

Algorithms for the Chiropractic Management of
Acute and Chronic Spine-Related PainThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Topics in Integrative Health Care 2012 (Dec 31); 3 (4) ~ FULL TEXT
OPEN ACCESS Gregory A. Baker, DC, Ronald J. Farabaugh, DC, Thomas J. Augat, DC, MS, CCSP, FASA,
Cheryl Hawk, DC, PhD, CHES
You may also enjoy this Algorithm PowerPoint
Algorithm PowerPoint (PPT format)
Algorithm PowerPoint (PPTX format)The complexity of clinical documentation and case management for health care providers has increased along with the rise of managed care. Keeping up with the policies of different insurers and third party administrators can be a daunting task. To address these issues for doctors of chiropractic (DCs) and policymakers, the Council for Chiropractic Guidelines and Practice Parameters (CCGPP) developed three consensus documents. Each of these documents was the outcome of a formal consensus process in which a multidisciplinary Delphi panel consisting of experts in chiropractic and low back pain treatment came to agreement on terminology and treatment parameters for the chiropractic management of spine-related musculoskeletal pain. [1-3]
From the FULL TEXT Article
Introduction:
The complexity of clinical documentation and case management for health care providers has increased along with the rise of managed care. Keeping up with the policies of different insurers and third party administrators can be a daunting task. To address these issues for doctors of chiropractic (DCs) and policymakers, the Council for Chiropractic Guidelines and Practice Parameters (CCGPP) developed three consensus documents. Each of these documents was the outcome of a formal consensus process in which a multidisciplinary Delphi panel consisting of experts in chiropractic and low back pain treatment came to agreement on terminology and treatment parameters for the chiropractic management of spine-related musculoskeletal pain. [1–3] Their recommendations were based on a combination of consideration of the current evidence and their clinical judgment. In addition, another consensus document related to care rendered by doctors of chiropractic for the purpose of health promotion, disease prevention, and wellness, developed through a project funded by the NCMIC Foundation, was also referenced to clarify terminology used in the algorithms. [4] (See Table 1.)
Table 1. Definition of terms related to acute and chronic care
The terms "supportive care" and "maintenance care," which are frequently used within the chiropractic health care arena, are not consistent with general healthcare industry lexicon. Instead of “supportive care,” we use the more descriptive term, “ongoing/recurrent” care.
Chronic pain management can be divided into three categories:
those who can home manage;
those who can be managed with episodic care; and
those who need “scheduled” ongoing care, which is a very small proportion of chronic pain sufferers. Those patients require proper documentation of responses to care and procedures, including therapeutic withdrawal response, multi-modal, multi-disciplinary consideration, patient education, etc.
Other related consensus-based terms: [1, 2]
Medically necessary care of acute conditions:
“care that is reasonable and necessary for the diagnosis and treatment of a patient with a health concern and for which there is a therapeutic care plan and a goal of functional improvement and/or pain relief.” [1,p.461]Medically necessary care for recurrent/chronic conditions:
“care that is provided when the injury/illness is not expected to completely resolve after a treatment regimen but where continued care can reasonably be expected to result in documentable improvement for the patient.” [1,p.461]Chiropractic management of chronic/recurrent conditions:
“Chiropractic care provided for the purpose of preventing relapse and/or exacerbations of the original complaint(s) as well as associated comorbidities.” [2, p. 560]Chiropractic wellness care or preventive care:
“Chiropractic care provided for the purpose of preventing disease, optimizing function, and supporting the patient's wellness-related activities.” [2, p. 560]
Dehen MD, Whalen WM, Farabaugh RJ, Hawk C.
Consensus Terminology for Stages of Care: Acute, Chronic, Recurrent, and Wellness
J Manipulative Physiol Ther 2010 (Jul); 33 (6): 458–463Hawk C, Schneider M, Evans MW, Jr., Redwood D.
Consensus Process to Develop a Best-Practice Document on the Role of Chiropractic Care in Health Promotion, Disease Prevention, and Wellness
J Manipulative Physiol Ther 2012 (Sep): 35 (7): 556–567
In order to make the recommendations in these three documents more accessible to users, the CCGPP created a set of algorithms based on these consensus recommendations. Clinical algorithms essentially provide a map to guide the practitioner in case management, especially for complex and multifactorial conditions. Using evidence-based clinical algorithms supports effective standardized care. [5] To ensure that the algorithms accurately represented the consensus recommendations, they were reviewed by a group of experts and then revised as per the experts’ comments. Experts invited to review were1) 2 members of CCGPP’s Research Panel;
2) 5 members of the CCGPP board representing districts of the Congress of Chiropractic State Associations (COCSA);
3) all 59 Delphi panelists who participated in the consensus projects on acute and chronic spine-related pain.
There were a total of 66 invited; 3 Delphi panelists did not have valid e-mail addresses, reducing the total to 63. Of these, responses were provided by1) 2 of 2 Research Panel members;
2) 3 of 5 COCSA representatives; and
3) 20/56 Delphi panelists, for an overall response rate of 38%.
These algorithms are only a guide, and are not appropriate for all patients and conditions. In particular, it should be noted that they relate specifically to spine-related pain, so are not applicable to other chiropractic treatment objectives. Furthermore, these algorithms are designed to guide the DC in planning the stages of care. They do not dictate the type of treatment procedures provided. These are detailed elsewhere. [3]
In general, these may include the following, as per the clinician’s assessment of patient needs:Active care procedures, such as rehabilitation/therapeutic exercises
counseling on activities of daily living, home exercise, pain management, other aspects of self-management and other lifestyle factors
passive care, such as manual therapy including joint adjustment/manipulation, joint mobilization, and soft tissue techniques
physical modalities
acupuncture
bracing, taping and orthoses, and
nutritional and nutriceutical support.These algorithms are designed to assist in the management of spine-related pain. They were designed for the chiropractic profession, but other provider types may also find them useful, since the algorithms do not specifically address the components of the treatment visit.
The algorithms are not designed for the management of other clinical objectives, such as non-painful functional or structural spinal care. They are also not appropriate for wellness care or other types of prevention and/or health promotion. If the algorithm suggests the release or referral of a patient, then the patient has either recovered or the clinical objective is outside the scope of this algorithm. See Figures 1–3 for the algorithms. For detailed information on the consensus projects from which these algorithms were derived, the reader is referred to the original papers. [1–3]
Figure 1. Algorithm for the Chiropractic Treatment of Spine Related Pain
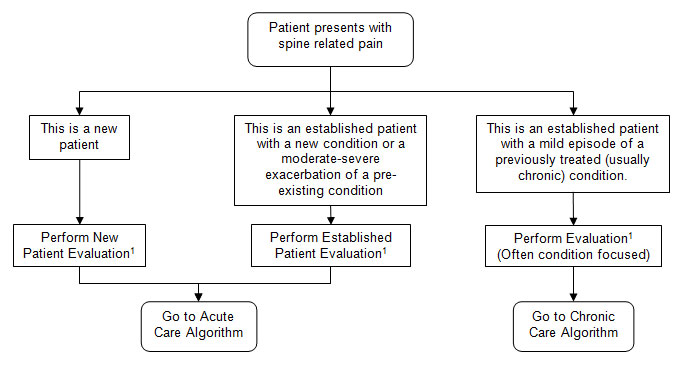
1 Evaluation components
- History
- Examination
- Outcomes Assessment Tools
- Pain intensity scales
- Pain diagrams
- Pain and disability questionnaires
- Functional outcomes questionnaires
- General health questionnaires
- Psychological profiles
- Imaging if warranted
Figure 2. Acute Care Algorithm
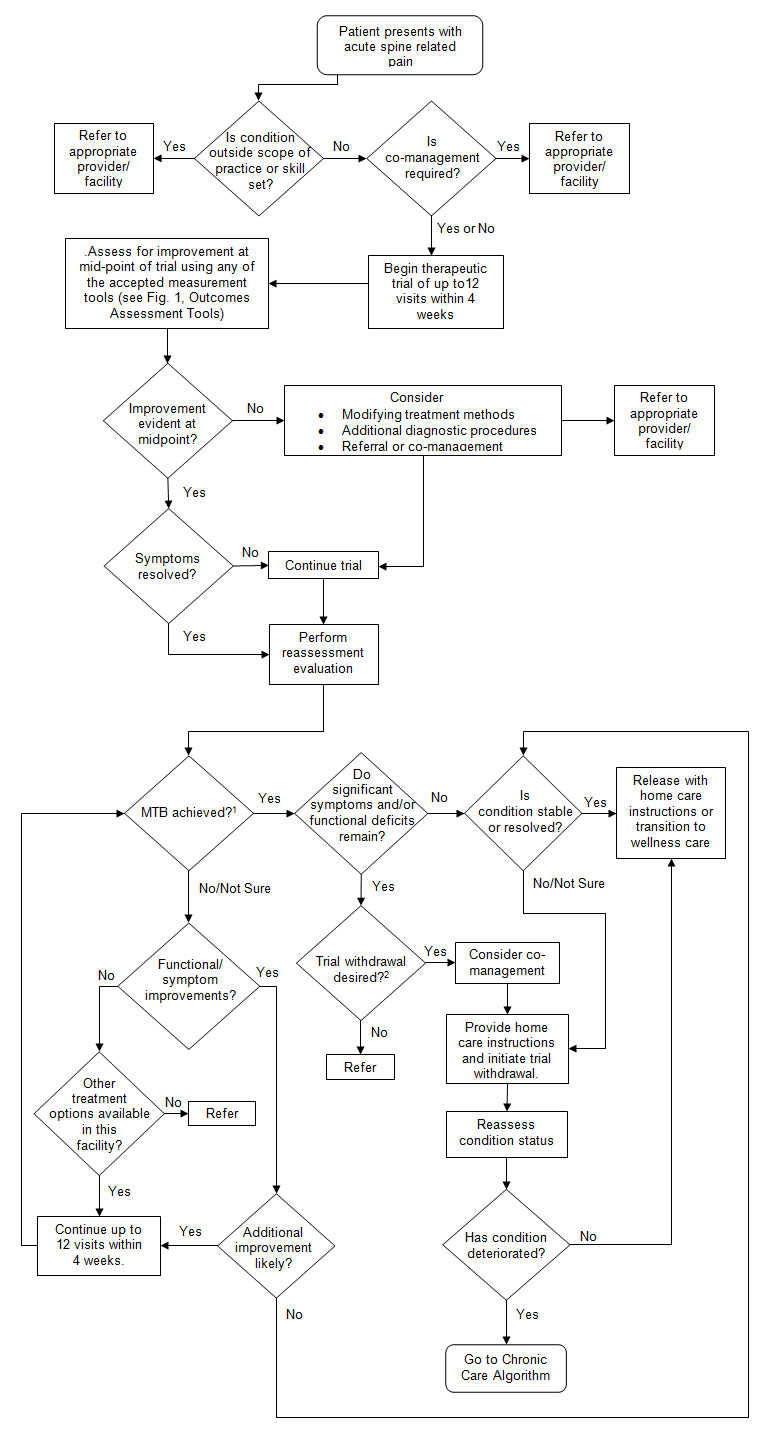
1 MTB = maximum therapeutic benefit
2 Trial withdrawal
A trial withdrawal may be necessary once a patient reaches maximum therapeutic improvement. This helps to determine if the condition recovery is stable. If the condition has deteriorated after the trial, then chronic or ongoing care may be necessary to maintain function and minimize symptoms. The therapeutic withdrawal can be gradual, where the patient’s care is tapered off. It can also be abrupt, with the patient instructed to return if the symptoms recur; or the patient can be scheduled for an evaluation at a later date to determine if there is any regression.
Figure 3. Chronic Care Algorithm
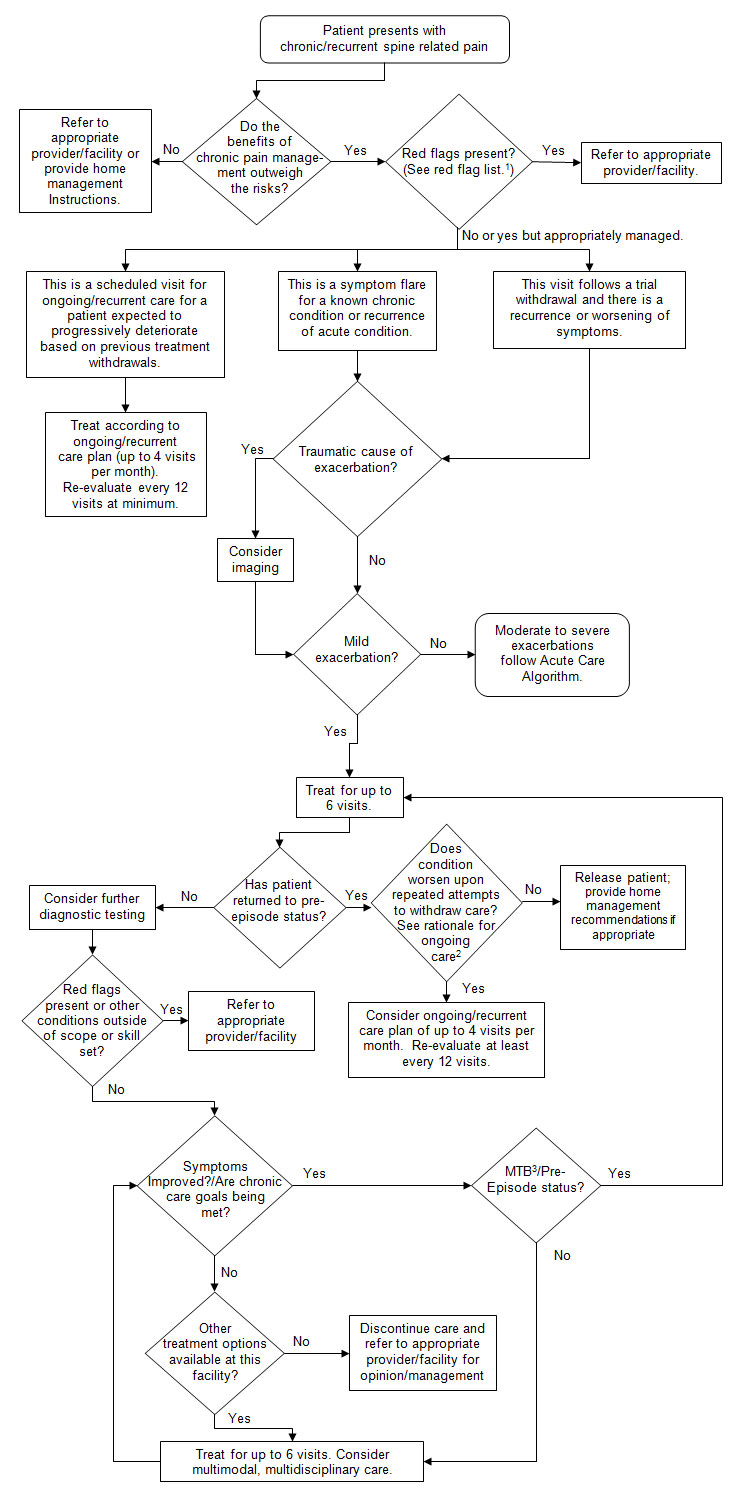
1 Red Flags
- Progressive neurological disorders
- Cauda equina syndrome
- Bone weakening disorders; i.e.; acute spinal fracture, spinal infection, spinal or extra-vertebral bony malignancies
- Tumor
- Articular derangements indicating instability; i.e., active avascular necrosis in weight-bearing joints
2 Documentation of necessity of ongoing care (in addition to standard documentation):*Complicating factors*
- Clinically meaningful response to initial treatment
- Maximum therapeutic benefit (MTB)
- Significant residual activity limitations
- Attempts to transition to self-care
- Consideration of alternative treatment approaches
- Factors affecting likelihood that self-care alone will sustain MTI (see Complicating Factors, below)
Patient characteristics Injury characteristics History Older age Severe initial injury >Pre-existing pathology Psychosocial factors > 3 previous episodes or surgery Delay treatment >7 days Severe signs and symptoms History of lost time Non-compliance Number/severity previous History of prior treatment Lifestyle habits exacerbations Congenital anomalies Obesity** Treatment withdrawal fails Symptoms persist despite Type of work activities to sustain MTI previous treatment* This list is not all-inclusive.
Source: Farabaugh RJ, Dehen MD, Hawk C.
Management of Chronic Spine-Related Conditions: Consensus Recommendations of a Multidisciplinary Panel
J Manipulative Physiol Ther 2010 (Sep); 33 (7): 484–492
**Source: Harvard Health Letter.
Drop pounds to relieve back pain. Strengthening your core muscles can also help.
Harv Health Lett 2012; 37 (10): 4–6
MTB = maximum therapeutic benefit
Acknowledgements:
The authors thank the experts who generously donated their time and expertise to reviewing the algorithms: Richard Branson, DC; Wayne Carr, DC; Frederick Carrick, DC, PhD; Jeffrey Cates, DC, MS, DABCO; Gregory Doerr, DC, CCSP, ART, CSTI, CKTP; John Downes, DC; Joseph Ferstl, DC, FACO; Anthony Hall, DC; Michael Hall, DC, FIACN; Kathryn Hoiriis, DC; Cole Hosenfeld, DC, CCSP; Lawrence Humberstone, DC; Thomas Kosloff, DC; Kurt Kuhn, DC, PhD, MS; Glen Nykwest, DC; Mariangela Penna, DC; Reed Phillips, DC, PhD; Daniel Redwood, DC; Gregory Snow, DC; John Stites, DC, DACBR; Leonard Suiter, DC; David Taylor, DC, DABCN, FIACN.
They also thank Michelle Anderson for coordinating all electronic communications for the project.
References:
Globe GA, Morris CE, Whalen WM, et al.
Chiropractic Management of Low Back Disorders: Report From a Consensus Process
J Manipulative Physiol Ther 2008 (Nov); 31 (9): 651–658Dehen MD, Whalen WM, Farabaugh RJ, Hawk C.
Consensus Terminology for Stages of Care: Acute, Chronic, Recurrent, and Wellness
J Manipulative Physiol Ther 2010 (Jul); 33 (6): 458–463
Farabaugh RJ, Dehen MD, Hawk C.
Management of Chronic Spine-Related Conditions:
Consensus Recommendations of a Multidisciplinary Panel
J Manipulative Physiol Therp 2010 (Sep); 33 (7): 484–492
Hawk C, Schneider M, Evans MW, Jr., Redwood D.
Consensus Process to Develop a Best-Practice Document on the Role of Chiropractic Care
in Health Promotion, Disease Prevention, and Wellness
J Manipulative Physiol Ther 2012 (Sep): 35 (7): 556–567
Miller T, Ryan M, York C.
Utlizing algorithms and pathways of care in allied health practice.
Internet J Allied Health Sciences Practice 2005; 3 (2)
Harvard Health Letter.
Drop pounds to relieve back pain. Strengthening your core muscles can also help.
Harv Health Lett 2012; 37 (10): 4
Return to BEST PRACTICES
Return to LOW BACK PAIN
Return to CHRONIC NECK PAIN
Return to LOW BACK GUIDELINES
Return to DIAGNOSIS AND MANAGEMENT
Since 3–25–2013
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |