have a designated Coordinator (28% of sample; n = 168). Half the sample said they had a RTW plan (51%; n = 325).
Associations Between Coordinator Activities and RTW Outcomes
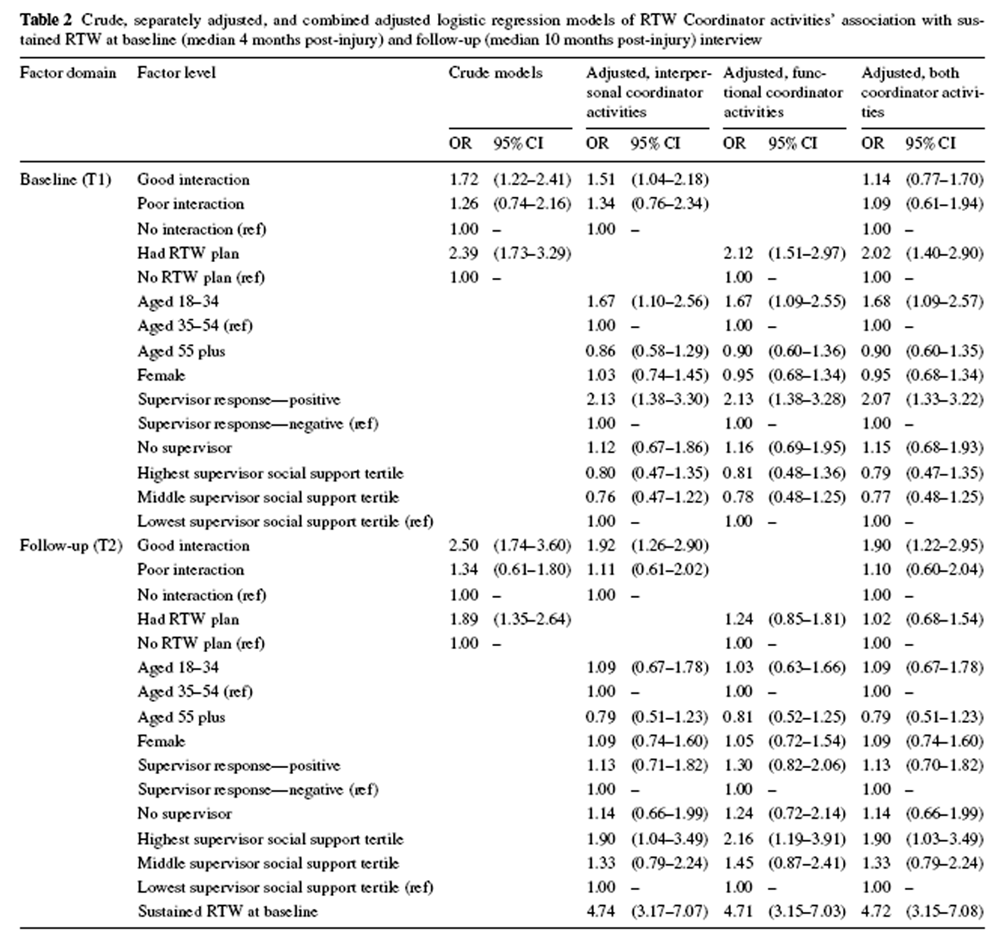
Table 2 Crude and adjusted associations between Coordinator activities and RTW outcomes are presented in Table 2. Variables meeting the threshold for inclusion as a confounder in adjusted analyses were supervisor response to injury and supervisor social support for both baseline and follow-up models, and RTW status at baseline for followup analysis. All VIFs were below 2.5, indicating low risk of multicollinearity.
In crude models, good Coordinator interactions and RTW plans were significantly associated with greater odds of achieving sustained RTW. Most associations remained significant when adjusting for demographics and confounders, the exception being RTW plans at follow-up. Including both Coordinator activities in one regression resulted in only one being significant at either time point: RTW plans were associated with doubled odds of RTW at baseline (OR 2.02, 95% CI 1.40–2.90), while good Coordinator interactions nearly doubled odds of RTW at follow-up (OR 1.90, 95% CI 1.22–2.90). At no point were poor Coordinator interactions significantly associated with RTW outcomes in comparison to no Coordinator interaction.
Discussion
We investigated the impact of workplace-based RTW Coordinators on the RTW outcomes among workers who had taken time off following occupational injury, focusing on two Coordinator activities: having a good interaction with the injured worker and providing a RTW plan. We expected both Coordinator activities to improve RTW outcomes over and above other workplace factors and to observe the association in both cross-sectional and prospective analyses. The findings mostly supported our hypotheses, though there were some surprising results concerning how and when Coordinators affected RTW.
Participant rating of the stressfulness of Coordinator interactions, which we assessed as a proxy for Coordinators’ interpersonal activities, was a major factor in RTW outcomes. When adjusting for demographics and confounders, good interactions were significantly associated with better RTW outcomes, while poor interactions were not significantly different from having no Coordinator contact. However, RTW plans, which we assessed as an indicator of Coordinators’ fulfilment of their functional roles, doubled the odds of RTW at baseline and attenuated the impact of good interactions to non-significance. At follow-up interview, which was administered 6 months after the baseline interview, we found the opposite: good interactions doubled the odds of achieving RTW while RTW plans were not significantly associated with RTW, nor did they substantially attenuate the impact of good interactions.
The findings may be attributable to differences between claimants returning to work at either time point. Earlier in the claims process, injury-related factors such as severity are more important predictors of RTW. [35, 36] Claimants that RTW early tend to do so with little to no intervention. [37] In contrast, psychosocial factors such as psychological job demands, low job control, and work schedule flexibility are more important for those returning later. [35] Such claims are associated with higher rates of secondary mental health conditions, disputes, and resistance to intervention. [37, 38] Henceforth, we refer to these as shorter- and longer-duration claims for simplicity.
Coordinators’ functional role—indicated by the RTW plan—may be the important catalyst for RTW among shorter-duration claims, as suggested by the attenuation of the effect of good interactions when adjusting for RTW plans. The inversion of associations between baseline and follow-up — good interactions were significant while having a RTW plan was not — suggests that Coordinators’ interpersonal activities are more important for fostering RTW among longer-duration claims. As noted above, such claims are vulnerable to secondary mental health conditions and disputes, which better interactions may prevent or mitigate. Longer-duration claims — sometimes referred to as “complex” — are of particular interest to workers’ compensation organisations, since they are estimated to account for 20% of claims yet 90% of liabilities. [37]
In crude analyses, both good interactions and RTW plans were significantly associated with better RTW outcomes at baseline and follow-up interview. When considered with findings of adjusted analyses, this suggests that paths A and B in Fig. 1 capture both the interpersonal and functional Coordinator activities. In other words, the nature of interactions (path A) can reflect Coordinators’ delivery of functional activities, and that functional activities such as drafting a RTW plan (path B) can reflect good interactions.
There are considerable implications for improving Coordinator effectiveness. While previous research has suggested various characteristics of effective Coordinators [6, 11, 14, 17], our results indicate that injured workers are more responsive to different interventions depending on their likely trajectory. For instance, workers likely to RTW earlier in the process may do so more speedily if provided with a RTW plan, while those likely to take more time may benefit from good interactions with their Coordinator. As numerous characteristics are associated with longer-duration claims [39, 40], Coordinator effectiveness and efficiency could be improved through targeted intervention based on injured workers’ likely trajectory, though how this would be done is beyond the scope of this paper. However, as both Coordinator activities were captured at baseline, the findings suggest that regardless of type they should be implemented early in the claims process. Functional activities, as indicated by RTW plans, appeared to have a more immediate effect, while the interpersonal activity was comparatively lagged.
Most participants rated their Coordinator interactions as minimally stressful, though one in six rated them quite or extremely stressful. While the proportion should not be considered generalisable, it hints at what could be a sizeable number of injured workers who could achieve RTW more quickly if they had better interactions with their Coordinator. However, the interactions were rated by the participant, making it difficult to determine why they were deemed stressful. In addition to reflecting how Coordinators treated participants, their ratings could have reflected frustration at failure to achieve RTW, the nature of injury, unmeasured aspects of the workplace or employer, or participant disposition.
Regardless, the only practical means of improving injured workers’ interactions with their Coordinator is through Coordinator selection and training. Some interpersonal traits of successful Coordinators may be inherent and immutable [17] and selecting Coordinators for such attributes, rather than solely on seniority and competence as per current guidelines in Victoria [13], could improve their effectiveness. Revising training, which Coordinators across Australia often feel is irrelevant, with too much focus on legislative requirements and not enough on more practical skills such as counselling [41], may also improve Coordinator effectiveness. [42]
We expected workplace size to confound the association between Coordinator activities and RTW outcomes. There were several reasons for this: Coordinator experience varies based on workplace size: larger organisations (remuneration of $2 million or more in 2013 AUD) must have a Coordinator appointed at all times, while smaller organisations must only appoint them for the duration of the employer’s RTW obligations. [13] This suggests differences in experience. Further, Coordinators from larger organisations in Victoria are more likely to participate in training. [42] However, workplace size did not meet the 10% threshold for impact on associations between main exposures and RTW outcomes at either time point.
One surprising finding was that 40% of participants reported having no contact or interaction with their Coordinator, the majority of whom said they had no designated Coordinator, and half did not have a RTW plan. Employer appointed Coordinators and RTW plans are both are required by WSV. [13] There are several possible reasons for the gaps between Coordinator and RTW plan obligations and provision: employers or Coordinators not meeting their RTW obligations, participants failing to recall their Coordinator interactions or RTW plans, or participants not recognising a co-worker as their Coordinator. Regardless of the reason, improving employer and Coordinator adherence to RTW obligations could have considerable benefits. Evidence on the effectiveness of regulatory workplace inspections [43] suggests that this strategy could be one approach to achieve this.
Strengths and Limitations
A major strength of this study is the use of cross-sectional and longitudinal outcomes, which allowed us to identify shorter- and longer-term impacts of two Coordinator activities on RTW outcomes. Further, while cross-sectional findings were vulnerable to issues of reverse causality (e.g., frustration at failure to achieve sustained RTW causing the participant to view Coordinator interactions negatively), prospective analyses strengthened causal interpretations. Use of sustained RTW outcomes, which required that the injured worker be back at work for at least 1 month by time of interview, mitigated methodological and conceptual issues associated with failed RTW attempts and arbitrary measurement points that plague single point-in-time measures of RTW. Use of two outcome points revealed differences in how and when Coordinators were effective at increasing likelihood of RTW. Had analyses been limited to a single time point, we would have failed to identify at least one of the ways Coordinators can improve RTW outcomes and misattributed effectiveness to a single activity.
Those lost to follow-up were significantly younger than those who were retained in the sample. However, the majority of those lost could not be recontacted and there were no other differences between these groups, suggesting this was the result of greater mobility among younger people. As such, it was unlikely to affect the association between Coordinator interactions and RTW outcomes or to be a serious source of bias.
Limitations included restriction of participants to claimants with upper-body musculoskeletal and mental health conditions, whose disability durations tend to be more variable than other conditions like fracture or disease. [23] Channelling bias, or the assignment to a treatment condition based on prognostic factors [44] (e.g., injury severity and/or employer’s perception of the likelihood of recovery) and a low participation rate may limit the findings’ generalisability and validity. Coordinators in this study were workplace-based, and as such the findings may not apply to Coordinators based at hospitals, insurers, or other locations. The relatively small sample size (n = 632) limited statistical power and may have prevented analyses from identifying other associations, such as the impact of poor Coordinator interactions. Measures of Coordinator intervention were limited to stressfulness of interactions and RTW plans, though there are likely other Coordinator activities that may improve RTW outcomes, such as coordination of RTW across stakeholders and adherences to rules and regulations [14]. The findings do not provide specific details on what makes an interaction good, nor how Coordinators may improve them.
Conclusions
The findings suggest that workplace-based RTW Coordinators are an effective intervention for improving RTW outcomes among injured workers. Their functional activities appeared beneficial for shorter-duration claims, while interpersonal activities appeared beneficial for longer-duration claims. Therefore different Coordinator activities may be more effective depending on injured worker trajectory. However, a large proportion of participants had not been contacted by a Coordinator nor had RTW plans, despite requirements for both.
In many countries, Coordinators help injured workers transition back to the job. Our findings could be used to improve their effectiveness through changes to Coordinator policy and practice, selection and training, and targeted intervention. Future research could further unpack the role to maximise Coordinator impact on RTW outcomes.
Acknowledgments
This research was funded by the Australian Research Council via a Linkage Grant (LP130100091).
Author Contributions
TJL conceived the study, conducted analyses, and drafted the manuscript. PMS, SH-J, RL, ADL, and MRS were responsible for the overall cohort design and data collection. TJL, PMS, SH-G, and MRS
Conflicts of Interest
TJL receives salary support from a WorkSafe Victoria grant. WorkSafe Victoria regulates workers’ compensation policies affecting the participants in this study. PMS, RL, SH-J, ADL, and MRS declare they have no conflict of interest.
References:
International Labour Organization.
Safety and health at work: a vision for sustainable prevention:
XX world congress on safety and health at work 2014:
global forum for prevention, 24–27 August 2014, Frankfurt, Germany.
Geneva: International Labour Office; 2014.
http://www.ilo.org/wcmsp5/groups/public/---ed_protect/---protrav/
---safework/documents/publication/wcms_301214.pdf.Waddell G, Burton AK.
Is work good for your health and wellbeing? London:
Department for Work and Pensions; 2006.McKee-Ryan FM, Song Z, Wanberg CR, Kinicki AJ.
Psychological and physical well-being during unemployment: a metaanalytic study.
J Appl Psychol. 2005;90(1):53–76.Broom DH, D’Souza RM, Strazdins L, Butterworth P, Parslow R.
The lesser evil: bad jobs or unemployment? A survey of mid-aged Australians.
Soc Sci Med. 2006;63(3):575–586.Milner A, Krnjacki L, Butterworth P, Kavanagh A, LaMontagne AD.
Does disability status modify the association between psychosocial job quality and mental health? A longitudinal fixedeffects analysis.
Soc Sci Med. 2015;144:104–111Gardner BT, Pransky G, Shaw WS, Hong QN, Loisel P.
Researcher perspectives on competencies of return-to-work coordinators.
Disabil Rehabil. 2010;32(1):72–78.Shaw WS, Hong QN, Pransky G, Loisel P.
A literature review describing the role of return-to-work coordinators in trial programs and interventions designed to prevent workplace disability.
J Occup Rehabil. 2008;18(1):2–15.Franche RL, Cullen K, Clarke J, Irvin E, Sinclair S, Frank J, et al.
Workplace-based return-to-work interventions: a systematic review of the quantitative literature.
J Occup Rehabil. 2005;15(4):607–631.Tompa E, de Oliveira C, Dolinschi R, Irvin E.
A systematic review of disability management interventions with economic evaluations.
J Occup Rehabil. 2008;18(1):16–26.Durand MJ, Corbiere M, Coutu MF, Reinharz D, Albert V.
A review of best work-absence management and return-towork practices for workers with musculoskeletal or common mental disorders.
Work. 2014;48(4):579–589Bohatko-Naismith J, James C, Guest M, Rivett DA.
The role of the Australian workplace return to work cordinator: essential qualities and attributes.
J Occup Rehabil. 2015;25(1):65–73.Bohatko-Naismith J, Rivett DA, James C, Guest M.
A review of the role and training of return to work coordinators in Australia.
J Health Saf Environ. 2012;28(2):173–190.WorkSafe Victoria.
Return to work coordination: the basics you need to know.
In: Victorian WorkCover Authority, editor.
Melbourne: WorkSafe Victoria; 2013.Durand MJ, Iuliana N, Coutu MF, Bernier M.
Practices of return-to-work coordinators working in large organizations.
J Occup Rehabil. 2017;27(1):137–147.Tan HSK, Yeo DSC, Giam JYT, Cheong FWF, Chan KF.
A randomized controlled trial of a return-to-work coordinator model of care in a general hospital to facilitate return to work of injured workers.
Work. 2016;54(1):209–222.Vogel N, Schandelmaier S, Zumbrunn T, Ebrahim S, de Boer WEL et al.
Return-to-work coordination programmes for improving return to work in workers on sick leave.
Cochrane Database Syst Rev. 2017Pransky G, Shaw WS, Loisel P, Hong QN.
Development and validation of competencies for return to work coordinators.
J Occup Rehabil. 2010;20(1):41–48.WorkSafe Victoria.
VCode: the nature of injury/disease classification system for Victoria.
Melbourne: WorkSafe Victoria; 2008.
https://www.worksafe.vic.gov.au/__data/assets/pdf_file/0010/10513/
VCode_Vs1.2_1_July_2008_26_June_08.pdfAustralian Safety and Compensation Council.
Type of occurrence classification system 3rd edition revision 1.
Canberra: Australian Government; 2008.
https://www.safeworkaustralia.gov.au/system/files/documents/1702/
type_of_occurrence_classification_system_3rd_edition_revision_1.pdfBerecki-Gisolf J, Clay FJ, Collie A, McClure RJ.
Predictors of sustained Return to Work after work-related injury or disease: insights from workers’ compensation claims.
J Occup Rehabil. 2012;22(3):283–291.Steenstra IA, Lee H, de Vroome EMM, Busse JW, Hogg-Johnson S.
Comparing current definitions of return to work: a measurement approach.
J Occup Rehabil. 2012;22(3):394–400.JGraph Ltd. draw.io.
London, UK; 2017.
https://www.draw.io/Lane TJ, Collie A, Hassani-Mahmooei B.
Work-related injury and illness in Australia, 2004 to 2014:
what is the incidence of work-related conditions and their impact on time loss
from work by state and territory, age, gender and injury type?
Melbourne: Monash University (ISCRR); 2016. Contract No.: 118-0616-R02.
http://www.iscrr.com.au/__data/assets/pdf_file/0020/540830/
118_Work-injury-in-Australia-Review-2004-2014.pdfHogg-Johnson S, Cole DC.
Early prognostic factors for duration on temporary total benefits in the first year among workers with compensated occupational soft tissue injuries.
Occup Environ Med. 2003;60(4):244–253.Cole DC, Mondloch MV, Hogg-Johnson S.
Listening to injured workers: how recovery expectations predict outcomes.
Can Med Assoc J. 2002;166(6):749–754.Kristensen TS, Hannerz H, Hřgh A, Borg V.
The Copenhagen psychosocial questionnaire: a tool for the assessment and improvement of the psychosocial work environment.
Scand J Work Env Hea. 2005;31(6):438–449.Franche RL, Corbičre M, Lee H, Breslin FC, Hepburn CG.
The Readiness for return-to-work (RRTW) scale: development and validation of a self-report staging scale in lost-time claimants with musculoskeletal disorders.
J Occup Rehabil. 2007;17(3):450–472Cousins R, MacKay CJ, Clarke SD, Kelly C, Kelly PJ, McCaig RH.
‘Management Standards’ work-related stress in the UK: practical development.
Work Stress. 2004;18(2):113–136.MacKay CJ, Cousins R, Kelly PJ, Lee S, McCaig RH.
‘Management Standards’ and work-related stress in the UK: policy background and science.
Work Stress. 2004;18(2):91–112.Breaugh JA.
The measurement of work autonomy.
Hum Relat. 1985;38(6):551–570.Rothman KJ.
Epidemiology: an introduction, 2nd ed.
New York: Oxford University Press; 2012.Bliss R, Weinberg J, Webster T, Vieira V.
Determining the probability distribution and evaluating sensitivity and false positive rate of a confounder detection method applied to logistic regression.
J Biom Biostat. 2012;3(4):142Shrive FM, Stuart H, Quan H, Ghali WA.
Dealing with missing data in a multi-question depression scale: a comparison of imputation methods.
BMC Med Res Methodol. 2006;6(1):57Downey RG, King CV.
Missing data in likert ratings: a comparison of replacement methods.
J Gen Psychol. 1998;125(2):175–191.Krause N, Dasinger LK, Deegan LJ, Rudolph L, Brand RJ.
Psychosocial job factors and return-to-work after compensated low back injury: a disability phase-specific analysis.
Am J Ind Med. 2001;40(4):374–392.Dasinger LK, Krause N, Deegan LJ, Brand RJ, Rudolph L.
Physical workplace factors and return to work after compensated low back injury:
a disability phase-specific analysis.
J Occup Environ Med. 2000;42(3):323–333.Glass D.
Investigation into the management of complex workers compensation claims and
WorkSafe oversight.
Melbourne: Victorian Ombudsman; 2016. Contract No.: 203.Schultz IZ, Gatchel RJ, editors.
Handbook of complex occupational disability claims: early risk identification, intervention, and prevention.
New York: Springer; 2005.Street TD, Lacey SJ.
A systematic review of studies identifying predictors of poor return to work outcomes following workplace injury.
Work. 2015;51(2):373–381.Steenstra IA, Busse JW, Tolusso D, Davilmar A, Lee H, Furlan AD, et al.
Predicting time on prolonged benefits for injured workers with acute back pain.
J Occup Rehabil. 2015;25(2):267–278.Bohatko-Naismith J, Guest M, Rivett DA, James C.
Insights into workplace return to work coordinator training: an Australian perspective.
Work. 2016;55(1):29–36.Cooney R, Mwila NK.
Improving return to work (RTW) Coordinator training. Melbourne: Institute for Safety,
Compensation and Recovery Research,
Monash University; 2013. Contract No.:1212-033-R2C.Levine DI, Toffel MW, Johnson MS.
Randomized government safety inspections reduce worker injuries with no detectable job loss.
Science. 2012;336(6083):907–911.Lobo FS, Wagner S, Gross CR, Schommer JC.
Addressing the issue of channeling bias in observational studies with propensity scores analysis.
Res Social Adm Pharm. 2006;2(1):143–151.
Return to LOW BACK PAIN
Return to RETURN TO WORK
Return to WORKERS' COMPENSATION
Since 6-28-2018
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |