

An Evidence-based Diagnostic
Classification System For Low Back PainThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Canadian Chiropractic Assoc 2013 (Sep); 57 (3): 189–204 ~ FULL TEXT
OPEN ACCESS Robert Vining, DC, Eric Potocki, DC, MS, Michael Seidman, MSW, DC,
A. Paige Morgenthal, DC, MS
Palmer College of Chiropractic,
Palmer Center for Chiropractic Research,
5433 Bryant Ave,
South Minneapolis, MS 55419;
dr.potocki@yahoo.com
INTRODUCTION: While clinicians generally accept that musculoskeletal low back pain (LBP) can arise from specific tissues, it remains difficult to confirm specific sources.
METHODS: Based on evidence supported by diagnostic utility studies, doctors of chiropractic functioning as members of a research clinic created a diagnostic classification system, corresponding exam and checklist based on strength of evidence, and in-office efficiency.
RESULTS: THE DIAGNOSTIC CLASSIFICATION SYSTEM CONTAINS ONE SCREENING CATEGORY, TWO PAIN CATEGORIES: Nociceptive, Neuropathic, one functional evaluation category, and one category for unknown or poorly defined diagnoses. Nociceptive and neuropathic pain categories are each divided into 4 subcategories.
CONCLUSION: This article describes and discusses the strength of evidence surrounding diagnostic categories for an in-office, clinical exam and checklist tool for LBP diagnosis. The use of a standardized tool for diagnosing low back pain in clinical and research settings is encouraged.
From the FULL TEXT Article:
Introduction
Health professionals across such disciplines as orthopedics, physical therapy, and chiropractic have shared the goal of categorizing patients with musculoskeletal low back pain (LBP) according to evidence-based classification systems. [1, 2] To this end, several investigators have generated classification systems for LBP diagnosis and treatment. [3–8] Identifying specific pathophysiology causing LBP has the potential to positively impact clinical research and practice by providing opportunities to test, validate or reject treatments targeted at specific diagnoses. [1, 2] Clinical prediction rules [4, 6] and symptom or treatment-based classification systems [7, 8] lack the pathophysiological component(s) clinicians sometimes use to better understand a condition and make clinical decisions. Patho-anatomic diagnoses address pain arising from more specific anatomic structures or pathological processes. However, definitively confirming pain sources for LBP continues to be a challenge.
Clinical guidelines recommend evidence-based assessment and suggest classifying LBP patients with substantial neurological involvement, inflammatory arthritis, visceral or metastatic disease, and non-specific pain. [9, 10] Rather than using the label of non-specific pain, an evidence-based diagnostic tool can potentially help identify conditions with similar characteristics, and aid communication with other clinicians, third-party payers, and patients by providing consistent terminology and assessment methods.
It is still largely unknown whether treatment according to various classification systems results in improved clinical outcomes. More research is needed to definitively answer this question. [1, 2, 11, 12] The purpose of this methodological project was to create a diagnostic classification system with an evidence-based diagnostic checklist tool for use in a chiropractic research clinic conducting clinical trials of LBP [13–15] and for use in traditional clinical settings.
Eligibility and treatment decisions for clinical studies of LBP at our research center are in part based on diagnostic information. The authors recognized a need for both a standardized clinical evaluation and diagnostic criteria to facilitate more consistent use of evidence-based diagnostic rationale.
Our goals for this project were to:(1) identify diagnostic LBP categories supported by the best available evidence, and
(2) create an efficient in-office evidence-based LBP diagnostic checklist and accompanying exam
for use in research and clinical practice.This article outlines the diagnostic categories, accompanying checklist, and discusses the supporting evidence.
Methods
Recognizing the need for more specific diagnostic information, the authors sought to create a LBP diagnostic classification system based on available evidence for use in both a research and clinical setting. One system was available for use as a model. Therefore, the process began with a diagnostic classification system published by Petersen. [3, 16] This classification system was chosen because it encapsulated diagnosis from a patho-anatomic/pathophysiological perspective and it represented the potential to categorize LBP patients in a research setting.
Briefly, these diagnostic categories included:(1) disc syndromes,
(2) adherent nerve root,
(3) nerve root entrapment,
(4) nerve root compression,
(5) spinal stenosis,
(6) zygapophyseal joint,
(7) postural,
(8) sacroiliac joint,
(9) dysfunction,
(10) myofascial pain,
(11) adverse neural tension,
(12) abnormal pain, and
(13) inconclusive.Next, references from Petersen’s classification system were reviewed and PubMed searches conducted to identify additional articles supporting each diagnostic category using key words describing the diagnostic category (e.g., facet, zygapophyseal joint, sacroiliac, SI joint, etc.), low back pain, utility, test, diagnosis, diagnostic, and manual therapy. Systematic reviews and clinical guidelines regarding low back pain diagnosis were also reviewed for conclusions, recommendations and as reference sources. Reference searches of diagnostic utility studies were also conducted.
Systematic reviews, clinical guidelines, and publications with higher diagnostic utility values, reference standards for higher quality research were sought and utilized to create the classification system.
Criteria utilized for consideration were:(1) commonly accepted diagnoses for which there is general agreement
regarding pathophysiology
(2) tests performed in an office setting, and
(3) articles reporting consistent with evidence-based criteria, such as
reporting sample population characteristics, appropriate
statistical analysis, use of a gold standard comparison,
validation studies performed, and sensitivity/
specificity reporting. [17]Nine doctors of chiropractic including the authors, functioning as members of the research clinic, utilized the initial diagnostic classification system and checklist for a period of one year while formally reviewing examinations of 166 participants with LBP who presented to the clinical research team during an IRB approved clinical trial. Formal meetings were held to discuss and inform clinicians about the classification system prior to its use. Clinicians using the checklist provided verbal and written feedback to the authors regarding clarity of terms, strength of evidence, efficiency, and usefulness as an in-office aid throughout the one-year trial period.
The categories contained in the original classification system were:(1) Screening,
(2) Reducible disc,
(3) Irreducible disc,
(4) Discogenic pain,
(5) Nerve root,
(6) Neurogenic claudication,
(7) SI joint,
(8) Zygapophyseal joint,
(9) Dysfunction/Postural instability,
(10) Myofascial,
(11) Non-organic,
(12) Chronic pain syndrome, and
(13) Other diagnoses.Factors observed by clinicians leading to changes included:
(1) criteria for some categories were largely similar,
(2) the large number of categories created a lengthy exam,
(3) the neurogenic claudication category required a checklist item(s)
to help rule-out similarly presenting conditions, such as vascular claudication,
(4) a single category entitled central pain better represented the
chronic pain syndrome and non-organic pain categories, and
(5) separating nociceptive and neuropathic pain diagnoses into subcategories
is more aligned with clinical assessment.The revised classification system was reorganized into 4 main diagnostic categories. Criteria with positive likelihood ratios lower than 2.4 were removed except for the myofascial category. The classification system and checklist presented in this article is currently in use at our research center (Appendix A).
Results
Four diagnostic categories and 8 subcategories in the classification system include:(1) a screening category,
(2) two pain categories with subcategories for Nociceptive and Neuropathic Pain,
(3) a functional evaluation category, Functional Instability, and
(4) a category for unknown or poorly defined diagnoses.Table 1. Low Back Pain Diagnostic Categories and Key Information.
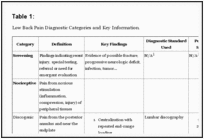
The clinical evaluation is characterized by a diagnostic category checklist comprised of yes/no questions and corresponding tests. Questions in each category of the checklist relate to symptoms, signs, and examination findings. Questions answered “Yes” indicate support for a diagnostic category. However, some questions indicate support for a category when answered “No”. “No” answers indicating support for a diagnosis are highlighted to provide a visual cue to the clinician. Most information needed to answer checklist questions are derived from the condition history and patient interview. However, several categories such as Zygapophyseal joint and SI joint include questions requiring specific exam information. Examination procedures included within the diagnostic checklist are also separately provided in Appendix B.
Several items in the diagnostic checklist are supported by Likelihood ratios, which describe the probability that a test accurately detects a disease. A positive likelihood ratio (+LR) of 1 lacks diagnostic value. [18] Higher values increase the diagnostic value. Positive LRs of 2–5 are considered small but sometimes important. Positive LRs of 5–10 are considered moderate but usually important while those over 10 are large and often conclusive. [19]
Diagnostic Categories
Screening
This category includes screening questions for acute injury, infection, potentially dangerous conditions such as cauda equina syndrome, or conditions requiring referral to an appropriate healthcare specialty. Criteria were drawn from evidence-based clinical guidelines and LBP screening recommendations. [9, 10, 20, 21] The screening category was not designed as a comprehensive screen for any condition requiring additional evaluation. It is, therefore, imperative that providers utilizing this tool recognize it as a supplement rather than a replacement for careful interpretation of clinical information.
Nociceptive Pain
Nociceptive pain is perceived from noxious stimulation (e.g. inflammation, compression, injury) of peripheral tissues causing primary afferent neuron signaling. [22] One recent study found more than 50% of LBP patients could be classified with nociceptive pain based on clinical criteria developed by an expert panel of clinicians. [23]
Nociceptive pain from the low back is divided into the following 4 subcategories:(1) lumbar discogenic pain,
(2) sacroiliac joint pain,
(3) zygapophyseal joint pain, and
(4) myofascial pain.Discogenic Pain
Lumbar discogenic pain is thought to be generated from nociceptive signaling of nerve fibers infiltrating the posterior annular fibers of an intervertebral disc and near its attachment at the endplate. [24] Infiltration appears to occur most in discs that exhibit some degree of annular disruption. [25, 26] Discogenic pain, studied with the use of discography, has been shown to reproduce LBP symptoms in patients with annular disruption. [27] However, discography findings can be interpreted differently and procedural variations that can affect results. [28] A comprehensive review of diagnostic interventions for chronic spinal pain rated lumbar discography with evidence level II-2, or evidence obtained from at least one properly designed small diagnostic accuracy study. [29]
Studies utilizing discography for diagnostic confirmation show centralization of pain with repeated motion as a key diagnostic phenomenon. [30, 31] Centralization is defined as progressive resolution, reduction or retreat of pain toward midline. Patients diagnosed with discogenic pain, particularly those whose symptoms centralize with repeated motion, tend to show a favorable response to conservative treatment. [32–34] A recent review of clinical tests rated centralization with repeated motion as diagnostic for discogenic pain [35] and a recent practice-based study found centralization signs in 41% of LBP cases. [36]
Sacroiliac (SI) Joint Pain
025The SI joints are irregularly shaped, diarthrodial joints supported by strong ligaments. [37] Lumbar paraspinal and pelvic muscles are considered significant stabilizers and other muscles as remote as the latissimus dorsi may also contribute via attachments through the thoracolumbar fascia. [38] SI joint innervation arises from the sacral plexus, ventral rami from L4 and L5 and dorsal sacral rami. [37] Two studies using an anesthetic block procedure reported 18.5% and 30% of LBP patients experienced SI joint pain. [39, 40] Another study using the same examination criteria found in the checklist diagnosed 27% of patients with SI joint pain. [36]
SI joint symptom presentation is similar to that from other low back sources and there is evidence to suggest that the SI joint may be responsible for some cases of sciatica in the absence of disc or nerve root pathology. [41] One study using controlled diagnostic SI joint blocks reports SI joint pain occurred in the area just inferior to the posterior superior iliac spine and rarely presented in the area over the ischial tuberosity. [42] However, further validation of these results is needed. One recent systematic review considered controlled SI joint injections, the current diagnostic standard, to be supported by a moderate level of evidence [43] and another rated it as level II-2 evidence derived from well-designed cohort or case-control analytic studies. [44]
The SI joint pain category includes one yes/no question assessing response to a combination of orthopedic maneuvers. [45] SI joint pain is suggested when 3 or more of 6 positive tests (Gaenslen’s left and right, thigh thrust, sacral thrust, distraction and iliac compression) are present in the absence of centralization. [45–47] When none of the tests are positive, SI joint pain is considered ruled-out.
Zygapophyseal Joint Pain
Lumbar zygapophyseal (Z) joints (or facet joints) are richly innervated with mechanosensitive neurons and free nerve endings. [48] Z-joints receive dual innervation from nerve roots exiting at the same and superior adjacent levels. Innervation extends into subchondral bone providing the potential for pain generation outside the joint. [49] Z-joints are diarthrodial synovial joints exhibiting variable orientation from upper to lower lumbar segments, usually becoming coronal in orientation at L5-S1, presumably as a response to local biomechanical stress. [48, 50] Cohen’s synthesis of existing data reported pain across the lumbosacral junction as the most common distribution. Other reported areas of Z-joint pain distribution include ischial, posterior thigh and groin, upper lumbar and flank, anterior medial thigh, and lateral leg. [49] Cohen also estimated the overall prevalence of primary LBP from Z-joints at between 10 and 15%. [49] One recent clinical study using the same criteria present in the checklist diagnosed 23% of 264 LBP patients with Z-joint pain. [36]
A controlled joint anesthetic block procedure is the standard test to confirm Z-joint pain. According to two recent reviews, controlled comparative anesthetic blocks are supported by level 1 (or ll-1) and by strong evidence. [29, 51] However, anesthetic blocks are invasive, costly, require specialized settings and carry inherent risks. [29]
For zygapophyseal joint pain, a clinical prediction rule is included into the diagnostic checklist. [52] A positive prediction rule indicated by satisfaction of 3 or more of 5 criteria carries a positive likelihood ratio of 9.7. This clinical prediction rule is considered more effective at ruling out facetogenic pain when negative. The strength of evidence supporting the clinical prediction rule could be improved with subsequent validation studies.
Myofascial Pain
Myofascial pain is defined as pain arising from muscles or related fascia. [53] Chronic myofacial pain can be regarded as a form of neuromuscular dysfunction [54, 55] characterized by trigger points or focal areas of hypertonicity and tenderness. [53, 56] The chronic myofascial pain hypothesis includes a sequelae of events leading to trigger point generation that includes excessive acetylcholine release from damaged motor nerve endplates, reduced local blood flow due to muscle contraction, and possible reduced calcium ion re-uptake by contracted muscle and ATP deficit. [56, 57]
At present, there is no gold standard for evaluating myofascial pain and no specific diagnostic tests have been developed. [58] Therefore, the current standards of trigger points, and aggravation with use of the involved muscle(s) are included in the checklist. [58]
Neuropathic Pain
We defined neuropathic pain as generated or perceived from peripheral or central nervous system tissues designated further into 4 subcategories:(1) compressive radiculopathy,
(2) non-compressive radiculopathy,
(3) neurogenic claudication, and
(4) central pain.
Compressive Radiculopathy
Compression of a nerve root can lead to peripheral symptoms and changes in motor and sensory function, often in a dermatome or narrow band-like distribution. [59, 60] Symptomatic compressive radiculopathy may be the result of a combination of inflammation and compression of the dorsal root ganglion or nerve root. [61, 62] Compression and inflammatory mediators arising from extruded nucleus pulposus material or from a degenerating disc have been shown to cause sciatica and hyperalgesia. [61–63] However, the compression model does not explain all neuropathic pain presentations.
Several checklist criteria for this category were derived from a single clinical study evaluating diagnostic information associated with compressive neuropathy confirmed by magnetic resonance imaging. [64] The diagnostic checklist includes symptoms of leg pain worse than back pain, dermatome distribution of pain when coughing, sneezing or straining, lower extremity paresis, and increased finger to floor distance during standing flexion. We also adapted questions from the Leeds Assessment for Neuropathic Symptoms and Signs (LANSS) [53, 65] for use in the checklist. The LANSS is a tool comprised of 5 questions and two examination findings used to help discriminate between nociceptive and neuropathic pain.
Non-compressive Radiculopathy
Non-compressive neuropathic pain is thought to arise from neural tissue exhibiting normal axonal conduction sensitized by inflamed nerve roots, trunks, or other tissue in close proximity. [66, 67] The plexus surrounding peripheral nerve trunks contains free nerve endings capable of mechanoreception and nociception and can become mechanically sensitized (mechanical allodynia) in the presence of inflammation. [66–68] Post-surgical adhesions inhibiting nerve root mobility may also cause neuropathic pain [69] through mechanical sensitization, a process similar or identical to the adherent and entrapped nerve roots described by Petersen. [3]
Evidence suggests that inflamed nerve roots are sensitive to stretch. In an animal model, mechanically sensitized nerves generate nociceptive impulses when stretched. [70, 71] Clinical maneuvers designed to assess elastic tolerance of lower extremity peripheral nerves are the straight leg raise, slump, and femoral nerve stretch tests. [64, 72, 73]
Currently, there is no gold standard test to confirm the diagnosis of non-compressive radiculopathy. Therefore, the diagnostic criteria consist of neurological symptoms without signs of nerve compression and a LANSS score indicating neuropathic pain. Though they cannot be validated by a gold standard test, the straight leg raise, slump and femoral nerve stretch tests likely support this diagnosis in the presence of an appropriate clinical picture.
Neurogenic Claudication
Neurogenic claudication is thought to arise from compression of the cauda equina or nerve root(s) fostered by narrowing (stenosis) of the central spinal canal or neural foramina. [74] Stenosis occurs congenitally or arises from degenerative change to the disc, facets, ligamentum flavum (hypertrophy), or other factors such as degenerative spondylolisthesis and lumbar extension. [74, 75] Physical activity increases neural oxygen demand, resulting in venous engorgement in stenotic areas, neural compression, and ischemia. Ischemia is the most likely pain generating mechanism demonstrated by reversible symptoms in patients with this condition. [74]
Neurogenic claudication typically presents with activity related unilateral or bilateral pain (sometimes weakness or heaviness) radiating into the buttock, thigh and/or leg that is relieved with sitting. Osteoarthritis and bursitis of the hip or knee, peripheral arterial disease (PAD), and several forms of peripheral neuropathy can present similarly and in combination with neurogenic claudication. What appears to be a simple diagnosis can require skillful differentiation. [74, 76]
The criteria in this category were derived from a single study evaluating a clinical prediction rule with expert clinicians serving as the diagnostic standard. [77] A score of 7 or greater on the clinical prediction rule containing 8 questions carries a modest positive likelihood ratio of 3.9.
Differentiating neurogenic and vascular claudication can be particularly challenging. Therefore, a negative Ankle Brachial Index (ABI) was added to the checklist. The ABI test was chosen for its ability to reliably assist in detecting lower extremity vascular compromise and its utility as an in-office assessment. [78–80]
Central Pain
The central nervous system adapts to inflammation, nociceptive activity and/or injury by augmenting neural signaling leading to hypersensitivity (central sensitization). [81] Central sensitization is characterized by an amplified pain response, increased reaction to noxious sensory stimulation (hyperalgesia), convergence of low threshold mechanoreceptor pathways with nociceptive circuits, and pain perceived from otherwise non-painful stimuli (allodynia). [82] Patients with central sensitization perceive real pain. However, there is a departure from the stimulus response relationship of the nociceptive pain mechanism. [82] One recent study classified approximately 23% of 464 patients with low back pain with central sensitization. [83]
Patients with chronic LBP can exhibit signs of central sensitization. [84, 85] Using a Delphi survey of expert clinicians, a consensus-derived list of clinical criteria was developed to identify patients suffering from nociceptive, neuropathic, and central pain. [86] Using these criteria in a clinical study, one sign and three symptoms were identified as consistent with the diagnosis of central pain. [23] These 4 criteria have not been validated in other settings and there is a possibility of bias because the standard to which these criteria were compared was expert opinion, possibly contributing to the high likelihood ratios for these criteria. Nevertheless, it is an important first step toward identifying and standardizing the assessment for clinical characteristics of central pain. This set of criteria represents evidence consistent with current patho-mechanistic understanding and has been shown to be useful and efficient in a clinical setting.Functional Instability
Functional or lumbar segmental instability is described as a disruption in the neuromuscular control of a spinal joint neutral zone during normal physiologic demand resulting in the potential for aberrant motion and loading of local tissue(s). [19, 87] Functional instability is distinct from frank instability, which suggests structural injury or deterioration with the potential for neurological compromise.
It is thought that LBP may alter muscle activity around the lumbar spine, contributing to changes in neuromuscular control mechanisms that maintain position and protect it from injury. [88, 89] The functional instability concept is supported by results from several clinical studies showing improvement in pain and function when introducing specific lumbar stabilization exercises for patients with LBP. [90–92] The prevalence of functional instability was calculated at 12% in a chronic LBP population [93] and 31.1% in patients with lumbar degeneration. [94] However, diagnosis by measuring intervertebral position from lateral lumbar radiographs has not been validated.
The three diagnostic checklist criteria in this category were derived from three clinical diagnostic utility studies and one systematic review. [19, 93–95] They include the presence of any hypermobile segment (+LR 2.4), the absence of any hypomobile segment (+LR 9.0) and the passive lumbar extension test (+LR 8.8). [95] Hypo/hypermobility is assessed with the patient prone while the clinician gently presses anteriorly with the hypothenar eminence on the spinous processes of lumbar vertebrae.
Other diagnosis
This category was designed for LBP diagnoses not included in the checklist. Diagnoses such as thoracolumbar and piriformis syndrome [96–98] could be included here. These diagnoses are not yet supported by studies designed to validate diagnostic criteria and are not as common as others included in the checklist. Therefore, they are more suited for consideration when other more prevalent conditions are ruled-out or as co-presenting conditions.
Clinical Application
The goal of this project was to create a practical, in-office system to consistently diagnose LBP from an evidence-based perspective within the context of chiropractic clinical research and in private settings. We combined available scientific evidence into a user-friendly tool to provide an aid for more consistent diagnosis for practitioners, researchers, and students.
The checklist format enables the examiner to mark findings and visually observe how the evidence supports or fails to support a given diagnosis. Visually categorizing where the most evidence lies may help clinicians organize diagnostic information and aid them in clinical decision-making. Because of the limitations of current validated tests and diagnostic criteria, the checklist, in general, may be more effective at ruling out categories.
Examination procedures are minimal as much information comes from the clinical interview. The checklist identifies when a specific evaluation or test is required ensuring it as a stand-alone document. Appendix B is available as a single page reference to show the examination procedures included in the checklist. Some checklist categories do not state a minimum number of items necessary to conclude or rule out a diagnosis (i.e., compressive radiculopathy, discogenic pain). In all categories, checked items show where evidence is or is not clustering. Clustered evidence does not guarantee accuracy and sometimes indicates more than one diagnosis. In these instances, the checklist can help establish an evidence-based differential diagnosis or the possibility of pain arising from concurrent conditions. We submit that identifying diagnoses with clustered evidence is superior to the diagnosis of non-specific LBP because it provides a pathophysiological basis for targeted clinical decisions regarding management, progress evaluation, need for testing, and a consistent framework to facilitate communication with patients and other providers.
LBP diagnosis is challenging as evidenced by calls for additional research on classification [1, 2] The checklist presented in this article is best used by the astute and experienced clinician. It is not a diagnostic template, but rather an aid. Without incorporating all aspects of the clinical presentation, checklist items can be interpreted as indicating evidence for what could be an incorrect diagnosis. Consider a patient with a score of 7 on the neurogenic claudication clinical prediction rule and a negative ABI. Using only the checklist, this evidence suggests a diagnosis of neurogenic claudication.
However, the true diagnosis could conceivably be pain originating from hip or knee joint osteoarthritis. Without differential examination, diagnostic accuracy could suffer. Therefore, checklist items indicating a diagnosis are most useful when balanced with a consistent clinical presentation and supported by differential examination whenever possible.
From a clinical perspective, this classification system represents an evidence-based approach to LBP diagnosis, which aids understanding of dysfunctional physiology, provides rationale for developing management strategies with patients and other providers, aids communication with patients and third-party payers, provides a common framework for interprofessional communication, and supports the education of student clinicians.
The classification system proposed in this article does not assess depression, post-traumatic stress disorder, or psychosocial factors important in the broader context of clinical diagnosis. These tools already exist, and at our center psychosocial components are screened with the clinical interview and established instruments such as the Patient Health Questionnaire-9 (PHQ-9) [99] and Generalized Anxiety Disorder-7 (GAD-7). [100]
Systematic reviews of each diagnostic category were not performed to develop this classification system. Clinicians are encouraged to examine the evidence supporting individual diagnostic categories. The effectiveness with which the checklist can aid clinicians in consistently diagnosing LBP has not yet been reported. The authors are engaged in ongoing studies designed to report reliability and LBP diagnoses generated with this system to further refine the evidence-based approach. Another logical next step is a hypothesis setting study to begin validation testing. [12]
Limitations
Until the development of new or improved comparative diagnostic methods, several checklist categories will be supported by construct validity and what is considered low-quality evidence, a common occurrence in many healthcare areas. It is important for clinicians to be aware of the strengths and limitations of the evidence on which diagnostic decisions are based. Second, diagnosis is inherently an art, thus difficult to standardize. A diagnosis derived with the aid of the exam and checklist is at least somewhat dependent on the knowledge, skill, experience and perceptiveness of the diagnostician. Third, new evidence is constantly emerging and a systematic review of the literature was not performed. Therefore, articles reporting studies of diagnostic testing may have been missed.
Summary
Recognizing the need for a standardized, evidence-based method to evaluate and diagnose LBP, we created an evidence-based diagnostic classification system with accompanying clinical exam and checklist tool. The use of evidence-based diagnostic methods to differentiate and classify LBP in research and traditional clinical settings is encouraged.
Acknowledgments
This work was partially funded through a grant from the National Institute of Health’s National Center for Complementary and Alternative Medicine (NCCAM) (1U19AT004137). This project was conducted in a facility constructed with support from Research Facilities Improvement Grant Number C06 RR15433 from the National Center for Research Resources, National Institutes of Health. The authors wish to thank Stacie Salsbury PhD, RN for her critical review of the manuscript.
Please refer to the Full Text Article for the following:
Appendix A. Diagnostic Classification Checklist:
Appendix B. Clinical evaluation procedures included in the diagnostic classification checklist
Return to LOW BACK PAIN
Return to CLINICAL PREDICTION RULE
Return to THE DIAGNOSIS AND MANAGEMENT
Since 9-14-2013
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |