

Straight Chiropractic Philosophy As A Barrier
To Medicare Compliance: A Discussion
of 5 Incongruent IssuesThis section was compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Chiropractic Humanities 2013 (Oct 24); 20 (1): 19–26 ~ FULL TEXT
OPEN ACCESS David R. Seaman, DC, MS, Jonathan R. Soltys, DC, MS
Professor,
National University of Health Sciences,
Pinellas Park, FL.OBJECTIVE: The purpose of this commentary is to discuss potential 5 factors within straight chiropractic philosophy and practice that may prevent Medicare compliance.
DISCUSSION: The national Medicare Benefit Policy Manual and the Florida Local Coverage Determination were reviewed to identify documentation and conceptual issues regarding chiropractic practice. Five Medicare positions were contrasted with tenets of straight chiropractic philosophy. Based on Medicare's documentation requirements, Medicare defines subluxation and chiropractic practice from the perspective of treating spinal pain and related functional disability. In contrast, traditional straight chiropractic philosophy is not based on the treatment of spinal pain and disability or other symptomatic presentations. In this context, 5 potential areas of conflict are discussed.
CONCLUSION: The Medicare version of chiropractic practice is not consistent with traditional straight chiropractic philosophy, which may play a role in preventing Medicare compliance. The chiropractic profession may need to consider the fashion in which "philosophy" as it relates to technique and practice is presented to students and doctors to facilitate compliance with the documentation requirements of Medicare.
KEYWORDS: Back pain; Chiropractic; Manipulation; Medicare; Philosophy; Spinal
From the FULL TEXT Article:
Introduction
Chiropractic education requires that students learn appropriate documentation in the classroom and then apply this knowledge during patient care in the institution’s clinics. Chiropractic interns are thoroughly trained in their clinical documentation skills; so we would expect that their practice behaviors regarding Medicare patients also would be thorough, appropriate, and compliant. However, according to the Office of Inspector General report in 2009, approximately 83% of the claims submitted to Medicare had deficiencies in documentation, coding, and billing, which led to inappropriate payments. [1]
In 2006, Medicare paid $466 million for chiropractic services. [1] Reviewers determined that approximately 47% of payments were inappropriate; $157 million was inappropriately paid for maintenance therapy, $46 million was paid for undocumented care, and $11 million was paid for miscoded care. [1]
Distinct from the undocumented claims, 83% of reviewed chiropractic claims failed to meet one or more of the documentation requirements. Concerning treatment, file reviewers reported that only 76% contained some form of treatment plan, 43% lacked treatment goals, 17% lacked objective measures, and 15% lacked the recommended level of care. [1]
The documentation requirements for Medicare patients are uncomplicated and outlined in the Local Coverage Determination (LCD) by the area contractor that administers Medicare claims, [2–4] which are all consistent with the Medicare Benefit Policy Manual that is published by the Centers for Medicare and Medicaid Services. [5]
Of interest and concern is that Medicare documentation requirements are not unique to Medicare; they are outlined in texts authored by doctors of chiropractic6,7 and are taught to students in chiropractic institutions. Despite this, only an estimated 17% of doctors of chiropractic are able to comply with Medicare documentation requirements. [1] Not only is the quality of patient care affected, as postpayment audit penalties generated by noncompliant documentation practices can be extensive and financially devastating to the practitioner.
To improve patient care and compliance, areas of conflict need to be identified, examined, and corrected. Therefore, the purpose of this commentary is to discuss potential factors within chiropractic education and practice that may influence Medicare compliance.
Discussion
Medicare requirements
The documentation requirements for Medicare are outlined in the LCD, [2–4] which is consistent with the Medicare Benefit Policy Manual that is published by the Centers for Medicare and Medicaid Services. [5] For this discussion, we chose the Florida LCD because we feel that it most closely articulates the purpose of chiropractic practice based on the documentation requirements that operationally define the subluxation and the appropriate use of chiropractic manipulation. [2] The Medicare Benefit Policy Manual and LCDs outline specific pain-based documentation requirements that must be identified during the initial visit. The initial documentation requirements include a history, description of the present illness, physical examination findings, a diagnosis, a treatment plan, and the date of initial treatment or date of exacerbation or reinjury of the existing condition. These include the symptoms causing the patient to seek treatment, which must emanate from the spine; the mechanism of trauma; the quality and character of symptoms/problem; the onset duration, intensity, frequency, location, and radiation of symptoms; and the aggravating or relieving factors. On days during which a treatment is provided, documentation requirements include an updated history, evaluation findings, documentation of treatment, and any changes in the treatment plan. With these documentation requirements in mind, Medicare further requires that doctors of chiropractic demonstrate medical necessity and document that the spine is the generator of the presenting symptoms.
Straight chiropractic philosophy
For the purpose of this discussion and to contrast the Medicare position with traditional straight chiropractic philosophy, we chose positions offered by 2 subluxation-based chiropractic guidelines, including the Practice Guidelines for Straight Chiropractic (PGSC) [8] and the Clinical Practice Guideline: Vertebral Subluxation in Clinical Practice (VSCP), [9] and a textbook that examined technique systems in chiropractic. [10] Although there are various definitions of vertebral subluxation (including Medicare's definition), these are consensus statements and are not currently evidence based.
However, for the purpose of this discussion of Medicare, the documentation requirements are specific and thus, for this argument, represent the operational definition of subluxation, independent of personal and consensus definitions of subluxation.
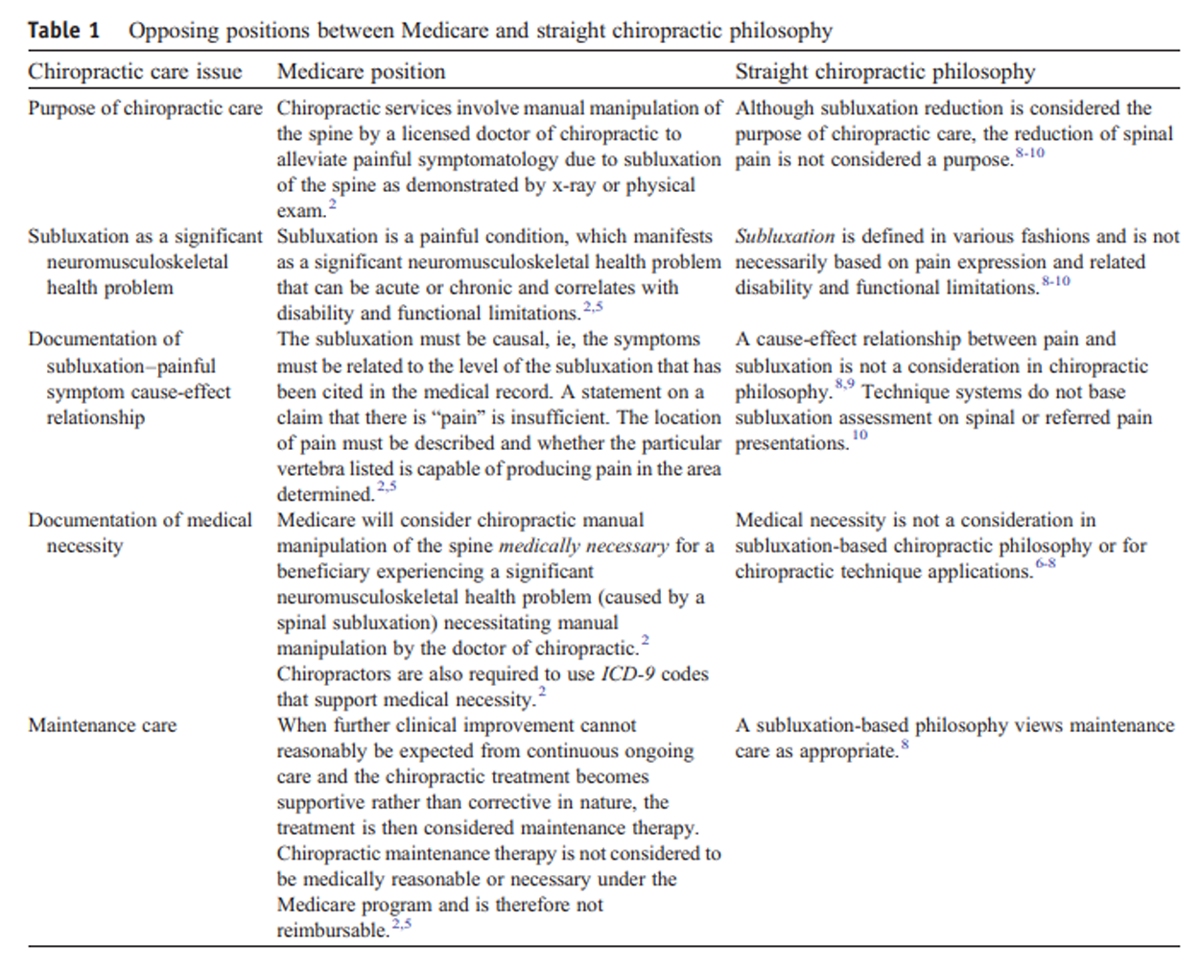
Comparison Medicare has taken a position on the purpose of chiropractic care, the nature of subluxation, and maintenance care. To identify potential barriers to documentation compliance, the Medicare position on these 5 topics is contrasted with that of the traditional straight chiropractic philosophy documents stated above.

Table 1 We selected 5 chiropractic care issues and compare opposing positions between Medicare and straight chiropractic philosophy (Table 1). This comparison suggests that the pain/disability-based Medicare version of chiropractic practice is not consistent with straight chiropractic philosophy.
The Medicare Benefit Policy Manual and the LCDs function to operationally define chiropractic practice and subluxation by specific pain-based documentation requirements. Consequently, to comply with Medicare requirements, doctors of chiropractic should view chiropractic practice and subluxation from this perspective when treating a Medicare patient. If this perspective is not taken, it is possible to misunderstand Medicare documentation and management requirements, which may lead to noncompliance issues for practitioners. The following further describes details surrounding these 5 issues.
Purpose of chiropractic care
The Florida LCD states that “chiropractic services involve manual manipulation of the spine by a licensed doctor of chiropractic to alleviate painful symptomatology due to subluxation of the spine as demonstrated by x-ray or physical exam.” [2] The LCD for Illinois, Minnesota, Wisconsin, Connecticut, and New York states that “Chiropractic manipulative treatment (CMT) is a form of manual treatment to influence joint and neurophysiological function.” [3] Other LCDs use terminology very similar or identical to that which is found in the Medicare Benefit Policy Manual that states5: “the term ‘physician’ under Part B includes a chiropractor who meets the specified qualifying requirements set forth in §30.5 but only for treatment by means of manual manipulation of the spine to correct a subluxation.”
A potential misinterpretation would be that, in Florida, the purpose of chiropractic is to treat spinal pain with manipulation; however, elsewhere in the United States, the purpose is to correct subluxation or to influence neurological function. Although it would appear that this is a discrepancy, no discrepancy actually exists. This is clarified by how Medicare operationally defines subluxation correction/treatment in the context of the documentation and management of Medicare patients, which is identical in the Medicare Benefit Policy Manual and all the LCDs, including Florida. The patient history is to include the symptoms causing the patient to seek treatment, which must emanate from the spine; the mechanism of trauma; the quality and character of symptoms/problem; the onset duration, intensity, frequency, location, and radiation of symptoms; and the aggravating or relieving factors. The symptoms should be reported as pain (algia), inflammation (itis), or as signs such as swelling spasticity, etc.
The LCD for the states of Maine, Massachusetts, New Hampshire, Rhode Island, and Vermont supports the clear terminology of the Florida LCD by stating that “Spinal Axis, aches, strains, sprains, nerve pains, and functional mechanical disabilities of the spine are considered to provide therapeutic grounds for chiropractic manipulative treatment.” [4] Clearly, from the perspective of Medicare, the purpose of chiropractic care is to document and manage spinal pain and disability.
In contrast, the PGSC states that “proper function rather than symptomatic relief is the paradigm of the chiropractic standard of care” ([8], p99). The VSCP explains that pain and symptoms are not necessary correlates of vertebral subluxation ([9], p83) and that chiropractic care is indicated and would be prudent even in the absence of pain symptoms ([9], p215). Chestnut11 specifically states that “‘manipulating for pain relief’ is not chiropractic.”
Spinal pain identification and reduction are not stated components of straight technique systems, which instead focus on the correction of subluxation, fixations, posture, leg length inequalities, muscle imbalances, and other indicators. [10] Clearly, the stated purpose of chiropractic for Medicare beneficiaries is not consistent with straight chiropractic philosophy.
Subluxation as an important neuromusculoskeletal problem According to Medicare, subluxation is an important neuromusculoskeletal health problem, which cannot be a “painless” condition. Trailblazer Health Enterprises, one of the administrative contractors for Medicare, describes subluxation as being an acute strain/sprain or a chronic loss of spinal joint mobility, each of which manifests as a painful limitation that requires an appropriate International Classification of Diseases, Ninth Revision (ICD-9), diagnosis code. [12] The LCD for Illinois, Minnesota, Wisconsin, and New York describes the use of outcome assessment tools for pain and disability monitoring in Medicare patients [2]:“The evaluation process must be an ongoing procedure. Even if a complete and thorough examination can be completed during the first visit, signs and certain symptoms must be rechecked during the course of treatment to determine the extent of the patient progress. Standardized measurement scales (e.g., Visual Analogue Scale (VAS), Oswestry Disability Questionnaire, and the Quebec Back Pain Disability Scale) may be used to measure improvement or lack thereof.”
Pain may be the outcome of strains, sprains, and chronic hypomobility in individuals 65 years and older; and the recommended use of outcome assessment tools for the management of pain and disability is confirmatory.
However, from the perspective of traditional straight chiropractic philosophy, the accepted definitions of subluxation and related treatment do not identify subluxation in the pain-based fashion as defined by Medicare. For example, the PGSC defines subluxation in the following fashions:“A misalignment of one or more articulations of the spinal column or its immediate weight-bearing articulations, to a degree less than a luxation, which by inference causes alteration of nerve function and interference to the transmission of mental impulses, resulting in a lessening of the body’s innate ability to express its maximum health potential.” ([8], p29)
The VSCP advances the notion that subluxations interfere with the transmission of mental impulses ([9], p164), which refers to the expression and activity of innate intelligence.13 This traditional view of subluxation does not consider symptoms as relevant. Instead, the purpose is to prevent symptoms by the reduction of symptomless subluxations as an approach to wellness. [11] Whether valid or not, this view of subluxation is not consistent with Medicare’s position that subluxation is an important neuromusculoskeletal health problem.
Although Medicare documentation revolves around the management of spinal pain and disability, some may still argue against this because only 2 of 4 criteria are required by Medicare to document a subluxation. [2–4, 12] The 4 criteria, referred to as PART, include pain, asymmetry, range of motion abnormality, and soft tissue changes, of which one must be asymmetry/misalignment or range of motion abnormality. The fact that pain is not required in the PART aspect of subluxation documentation can lead to the misinterpretation that Medicare documentation is not pain based. However, the documentation requirements described previously demonstrates that, from the perspective of Medicare, the purpose of chiropractic care is to manage spinal pain and disability.
Why then would pain not be required for PART documentation? An example would be a patient with cervicogenic vertigo or other vertebrogenic symptoms who does not have spine pain. The documentation requirements do not change, save for the fact that pain is the not the presenting symptom. From the authors’ perspective, this is a defect in Medicare documentation requirements for doctors of chiropratic, which should specify that pain be a required documentation component within the PART criteria if the patient is complaining of vertebrogenic pain.
Documentation of subluxation-symptom cause-effect relationship Medicare requires that the subluxation be causally linked to the painful presentation. In other words, the chosen “subluxated” vertebrae to be adjusted must be able to generate the painful complaints of the patient. This request from Medicare is no different than requiring a spine surgeon to identify the proper level of the painful herniated disk to be removed. It is the authors’ impression that the PART criteria should be viewed in the context of this documentation requirement that specifies that the vertebral level to be adjusted is capable of generating the painful symptoms.
Traditional straight chiropractic philosophy does not address pain and disability in this context. The focus is espoused to remove subluxations without concern for symptomatic expression. [8–11] Kent [14] states the chiropractic philosophy perspective on this topic: “Although stimulation of articular mechanoreceptors may exert an analgesic effect, use of manipulation for the episodic, symptomatic treatment of pain is not chiropractic.”
However, this is precisely the purpose and valuable contribution that chiropractic has to offer, from the perspective of Medicare.
Establishment of medical necessity Regarding medical necessity, the Social Security Act (Section 1862[a][1]) prohibits payment for services or procedures that are not “reasonable and necessary for the diagnosis or treatment of an illness or injury or to improve the functioning of a malformed body member” (http://www.ssa.gov/OP_Home/ssact/title18/1862.htm). Therefore, we propose that the establishment of medical necessity for chiropractic care requires that a Medicare patient presents with a painful neuromusculoskeletal condition—which limits activities of daily living—that has been identified in the patient history and physical examination and correlated with a spinal subluxation that is amenable to chiropractic care. [2–5, 12] In other words, Medicare requires that the spine is “causal,” which supports chiropractic manipulation as being “medically necessary.” This would be in contrast to back pain caused by an abdominal aortic aneurysm or prostate cancer, which supports surgery or chemotherapy as the medically necessary procedure. Medicare further requires the use of a specific ICD-9 code to support medical necessity of chiropractic care. Straight chiropractic philosophy does not use the establishment of medical necessity as a criterion for delivering chiropractic care. [8–11]
Maintenance care Despite the emerging evidence that regular spinal manipulation may reduce the incidence of spinal pain and disability, [15] Medicare does not currently reimburse doctors of chiropractic for maintenance care of the spine. The anti–maintenance care position of Medicare finds strong opposition from straight chiropractors, who view maintenance care as far more significant than merely preventing spinal pain. The purpose of maintenance care from the viewpoint of straight chiropractic philosophy (as opposed to biomedicine) is the removal of subluxations to promote an overall health benefit without consideration of symptoms [16]:“It is the position of the World Chiropractic Alliance that chiropractic care to detect and correct vertebral subluxations offers benefits for all people, including those who do not demonstrate symptoms of a disease or health condition. Therefore, the presence of symptoms and/or a medical diagnosis should not be a factor in determining the need for or appropriateness of chiropractic adjustments, nor should the presence of symptoms be required by any chiropractic board, insurance company or court of law to justify the rendering of chiropractic care to any patient.”
The subject of maintenance care may be viewed as appropriate from the perspective of straight chiropractic philosophy. And by not reimbursing for maintenance care, Medicare appears to reject a major premise of straight chiropractic philosophy, which advocates for a bigger worldview of subluxation and a distinct identity of chiropractic. Chestnut [17] explains:
“The philosophy of chiropractic defines its intent, states its major premise, and establishes its paradigm. The philosophy of chiropractic is an amalgamation of vitalism, holism, naturalism, conservatism, and critical rationalism and this philosophy has created a distinct health paradigm unique to chiropractic.”
With this perspective in mind, a natural consequence would be to reject Medicare’s notion that the chiropractic intervention should involve the alleviation of pain and functional disability. Rather than reducing pain and disability, subluxation reduction is viewed as impacting human genetic expression [17]:
“Therefore, natural interventions such as the chiropractic adjustment and the related therapeutic interventions aimed at removing vertebral subluxation complex and assisting the whole person to utilize their innate abilities to restore and maintain their genetic potential for health and wellness fall into the realm of chiropractic.”
Determining whether this view of spinal care is valid is not the purpose of this investigation. Valid or not, there appears to be a significant inconsistency between straight chiropractic philosophy and the documentation requirements to be compliant with Medicare guidelines.
Origins of the challenges for the chiropractic profession and suggestions for moving forward At present, Medicare only reimburses doctors of chiropractic for spinal manipulation based on medical necessity. Codes for evaluation and management, rehabilitation, and other modalities are not reimbursable. It should be understood that, although the documentation requirements for Medicare are written as being pain based, this does not mean that patients with other vertebrogenic symptoms should not be treated. As mentioned earlier, cervicogenic vertigo is an example of such a condition, which may respond to manipulation. [18] In this case, the same documentation and management criteria would apply, the difference being vertigo as the symptom, rather than pain. The likely reason for the pain-based requirements of Medicare is that pain is the most common vertebrogenic symptom encountered in clinical practice.
An important consideration for the chiropractic profession is that, no matter the symptomatic presentation, embracing the nonpain and nonsymptom focus of straight chiropractic philosophy would still lead to documentation challenges. Overcoming this issue is a challenge that must be addressed. It has been recommended that chiropractic philosophy be taught in its historical context, rather than in a doctrinal fashion. [19] We know that “chiropractic philosophy” originated as a successful legal defense that was developed in 1907 by BJ Palmer and attorney Tom Morris to defend doctors of chiropractic against charges of practicing osteopathy and medicine without a license. [19–21] Consider the following statement made by BJ Palmer in 1951 [20]:“We are always mindful of those early days when UCA … used various expedients to defeat medical court prosecutions. We legally squirmed this way and that, here and there. We did not diagnose, treat or cure disease. We analyze, adjusted cause, and Innate in the patient cured. All were matters of fact in science, therefore justifiable in legal use to defeat medical trials and convictions.”
Of interest to note is that BJ Palmer and John Howard, founder of the National School of Chiropractic, agreed on this fact. In other words, we, the chiropractic profession, created unique terminology and a unique “philosophy” for the purpose of legal protection. Howard stated it this way [20]:
“It has always been a sore in my eye to see how some who profess to be disciples of DD Palmer have tried and still insist on narrowing the science down to a simple technique. In the early days it was necessary to protect the ‘child’ (as DD was wont to refer to his chiropractic) by evasive terminology in order to avoid the chill and ice of the law and ‘analysis’ was used for diagnosis, ‘adjustment’ was employed for treatment, ‘pressure on the nerve’ was used for reflex stimulation or inhibition, etc. These terms were garments to protect the child until legal clothing could be secured.”
Before lawsuits began in 1907, BJ Palmer described chiropractic only as a science, not a science, art, and philosophy. [20] He also took out full-page adds in the Davenport Times, [22] in which he laid claim to curing numerous conditions and stated clearly that “I treat all diseases.” He did not state that the adjustment removes subluxation, that Innate within the body did the healing, or that lifetime wellness care was needed. In fact, he stated that he charged patients by the week because it would be unjust to charge by the month [22]:
“The Osteopaths charge by the month. Why do I charge by the week? Because the Chiropractic cures many in one or two weeks. It would not be justice to charge such for a full month. Our patients average about two weeks treatment.”
Understanding that straight chiropractic philosophy was a legal argument, rather than a foundational principle of chiropractic, should be impetus to reframe how chiropractic philosophy is taught and embraced by the profession. As doctors of chiropractic are now licensed in all 50 US states, the chiropractic profession no longer needs to embrace a philosophical legal defense as a practice guideline. And if the early prosecutions did not occur, it is possible that the nondiagnostic and nontreatment approach of straight chiropractic would never have emerged, which might have altered the current future to one where we find ourselves more compliant with traditional patient documentation requirements. It is further interesting to speculate that BJ Palmer might not be a promoter of straight chiropractic now that the profession is licensed. His nerve tracing method could be viewed as evidence that linking symptoms to a specific vertebral level is an important foundational principle of chiropractic and is consistent with Medicare documentation and management requirements.
Regarding chiropractic technique systems based in straight chiropractic philosophy, they may be best taught in concert with spinal pain diagnosis and management. Diagnostic algorithms [6] and a diagnosis-based clinical decision guide may be beneficial in this regard. [23–29] It is also reasonable to teach spinal manipulation as part of a management approach for spinal pain syndromes, rather than solely as part of a technique system that is not symptom based and not able to limit or prevent Medicare documentation problems.
Limitations
At present, the information presented in this study, although reasonable on paper, remains theoretical, which is a limitation. To most past speculation, a more detailed investigation is required to properly identify potential educational and practice issues that promote noncompliance with Medicare documentation. The purpose of this commentary was not to debate or define the term subluxation; thus, readers are directed to other publications on this topic. [30–32] A specific and definitive cause-effect relationship cannot be established to demonstrate that training in chiropractic philosophy and technique play a role in preventing Medicare compliance. Investigative studies would need to be accomplished to evaluate that relationship.
Conclusion
This commentary has contrasted current straight chiropractic philosophical concepts with Medicare requirements. We suggest that straight chiropractic philosophy, which is subluxation based without consideration for symptoms, may foster a mindset that is in direct conflict with pain-based Medicare guidelines for the practice of chiropractic. Chiropractic care and related documentation for Medicare beneficiaries are distinctly pain based and disability based, whereas straight chiropractic philosophy does not address pain or disability. The chiropractic profession needs to consider the fashion in which “philosophy” as it relates to technique and practice is presented to students and doctors to facilitate compliance with the documentation requirements of Medicare.
Contributorship Information
Concept development (provided idea for the research): DRS, JRS
Analysis/interpretation (responsible for statistical analysis, evaluation, and presentation of the results): DRS, JRS
Literature search (performed the literature search): DRS, JRS
Writing (responsible for writing a substantive part of the manuscript): DRS, JRS
Critical review (revised manuscript for intellectual content, this does not relate to spelling and grammar checking): DRS, JRS
References:
Office of Inspector General
Inappropriate Medicare payments for chiropractic services.
Dept Health Human Services. May. 2009.
http://oig.hhs.gov/oei/reports/oei-07-07-00390.pdfLocal coverage determination for chiropractic services in Florida.
First Coast Service Options, Inc. Florida
contractor/administrator for Medicare—part B.
http://medicare.fcso.com/Fee_lookup/
LCDDisplay.asp?id=29099&submitcode=+Submit+LCD for Illinois, Minnesota, Wisconsin, Connecticut, and New York.
Acquired from the Medical Policy Center on the, www.ngsmedicare.com Web site.
In upper right corner of homepage, select Part B and enter keyword L27350
in the Site Search field to access the LCD for chiropractic services.LCD for Maine, Massachusetts, New Hampshire, Rhode Island and Vermont.
Acquired from NHIC Web site at.
http://www.medicarenhic.com/providers/pubs/
REF-EDO-0006%20NE%20Chiropractic%20Billing%20Guide.pdfCenter for Medicare Services Medicare benefit policy manual.
Chapter 15—covered medical and other health services.
http://www.cms.gov/manuals/Downloads/bp102c15.pdfSouza T.A. 4th ed.
Jones and Bartlett; Boston: 2009.
Differential diagnosis and management for the chiropractors:
protocols and algorithmsWyatt L.H. 2nd ed.
Jones and Bartlett; Boston: 2005.
Handbook of clinical chiropractic careProceedings of International Straight Chiropractic.
World Chiropractic Alliance; 1993.
Practice guidelines for straight chiropractic; p. 29Council on Chiropractic Practice.
Clinical practice guideline.
Vertebral Subluxation in Chiropractic Practice (2008)Cooperstein R., Gleberzon B.J.
Churchill Livingstone; New York: 2004.
Technique systems in chiropracticChestnut J.
Designing, conducting & publishing research within
the chiropractic wellness paradigm—part 2.
J Vertebral Subluxation Res. 2008:1–3Chiropractic Services.
TrailBlazer Health Enterprises.
Centers for Medicare Services.
Part B. September 2011. Pg.2–3.
http://www.kmcuniversity.com/wp-content/
uploads/ChiropracticServices%20TBHE.pdf.Stephenson R.W.
Palmer School of Chiropractic; Davenport (IA): 1927.
Chiropractic text bookKent C.
Models of Vertebral Subluxation: A Review.
J Vert Sublux Res. 1996 (Aug); 1 (1): 1–7Senna M.K., Machaly S.A.
Does Maintained Spinal Manipulation Therapy for Chronic Non-specific
Low Back Pain Result in Better Long Term Outcome?
Spine (Phila Pa 1976) 2011 (Aug 15); 36 (18): 1427–1437WCA position paper on chiropractic care for asymptomatic patients.
Chiropractic Journal. 2002
http://www.worldchiropracticalliance.org/mission-of-the-world-
chiropractic-alliance/position-paper/position-paper-on-
chiropractic-for-asymptomatic-patientsChestnut J.
Designing, conducting & publishing research within the
chiropractic wellness paradigm—part 1.
J Vertebral Subluxation Res. 2008:1–3Fitz-Ritson D.
Assessment of cervicogenic vertigo.
J Manipulative Physiol Ther. 1991;14(3):193–198Coulter ID.
Chiropractic: a philosophy for alternative health care.
Oxford: Butterworth Heinemann; 1999:
misnomer, p. 1;
legal defense, p.4.Keating J.C.
B.J. of Davenport: the early years of chiropractic.
Association of Chiropractic History;
Davenport (IA): 1997. pp. 64–65Johnson C.
Reflecting on 115 Years:
The Chiropractic Profession's Philosophical Path
J Chiropractic Humanities 2010 (Dec); 17 (1): 1–5Palmer B.J.
I offer something different-better.
The Davenport Times. 1902;13:15Murphy D.R.
A Clinical Model for the Diagnosis and Management of
Patients with Cervical Spine Syndromes
Australasian Chiropractic & Osteopathy 2004 (Nov); 12 (2): 57–71Murphy DR Hurwitz EL:
A Theoretical Model for the Development of a Diagnosis-based Clinical
Decision Rule for the Management of Patients with Spinal Pain
BMC Musculoskelet Disord. 2007 (Aug 3); 8: 75Murphy D, Hurwitz E, Nelson C:
A Diagnosis-based Clinical Decision Rule For Spinal Pain
Part 2: Review Of The Literature
Chiropractic & Osteopathy 2008 (Aug 11); 16: 7Murphy DR, Hurwitz EL, McGovern EE:
Outcome of Pregnancy-Related Lumbopelvic Pain
Treated According to a Diagnosis-Based Decision Rule:
A Prospective Observational Cohort Study
J Manipulative Physiol Ther 2009 (Oct); 32 (8): 616–624Murphy DR, Hurwitz EL, McGovern EE:
A Nonsurgical Approach to the Management of Patients With
Lumbar Radiculopathy Secondary to Herniated Disk:
A Prospective Observational Cohort Study With Follow-Up
J Manipulative Physiol Ther 2009, 32(9):723-733Murphy DR, Hurwitz EL.
Application of a Diagnosis-Based Clinical Decision Guide
in Patients with Neck Pain
Chiropractic & Manual Therapies 2011 (Aug 27); 19 (1): 19Murphy DR, Hurwitz EL.
Application of a Diagnosis-Based Clinical Decision Guide
in Patients with Low Back Pain
Chiropractic & Manual Therapies 2011 (Oct 22); 19: 26Johnson C.
Use of the Term Subluxation in Publications During
the Formative Years of the Chiropractic Profession
J Chiropractic Humanities 2011 (Dec); 18 (1): 1–9Good, C.
The Great Subluxation Debate: A Centrist's Perspective
J Chiropractic Humanities 2010 (Jun); 17 (1): 33–39Venon H.
Historical Overview and Update on Subluxation Theories
Journal of Chiropractic Humanities 2010 (Dec); 17 (1): 22–32
Return to MEDICARE
Return to THE NAYSAYERS CORNER
Since 7-11-2016
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |