

Collaborative Community-Based Teaching Clinics at the
Canadian Memorial Chiropractic College: Addressing
the Needs of Local Poor CommunitiesThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Manipulative Physiol Ther 2007 (Oct); 30 (8): 558–565 ~ FULL TEXT
OPEN ACCESS Deborah Kopansky-Giles, DC • Howard Vernon, DC, PhD • Igor Steiman, DC, MSc •
Philip Decina, DC • Jarrod Goldin, DC • Maureen Kelly, MPA
Canadian Memorial Chiropractic College,
Toronto, Ontario, Canada.

Introduction: Inequities in access to health services, resulting from cuts in public sector budgets and inflation, greatly affect Canada's poorest and most vulnerable people. The purpose of this article is to describe the experiences of the community-based teaching clinics of the Canadian Memorial Chiropractic College (CMCC), located in the poor, inner city region of Toronto, where access to chiropractic care for this population has been enabled.
Discussion: Three chiropractic teaching clinics have been established in host facilities in the inner city community of Toronto. For over a decade, CMCC has had collaborative chiropractic clinics in the Sherbourne Health Centre (a southeast Toronto primary care facility), and Anishnawbe Health Toronto (an aboriginal health facility addressing the needs of urban First Nations people). For 3 years, we have been providing chiropractic services in the Department of Family and Community Medicine at St Michael's Hospital. The priority for these programs was the minimization of economic barriers to accessing care for poor and marginalized people. Outcomes have demonstrated high use when there is no economic barrier, excellent clinical outcomes and patient satisfaction, and a high level of collaboration with other health practitioners.
Conclusion: The CMCC's external clinics program has enabled access to chiropractic services to thousands of people living in the inner city and urban aboriginal communities of Toronto. This has resulted in the minimization of barriers to accessing care, the provision of appropriate and effective care, and collaboration. These clinics also greatly increase students' awareness of, sensitivity to, and commitment to being part of the solution to these problems.
Key Indexing Terms Poverty • Collaboration • Chiropractic • Musculoskeletal Conditions • Indigenous • Urban Health
From the FULL TEXT Article:
Introduction
According to the World Health Organization consultation paper Poverty and Health, it is generally understood that poverty increases the risk of ill health and vulnerability in the poor. It is also known that poverty impedes the effective delivery of health services through reduced demand for services, lack of continuity or compliance with care, and limited access to health services. [1]
Inequities in access to health services resulting from cuts in public sector budgets and inflation most greatly affect Canada's poorest communities and most vulnerable people. There is growing evidence that health-related risk events may well be the first step towards permanent poverty. Therefore, lack of adequate free or low-cost health services for those unable to pay may contribute to the impoverishment of the poor or marginalized communities in many ways. According to the World Health Organization, “These concerns on poverty and ill health help to show not only the dilemma posed by increasing poverty levels but also challenge the current health care model based on free market approach in favor of a comprehensive ‘health for all’ approach through primary health care.” [1]
Many of these inequalities in health, both within and between countries, are due to inequalities in the social conditions in which people live and work. [2] These social determinants have an important effect on health status and general wellbeing. In the United States, the Office of Disease Prevention and Health Promotion identified similar health inequities and subsequently has developed a national initiative to address these issues (Healthy People 2010). [3] In addition, many health care organizations are attempting to respond to these underlying causes of poor health and are committed to improving health and health equity by creating innovative models of health care delivery, aimed specifically at poor and vulnerable populations.
Concerns about chronic disease and disability are global. The World Health Organization has recognized that musculoskeletal conditions rank in the top 3 health concerns presenting as a significant global burdens of disease. [4] The Canadian Memorial Chiropractic College (CMCC) recognizes these local and global needs and shares in a commitment to address these issues. To that end, in the last decade, it has established three external teaching clinics in marginalized communities, whereby chiropractic care is made available to the community through a collaborative practice approach or interdisciplinary approach, as described by Boon et al. [5] Clinical faculty members of the CMCC have spent the last decade gaining experience in addressing musculoskeletal disorders in complex, disadvantaged communities through our external teaching clinics program. This program, aimed at delivering accessible chiropractic services to disadvantaged communities, has demonstrated that health improvements can be accomplished with an integrated approach to care of this complex population. Further, it has shown how community awareness can be raised in the student population, resulting in a greater sensitivity to these important issues.
We know from population data that over 80% of the adult population will suffer from back or neck pain at some point in their lives, and at any single point in time, approximately 25% are affected, limiting their ability to function. [6] In Canada, the current priority in health care is to improve access to health care services; to reduce wait times, particularly by vulnerable and diverse populations; and to reform primary health care delivery through interprofessional collaborative practice models. [7]
These emerging and complex health issues, paired with governmental goals, were the impetus for the CMCC to embark on a program of enabling access to chiropractic services for Toronto's poor and marginalized communities through collaboration with partner health organizations. Since the mid 1990s, CMCC's external clinics program has identified and prioritized communities that have had significant barriers to accessing chiropractic services. [8] Over the course of the past decade, we have been providing chiropractic services without economic barrier (or with very minimal economic barrier) in 3 Toronto inner city communities. These clinics include the chiropractic clinic at St Michael's Hospital, and the CMCC teaching clinics at the Sherbourne Health Centre (SHC) and Anishnawbe Health Toronto (AHT), all within a 2-km radius. These clinical programs are examples of where the community (ie, the HIV/AIDS community, the aboriginal community) identified a need and came together with CMCC and local health facilities to create innovative health service programs. [8]
Description of the Toronto Inner City Community
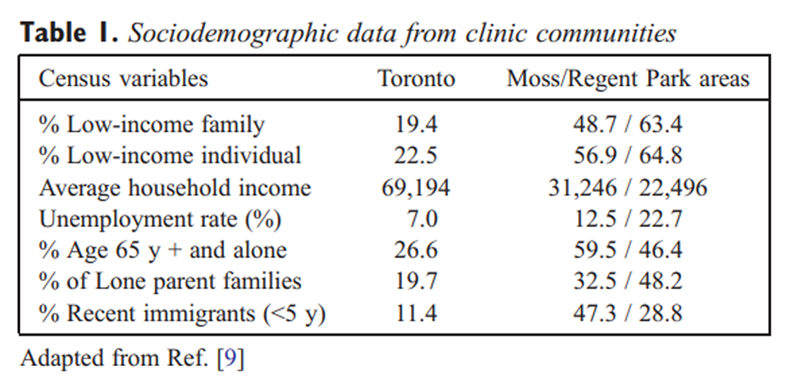
These 3 clinical programs are embedded in the Toronto neighborhoods that represent the poorest and most diverse demographic in the city. The downtown central east region of Toronto is where these 3 clinical programs reside. There has been a significant amount of research describing the health profiles of inner city populations in Canada and the United States. In 2001, Wasylenki described the complex subpopulations in the St Michael's community and the association of poverty with poor health outcomes [10]: “These subpopulations include homeless individuals, people with HIV infection, people with severe and persistent mental illnesses, women at risk due to social isolation, poverty, working in the sex trade or the stresses of single parenthood, and people with addictions.”

Table 1 Transference of the inner city health problems to the broader community also occurs. For example, HIV, tuberculosis, and other communicable diseases transition outward over time, affecting the broader community and increasing the burden of disease. It is imperative, therefore, that a focus for health care reform needs to be prioritization of access to health care by poor, diverse, and marginalized communities in the inner city. Table 1 describes the inner city sociodemographics where our community-based clinics are located.
St Michael's Hospital Chiropractic Program
Figure 1 St Michael's Hospital (Figure 1) was founded in 1892 with a mission to provide compassionate, effective care to disadvantaged populations. The complex health issues faced by inner city communities require coordinated and integrated access to health services — a priority for the St Michael's Inner City Health Program where the Department of Family and Community Medicine (DFCM) and our chiropractic program are housed. In 2004, the St Michael's Hospital, in collaboration with CMCC, commenced an integrated chiropractic service within the DFCM under an initial project grant from the Primary Health Care Transition Fund (Health Canada and the Ministry of Health and Long-Term Care, Ontario, Canada). The demonstration project has been completed, and based on its positive results, the chiropractic services have now become a permanent program, embedded within the DFCM.
This integrated hospital-based community chiropractic health care service offers distinct benefits to the community; it:
reduces barriers to patient access for chiropractic services among the poor and underserved;
nhances quality of health care provided through improved coordination of care in an interdisciplinary practice model;
improves quality of life for the medically underserved;
reduces demand burden on medical and other health care staff and the hospital and the health care system; and
provides health information to promote the prevention of chronic musculoskeletal disorders.
Barrier Reduction
As noted earlier, the St Michael's Hospital clinic is located in central, downtown Toronto, nested amongst the city regions with the poorest socioeconomic status. Clinic demographic data (through postal code tracking) show that over 75% of our patients reside in the economically disadvantaged adjacent communities of Moss Park and Regent Park (noted in Table 1). [9] In general, this population has less access to health services, has more complex health problems, and consequently, has higher admissions to hospitals. [10, 11]
Since the inception of our services, more than 600 patients have been able to access patient-centered chiropractic services, accounting for over 7500 patient visits. There are no service fees for patients to access the care and, therefore, no economic barrier. Over 95% of St Michael's family physicians have referred patients to the chiropractic service over the first 2.5 years of the demonstration project, representing the absence of physician-imposed barriers for patients accessing chiropractic in the hospital setting. Our initial observations suggest that the involvement of chiropractic services within St Michael's Hospital serves a secondary function of linking the underprivileged patient more closely to the primary care system. In this way, chiropractic may provide a means of reducing the loss to follow-up that ultimately carries greater costs when care is delayed. [11] Data on such systemic effects will be the focus of future study.
Interdisciplinary Practice Approach
To ensure collaboration and encourage eventual full integration within the primary care services of the DFCM, a clinical working group composed of physicians, chiropractors, physiotherapists, nurses, and hospital administrators has been meeting regularly in a collegial and inclusive environment. The group plans for program evolution, addresses emerging issues that arise, and discusses recurring clinical scenarios. In addition, new research ideas and interprofessional education initiatives are reviewed. The model has resulted in the successful integration of chiropractic, physiotherapy, and dietetics into a clinic with appropriate referral and triage protocols. The chiropractors play an active role in St Michael's Hospital through involvement in hospital committees, task forces, and working groups.
The chiropractors practice under an evidence-based model responsive to patient needs (patient-centered). They assess, diagnose, and treat a wide range of neuromusculoskeletal disorders. There is direct access to diagnostic imaging, as facilitated by the hospital. Patients are able to access services for a limited period of time, at the discretion of the treating practitioner, until maximum improvement is considered to have occurred. Patients seeking maintenance chiropractic services are referred to the less busy SHC clinic to enable access for other DFCM patients.
The chiropractors also contribute at St Michael's Hospital through involvement in hospital committees, task forces, and working groups. The expertise of the chiropractic staff is increasingly recognized by the hospital, as demonstrated by their participation on a number of hospital committees (HIV Community Advisory Panel, Integrative Therapy Advisory Task Force, Orthotics Working Group, Health Disciplines Council, Interprofessional Education Working Group, Clinical Program Working Group). Recently, one of our chiropractors was selected as one of a very small group of mentors to further the hospital's work on piloting interprofessional collaboration, in partnership with another downtown hospital.
The St Michael's Hospital chiropractic model of care has been entered in the Ontario Ministry of Health and Long-Term Care provincial Best Practices Registry and was accepted by the Ontario Hospital Association as an International Best Practice at their November 2006 conference.
Improved Quality of Life
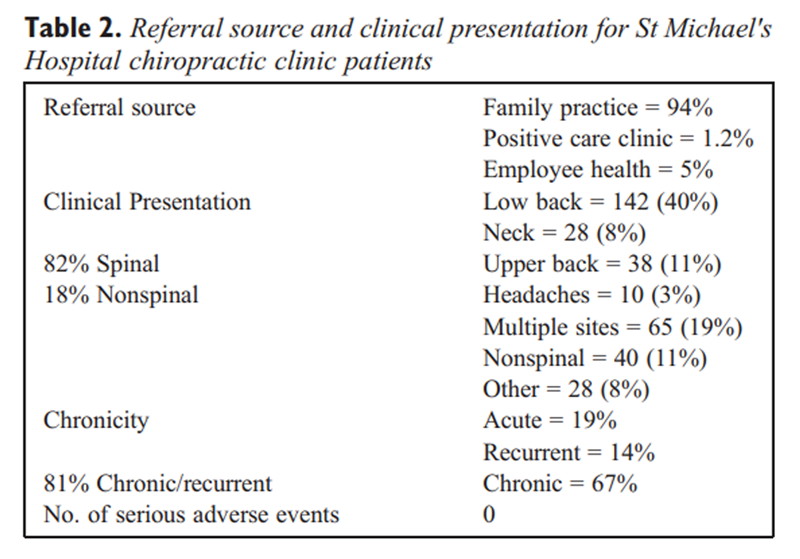
Table 2 Referral of over 600 patients into the clinic from 45 physicians, primarily of the family practice group, was based mainly on the classical musculoskeletal complaints for which chiropractors are commonly consulted, such as back and neck pain, headaches, and pain in the extremities. While under care at the clinic, most patients sought care for additional health concerns. Table 2 gives the clinic statistics for referral sources and case mix. A high proportion of patients present with chronic symptoms and spinal pain. Most patients also have significant health comorbidities, such as diabetes, osteoporosis, arthritis, and mental health issues. This is somewhat different than the typical practice pattern seen among Ontario chiropractors. [12]
Currently, chiropractic services are provided to the inner city community, 5 d/wk, by 2 chiropractors who are staff members of the DFCM. The clinic is physically integrated with the outpatient physiotherapists and dieticians and in close proximity to most family practice physicians. Community members and hospital staff access our services on referral from their family physicians, through the Positive Care Clinic (HIV/AIDS), or through the employee health unit. The demand is sufficiently high, such that the current waiting period for patients is 4 to 5 weeks to access the services. The chiropractic schedule is full daily, indicating high community demand and use.
As part of our program of care, we collected clinical outcomes at intake and discharge. Standardized instruments (Neck Disability Index, Roland-Morris Low Back Pain Questionnaire, etc) were used to assess the severity of the patients' complaints and their quality of life. Examples from our initial data analysis show clinically significant gains were obtained in patients with neck pain (mean Neck Disability Index change, 6.8/50) and lower back pain (50% obtaining more than the minimal clinically important change on the Roland-Morris Low Back Pain Questionnaire). The percentage of patients whose pain produced moderate to severe limitation of work outside the home dropped from 81% to 65%. Those significantly affected by emotional strain fell from 73% to 59%, and those able to work in the home rose from 60% to 84%.
There was an endorsement of over 90% for “excellent” or “very good” across all parameters on the patient satisfaction survey. We are in the process of preparing this data for publication.
Reducing Burden on Providers and the System
As noted earlier, the issue of wait times for accessing health services is a critical issue both provincially and nationally. Interviews were conducted with physicians and staff over the course of our project to discern the effect of chiropractic inclusion on work loads. Early in the project, staff noticed a reduction in the wait period for patients to access physiotherapy as some patients were opting for the shorter delay to access chiropractic services for their complaints. Our ability to reduce wait times for the physiotherapy services was seen as an additional benefit to integration. Physicians, through interviews, reported significant changes in attitude toward the chiropractic staff, not only in terms of respect for training and expertise but also for the value to patients and reduction of personal physician work-related stress. Examples of responses, in the physician's own words, include:I have only had positive feedback from many of my clients; they have always had some sort of change in their outcome and they have always had some sort of positive thing to say.
We are able to give the patient hope and encouragement and actually I have a lot of patients that it has helped with their pain reduction and certainly has taken the burden off me psychologically a little bit and timewise as well.All respondents (17/40) to a physician satisfaction questionnaire reported that they were highly satisfied with the inclusion of the chiropractic services and felt that they should continue to be provided within the department. In both the interviews and survey feedback, health providers stressed the importance of interprofessional education and collaborative practice as a means to improve the quality of care delivered to inner city patients. The chiropractic hospital-based program reputation has spread, resulting in invitations to present at numerous local, national, and international academic conferences as well as to policy makers at various governmental levels. Both the clinical data and the expanded acceptance by the medical community are proving to be important and persuasive elements in the case to reduce institutionalized policy barriers to the access and use of chiropractic services. We have been able to demonstrate that the provision of chiropractic care enhances the quality of life and improves function of our patients within the inner city.
Health Promotion and Prevention
All patients accessing chiropractic services are educated about healthy lifestyles and prevention of further disease or injury. We offer an interprofessional back education class, quarterly, for patients on the physiotherapy and chiropractic wait lists as well as for patients currently under care. Back class pre- and postsession questionnaires have indicated that the level of knowledge and understanding about healthy lifestyle and prevention of back problems has improved after completion of the class. Similarly, we have seen these same benefits and resultant improved health status at our other two inner city teaching clinics at SHC and AHT.
Sherbourne Health Centre Chiropractic Clinic
The SHC Chiropractic Clinic is located within the SHC, a relatively new and innovative institution that is working toward an integrative model of healthcare. The SHC is committed to providing services to those living in poverty, the majority of which are the vulnerable and at risk, the homeless, and the underhoused. Other groups, which may also have access barriers to basic health care, include mental health patients, a substantial percentage of new immigrants, and a large section of the HIV/AIDS community.
Figure 2 One of the underlying principles of SHC (Figure 2) is to provide quality health care services to those who are living in precarious housing situations or who are without housing. It is often difficult for the underhoused to access the regular health care system. The SHC has developed programs that deliver solutions through such innovations as unscheduled care clinics, during which appointments are not required and ID and health coverage are not needed to access care. Another successful program has been the Sherbourne Health Buses, which were donated by the Rotary Club. These 2 fully equipped vehicles, manned by volunteer nurses and other community volunteers, make regular stops at many of the area shelters to provide basic heath care, blankets, hats, mittens, and even needle exchange to the shelter residents and local street people. Medical services statistics from the SHC in 2005 indicate that over 47000 health care visits were delivered to new immigrants, children, seniors, the lesbian and gay community, and many more clients who come from the diverse communities in the southeast Toronto region.
The SHC has developed various programs to provide health services to the gay, lesbian, bisexual, transgendered, and transsexual communities. Many within this community have a perceived barrier to accessing health care services and may often be discriminated against. A substantial number of our inner city clinic patients live on disability support programs and have very limited financial resources. The focus, vision and core values of the SHC have been advantageous for the chiropractic clinic and have allowed our services to grow in this niche community.
Sensitivity, respect, and providing services in a nonjudgmental and safe environment are extremely important to these populations who have specific health concerns. Over time, we have identified the specific physical health problems that occur in some of these niche populations. The one group that we have had the most experience with is the HIV/AIDS community. CMCC's chiropractic clinic was originally developed in response to a need identified by the HIV community within the southeast Toronto catchment area. As a result of long-term relationship building of the faculty clinicians and interns in the community, the clinic has developed strong ties to local HIV service agencies, such as the AIDS Committee of Toronto and the Toronto People with AIDS Foundation. These agencies counsel people on issues such as housing, disability support, and health. In this role, they identify clients who find themselves at financial risk and who could make use of our services, as our clinic fees are often significantly discounted in order to make care accessible. In addition, the interns at our clinic tour these agencies and familiarize themselves with the available services. We can then refer patients in a reciprocal way, when appropriate. Referral for assistance through their local food bank and free legal and accounting services, is a common occurrence at our clinic.
The SHC has developed a unique program for the health needs of patients at risk in our community. The infirmary has been developed in the center, which will operate 24 h/d, 7 d/wk, and will provide enhanced health outreach services for people who are homeless or underhoused. It will offer a safe and comfortable environment for those who are recovering from a medical condition and have no place to go to adequately recuperate once they have been discharged from one of the downtown hospitals. Referrals will also be encouraged from local shelters, drop in centers, and community organizations. The primary care clinic also plans to expand its hours of operation to a minimum of 12 h/d.
Our experience at the SHC has been one in which trust and collaborative treatment has developed over time. The chiropractic clinic has been in existence longer than the medical clinic and was in fact the first operating health service of the SHC. Physicians have been hired in a progressive fashion as the medical services have grown. As the medical staff learn about and come to understand the chiropractic services available, referrals to our clinic continue to increase.
In Ontario, chiropractic services were delisted from provincial health insurance in December 2004. Before delisting, patients accessing care at the Sherbourne clinic were not required to co-pay for services. The clinic billed only the provincial plan due to the low economic status of most patients. The effect of delisting on the community has been dramatic, as evidenced by the reduction in use after the removal of any provincial payment for treatment. In 2003 to 2004, the clinic assessed approximately 650 new patients and provided more than 12000 treatment sessions. In the past year, with the implementation of a very small copayment (due to government delisting), chiropractic clinic use has reduced to 300 new patients and approximately 8000 subsequent visits. This demonstrates the impact of an economic barrier (even a small one) on the ability of the poor in accessing treatment. The chiropractic clinic at the SHC has worked diligently to remove barriers to accessing services for those at socioeconomic risk. Our partners at the SHC are aware that although we must charge for the chiropractic services, we are not hesitant to reduce our fees according to the patient's needs in order to ensure proper access to care. As noted previously, many of our patients are on disability support programs, other government-assisted programs, and many live in shelters. Those in shelters only pay a nominal fee.
Public health nursing services within the community are the front-line resources that work with patients living in shelters or through drop-in centers for those living on the street. Referrals to the chiropractic clinic directly from nurses have been important for continuity of care. As mentioned previously, the SHC operates 2 health buses. These vehicles regularly travel from the health center out into the community to set locations. This outreaching of services addresses the major concern that many people living in poverty have, which is apprehension and reservation about approaching the larger centers for health services. Patients are often identified and referred by this service. Chiropractic students have found that volunteering on the health buses, along with nurses and other volunteers, is a very rewarding experience.
The physical environment of our health center is one in which medical and nursing services are provided in the same space, whereas chiropractic, naturopathic, acupuncture, and counseling services are provided separately. The chiropractic and naturopathic clinics are physically integrated within the health center. The proximity of services advances our goal of addressing each component of our patient's health. Besides nursing, medicine, and chiropractic care, several other services are available. The chiropractic service has a long-established history of working collaboratively with the counseling services to address chronic health issues.
The types of conditions patients present to the chiropractic clinic with include uncomplicated musculoskeletal conditions such as back pain, neck pain, headaches and peripheral joint strain/sprains typical of chiropractic practice in Ontario. [12] Complicating these common presentations in our inner city clinic are peripheral neuropathies, viral myalgias, Kaposi's sarcoma, lipodystrophy, diabetic neuropathies, HIV/AIDS medication-related side effects (osteopenia), infestation-related dermatological conditions (body lice, bed bugs), and significant mental health issues. The frequency of these types of presentations is unique to the inner city and impoverished community and results in a much more complex clinical presentation and the requirement for close collaboration with the center's other health providers.
Anishnawbe Health Toronto
Anishnawbe Health Toronto is a community health center in downtown Toronto. Anishnawbe Health has articulated its goal as, [13] “AHT not only promotes traditional aboriginal practices but has affirmed and placed them at its core. AHT's model of health care is based on traditional practices and approaches and is reflected in the design of its programs and services.” This aboriginal health care model (AHCM), reflected in AHT, is based on a fundamental philosophic principle: that a person's life is composed of four critical dimensions—physical, mental, emotional, and spiritual. [14] Health is viewed as the harmonious interplay of the effects of each of these dimensions. In the Ojibway language, this is known as “Pimatizwin.” [15] Thus, this health model can be described as “holistic” and, to at least a certain extent, “vitalistic.” Ill health is viewed as dysfunction and imbalance in one, some, or all of these dimensions. Healing is viewed as a process that addresses each of these dimensions and that strives to restore harmony among them.
The AHCM is also culture-based and culturally sensitive. All aspects of the “clinic experience,” from outreach into the community, the atmosphere, and environment of the clinic itself, the interpersonal experience within the clinic, the way in which patients are oriented to the services of the clinic, the range of services, the way services are provided, and others, are grounded in respect for and appreciation of the experience of aboriginal peoples. While each person is certainly viewed uniquely, there are many features of the experience of aboriginal Ontarians, their past history, their socioeconomic narrative, their spiritual practices, their general world view, and their health-related needs that are shared by many; it is these features that are given the utmost attention within the AHCM and which make aboriginal health care centers unique and uniquely qualified to provide appropriate health care to these people.
Figure 3 Chiropractic services have been part of the integrated practice at AHT (Figure 3) since 1996. The CMCC teaching clinic was founded with the humble beginnings of one clinician supervising 3 interns twice a week. This has grown to 7 interns 3 d/wk. Typically, we average approximately 250 new patients per year and more than 3300 subsequent visits in this small yet busy clinical setting.
Chiropractic care has been well received since the beginning of our program. Patients can access care directly, or are referred from allopathic practitioners as well as the traditional elders, healers, and others at the AHT.
Considering the holistic approach, patients have the opportunity to address all aspects of their health care needs within an integrated paradigm. For example, a patient who is stressed at work and has headaches can see the chiropractor for the mechanical headaches, a counselor for the stress at work, and an elder to address the patients past cultural experiences and help reinforce history, tradition, and roots. Patients' clinical charts are shared by all health providers, enabling access to what other services are being provided to the patient as well as enhancing communication through a common paper record. This will be further enhanced once the ongoing work of developing an electronic medical record is completed.
The types of patient problems seen at the Anishnawbe chiropractic clinic include those that are typical of general chiropractic practice such as neck and low back pain, headaches, joint strain/sprain-type injuries, and other postural or mechanical musculoskeletal injuries. Because of the high rates of cardiovascular disease and diabetes within the aboriginal population, we are acutely aware of the need and benefit of an integrated approach for our patients; as such, we are members of the integrated diabetes program offered at the clinic. Other social and societal issues such as poverty, mental health, and substance abuse also present with a frequency higher than that of typical private practice. Our patients come from all walks of life, ranging from university students, professionals, mothers and children, to unemployed and impoverished individuals.
Because of the cost of chiropractic care, it has been difficult for many of our patients to access it in the past. It is interesting to note is that it is sometimes more socially prohibitive (“Am I dressed OK?” “Can I go?”) than it is economically prohibitive. The chiropractic program at AHT is busy, providing 4 to 6 new patients and 150 to 200 treatments per week in our 3-d/wk program. The students are exposed to a real-world clinical setting with challenging cases; their clinical education is greatly enhanced by this program. It truly is an example of “you get back what you give out.” As a group, the attending CMCC clinician and interns have been invited to attend many traditional programs and events. They have participated in a sweat lodge ceremony every year, full moon ceremonies, shaking tent ceremonies, and many more. It is a profound experience. One intern said, “I changed and learned more in the 6 months at AHT than in the last 26 years of my life.”
Being aware of community needs and instilling a desire to give back to the community are important priorities for AHT. Our chiropractic interns are involved in many outreach activities such as the street patrol that picks up homeless people on cold, winter nights and relocates them to shelter housing. Interns complete their 6-month placement with a good understanding of and a keen sensitivity to aboriginal health principles and the complex social and health issues facing an urban aboriginal community.
Conclusion
Over the past decade, the CMCC's external clinics program has enabled access to chiropractic services to thousands of people living in the inner city community and within the urban aboriginal community of Toronto. Our priority is to minimize barriers to accessing chiropractic care, to provide appropriate and effective care, and to promote collaboration with other health practitioners and the community. These clinics increase students' awareness of, sensitivity to, and commitment to being part of the solution to these problems. They go forth from CMCC with a greatly enhanced consciousness as people, as professionals, and as healers. We believe that they are better people for this.
Over the past decade we have seen the significant benefits of enabling access to our services to the poor community in the reduction of pain, improvement in function, and betterment in the quality of life for these complex and disadvantaged communities. There is a paucity of information regarding the health benefits to poor or marginalized communities when there is equitable access to chiropractic services. Further research in this area is necessary.
It is our view that all health care practitioners, including chiropractors, have the responsibility of minimizing the effects of poverty and marginalization on people's health and to become engaged with their local communities to ensure equitable access to health services in an effort to reduce the effects of these negative social and societal determinants of health. In this way only may we contribute to improving the health and wellbeing of our communities.
Practical Applications
Poverty and inequitable access to health care result in poorer health status.
CMCC provides chiropractic treatment in 3 teaching clinics without or with minimal economic barrier to the inner city community of Toronto.
There is high use of chiropractic services when there is no economic barrier to accessing care.
Collaborative practice within interdisciplinary settings has resulted in improved health outcomes for disadvantaged communities.
Chiropractic interns need to understand their role and responsibility in improving the health of the poor and in giving back to the community.
Acknowledgment
The authors wish to thank our local host organizations for supporting chiropractic integration and the local aboriginal and HIV/AIDS communities for their advocacy for equitable health care and efforts towards minimization of stigma and poverty.
References:
World Health Organization [homepage on the Internet].
Geneva: AFRO Division: Healthy Environments in Sustainable Development.
Priority # 1: Poverty and Health [1999] [cited 2 April, 2007].
Available from:
www.afro.who.int/pih/pub/positionpaper.pdf.Assai M, Siddiqi S, Watts S.
Tackling social determinants of health through community based initiatives.
BMJ 2006;333: 854-6.Healthy People 2010: Understanding and Improving Health
U.S. Government Printing Office Web site at http://www.bookstore.gpo.gov/World Health Organization (homepage on the Internet) 2006.
Global burden of disease and risk factors report [cited 2007 April 2].
Available from:www.who.org/ 2002Boon H, Verhoef M, O'Hara D, Findlay B.
From parallel practice to integrative health care: a conceptual framework.
BMC Health Serv Res 2004;4:15.Cassidy JD, Cote P, Carroll LJ, Kristman V.
Incidence and course of low back pain episodes in the general population.
Spine 2005;30:2817-23.Primary health care. A framework that fits [homepage on the Internet].
Ottawa: enhancing interdisciplinary collaboration in primary health care
[cited 2007 March 14]. Available from: www.eicp-acis.ca/Kopansky-Giles D, Tibbles A, Decina P, Goldin J, Zylich S.
Community-based external clinics program at CMCC.
Top Clin Chiropr 2002;9:62-7.Toronto Health Profiles [homepage on the Internet].
Toronto: c1991-2001 community health profiles partnership.
Sociodemographic data [cited 2006 March 14].
Available from: www.torontohealthprofiles.ca/Wasylenski D.
Inner city health.
CMAJ 2001;164:214-5.Glazier R, Badley EM, Gilbert JE, Rothman L.
The nature of increased hospital use in poor neighbourhoods:
findings from a Canadian inner city.
Can J Public Health 2000;91: 268-73.Waalen J, Mior S.
Practice patterns of 692 Ontario chiropractors (2000-2001).
J Can Chiropr Assoc 2005;49:21-31.Anishnawbe Health Toronto [homepage on the Internet]
Toronto: 2007 [cited 14 March 2007]. Available from:
www.aht.ca/Bartlett JG.
Health and well-being for Metis women in Manitoba.
Can J Public Health 2005;(Suppl 1):S22-7.White Bird D.
Foreword from the Assembly of Manitoba Chiefs.
Can J Public Health 2005;(Suppl 1):S5.
Return to INTEGRATED HEALTH CARE
Since 8-21-2023
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |