

Safety of Chiropractic Manipulation of the Cervical Spine:
A Prospective National SurveyThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Spine (Phila Pa 1976). 2007 (Oct 1); 32 (21): 2375–2378 ~ FULL TEXT
Haymo W. Thiel, DC, PhD, Jennifer E. Bolton, PhD, Sharon Docherty, PhD, and Jane C. Portlock, PhD
Department of Research and Professional Development,
Anglo-European College of Chiropractic,
Bournemouth, United Kingdom.
hthiel@aecc.ac.uk
STUDY DESIGN: Prospective national survey.
OBJECTIVE: To estimate the risk of serious and relatively minor adverse events following chiropractic manipulation of the cervical spine by a sample of U.K. chiropractors.
SUMMARY OF BACKGROUND DATA: The risk of a serious adverse event following chiropractic manipulation of the cervical spine is largely unknown. Estimates range from 1 in 200,000 to 1 in several million cervical spine manipulations. METHODS: We studied treatment outcomes obtained from 19,722 patients. Manipulation was defined as the application of a high-velocity/low-amplitude or mechanically assisted thrust to the cervical spine. Serious adverse events, defined as "referred to hospital A&E and/or severe onset/worsening of symptoms immediately after treatment and/or resulted in persistent or significant disability/incapacity," and minor adverse events reported by patients as a worsening of presenting symptoms or onset of new symptoms, were recorded immediately, and up to 7 days, after treatment.
RESULTS: Data were obtained from 28,807 treatment consultations and 50,276 cervical spine manipulations. There were no reports of serious adverse events. This translates to an estimated risk of a serious adverse event of, at worse approximately 1 per 10,000 treatment consultations immediately after cervical spine manipulation, approximately 2 per 10,000 treatment consultations up to 7 days after treatment and approximately 6 per 100,000 cervical spine manipulations. Minor side effects with a possible neurologic involvement were more common. The highest risk immediately after treatment was fainting/dizziness/light-headedness in, at worse approximately 16 per 1000 treatment consultations. Up to 7 days after treatment, these risks were headache in, at worse approximately 4 per 100, numbness/tingling in upper limbs in, at worse approximately 15 per 1000 and fainting/dizziness/light-headedness in, at worse approximately 13 per 1000 treatment consultations.
There are more articles like this @ our
STROKE AND CHIROPRACTIC PageCONCLUSION: Although minor side effects following cervical spine manipulation were relatively common, the risk of a serious adverse event, immediately or up to 7 days after treatment, was low to very low.
From the FULL TEXT Article:
Introduction
Although it is generally assumed that serious complications following spinal manipulative therapy of the cervical spine, including neurologic deficit and stroke, are relatively uncommon, their exact incidence is unknown. Estimates vary between 1 serious adverse event in 200,000 manipulative neck treatments [1] to 1 in several million, [2] and 1 in 100,000 persons. [3] Most of these estimates come from case reports and retrospective studies, or from survey and medical claims data. In contrast to serious adverse events, relatively minor side effects of cervical spinal manipulation, such as neck pain, stiffness and soreness, headache, and tiredness are common in clinical practice. [4]
It is the risk, however, of serious adverse events following cervical spine manipulation that is of most concern, not only for patients and chiropractors, but also for general practitioners and hospital specialists considering referring patients for chiropractic treatment. Given the increasing popularity of complementary medicine, [5] including chiropractic, and the potential consequences of a serious adverse event, it is crucial that more evidence is available to inform clinicians and patients of the size of the risk. This is not only to balance any potential benefits but also to counteract any irrational condemnation of the treatment.
This study was therefore conducted to provide an estimate of the risk of adverse events following chiropractic manipulation of the cervical spine in a sample of U.K. chiropractors. As far as we are aware, it is the first, largescale prospective study of its kind specifically designed to record serious and minor adverse events following chiropractic manipulation of the neck.
Materials and Methods
All registered chiropractors who were members of the British and Scottish Chiropractic Associations (1,183 at the time) were invited to participate. Standardized forms, which had previously undergone peer-review and pilot testing, recorded details on treatment and outcomes in patients 16 years of age and older receiving chiropractic treatment in which at least 1 cervical spine manipulation was administered. Manipulation was defined as a high-velocity/low-amplitude or mechanically assisted thrust to the cervical spine.
Data were collected from June 2004 to March 2005, in which individual chiropractors’ defined 6-week recording periods were staggered to facilitate data collection. The 377 participating chiropractors were asked to provide details of themselves (name, age, gender and years in practice). All 19,722 patients recruited to the study gave informed written consent.
Chiropractors recorded details during their defined 6-week period on either 100 consecutive treatment consultations or consecutive treatment consultations to the end of this period, whichever was the sooner. The primary sampling units were the: 1) treatment consultation, 2) follow-up period (up to 7 days after the consultation) and 3) cervical spine manipulation. Event rates are therefore reported for these units and not for individual patients. For the treatment consultation, details were recorded at the end of the treatment session by the chiropractor, completing details on the cervical spine manipulation(s), asking the patient about any worsening of presenting symptoms and onset of any new symptoms, and recording any adverse event immediately following treatment. For an adverse event, the chiropractor was asked to indicate whether it was considered to be a significant (serious) event, defined as “referred to hospital A&E and/or severe onset/worsening of symptoms immediately after treatment and/or resulted in persistent or significant disability/incapacity.” [6] Any event defined in this way was reported on a separate form. The follow-up period was defined as the intervening period between the treatment consultation and the patient returning, if appropriate, for their next session of treatment, provided this occurred within the 6-week recording period.
Details were recorded in a similar manner as those for a treatment consultation, but in this case at the beginning of the return treatment session. The patient was asked about any worsening of existing symptoms and onset of any new symptoms in the intervening (follow-up) period (from “later that day” to 7 days after the treatment consultation). The chiropractor recorded any adverse event that had occurred in the follow-up period and whether it was considered to be significant using the same criteria as before.
Once all the data were received, patients were identified in cases where they had failed to return for their next treatment, even though this had been scheduled within the 6-week recording period. This group represented the only possibility of a failure to record serious adverse events, if they had occurred, and so risk compromising the event rate for the follow-up period. Members of the research team first contacted the patient’s chiropractor to determine whether an adverse event had occurred. If this contact was unsuccessful, the patient was contacted by phone. As a last resort, and failing all other means of determining whether a serious adverse event had occurred, the patient’s general practitioner was contacted to establish if any problems had occurred that could possibly be related to chiropractic treatment.
SPSS, version 13.0, was used to analyze the data. To estimate risk in cases where no occurrence of an adverse event occurs, Hanley’s “rule of three” was used. [7] This states that if none of n patients shows the event, then it can be assumed with 95% confidence that the chance of this event is, at worst, 3 in n (i.e., 3/n). It is generally accepted that treatment associated events occurring at a rate of 1 in 10,000 to 100,000 can be categorized as very low risk. [8] Again using the “rule of three,” to be confident at the 95% level that a serious adverse event occurs in n treatments where no serious adverse event has occurred, a survey sample size needs to be 3n. [7, 9] Therefore, a sample size of 50,000 cervical spine manipulative interventions was sought to give a frequency of 1 serious adverse event in approximately 17,000 interventions. Information from a pilot study, which was carried out to determine the feasibility of the main study and including 498 patients, indicated this required approximately 30,000 treatment consultations. This study received an ethical opinion from the Eastern Multicenter Research Ethics Council (United Kingdom) and ethical approval from the Faculty of Science Ethics Committee University of Portsmouth (United Kingdom).
Results
A total of 377 chiropractors (31.9% of the target population) participated in the study; 59.7% were male, 65.8% were between 30 and 49 years of age, and 67.4% had been in practice for 5 or more years. In total, data were recorded from 19,722 patients (60.3% female; mean ± SD age, 47.3 ± 14.01 years; age range, 16–100 years).
In terms of the sampling units, data were recorded from 50,276 cervical manipulations and from 28,109 treatment consultations. There were an additional 698 treatment consultations of those patients who had failed to return for their next treatment even though it was scheduled within the 6-week recording period. Of these, contact with the chiropractor, the patient or the general practitioner ascertained that, in 285 cases no serious adverse event had occurred. This meant that, in 413 treatment consultations, or 1.4% of the total number of treatment consultations (28,807), any adverse event(s) occurring in the follow-up period would not have been recorded. Of the 28,807 treatment consultations, 15,520 completed an intervening period by recording details at the next treatment session.
No significant adverse event was reported by the chiropractors using the definition criteria and no separate forms were received. Using the “rule of three,” [7] this translates to a 95% confidence of a serious adverse event occurring either immediately or up to 7 days after a typical chiropractic treatment involving at least 1 cervical manipulation of, at worse, 1 in 9,600 (upper limit 95% confidence interval [CI], 0.01%) and 1 in 5,200 (upper limit 95% CI, 0.02%), respectively. Using the manipulative procedure as the unit of analysis, this translates to a 95% confidence level of a serious adverse event following a single cervical spine manipulation of, at worse, 1 in 16,800 (upper limit 95% CI, 0.006%).

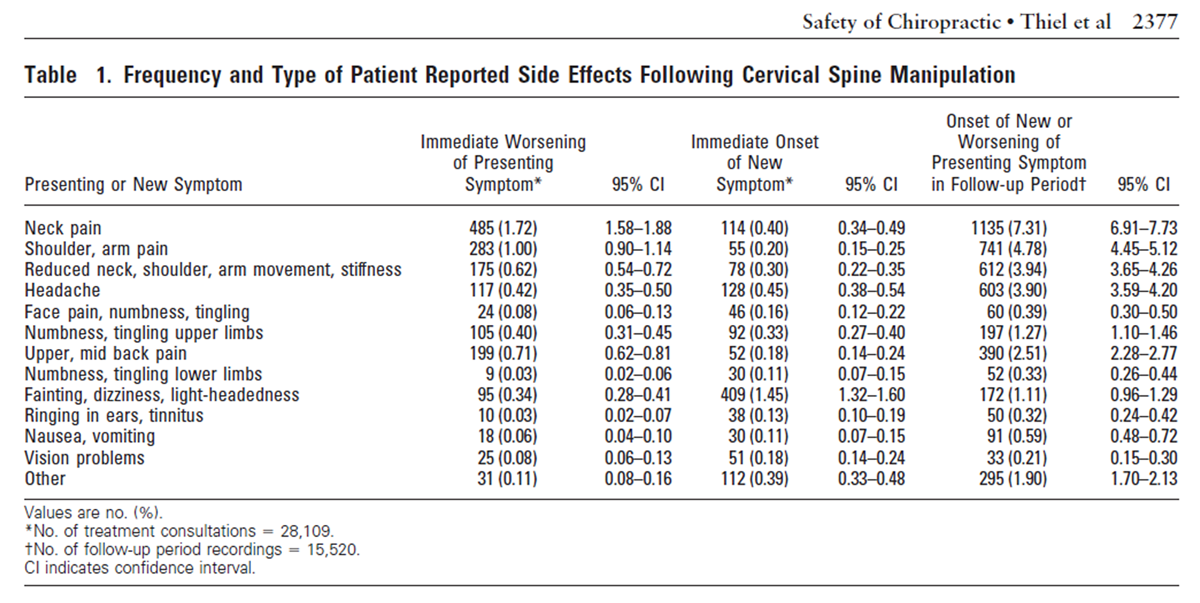
Table 1 In addition to reporting by the chiropractors, the patients were asked to report any worsening of presenting symptoms, or onset of any new symptoms following cervical spine manipulative treatment, either immediately or in the follow-up period (Table 1). Patients were allowed to report on any number of side effects as they occurred. As expected, immediate worsening of presenting symptoms was predominately musculoskeletal in nature, with a worsening of neck pain as the most common symptom (1.7% of treatments). Immediate onset of new symptoms, on the other hand, accentuated nonmusculoskeletal symptoms, such as headache and fainting/ dizziness/light-headedness. The most common of these, fainting/dizziness/light-headedness, occurred in 1.5% of cases. In the follow-up period, the onset of new or worsening of presenting symptoms demonstrated that discomfort in the area of the manipulation (neck pain) was the most common, occurring in 7.3% of cases followed by other musculoskeletal symptoms of shoulder/arm pain (4.8%) and reduced movement in the neck and upper limb (3.9%). Symptoms that may have indicated a neurologic involvement, such as headache, numbness/ tingling in upper limbs, and fainting/dizziness/lightheadedness, in the period up to 7 days following cervical spine manipulation, occurred in 3.9%, 1.3% and 1.1% of cases, respectively.
Discussion
This study provides further evidence of the risk of a serious adverse event following chiropractic manipulation of the neck. This risk, reported by a sample of U.K. chiropractors, ranged from, at worse (upper limit 95% CI) ~ 1 per 10,000 treatment consultations immediately after cervical manipulation, ~ 2 per 10,000 treatment consultations up to 7 days after treatment, and ~ 6 per 100,000 cervical spine manipulations. In contrast, patient- reported risks of relatively minor side effects were considerably higher. Besides the expected worsening or onset of musculoskeletal symptoms after treatment, the largest risk of side effects with a possible neurologic involvement immediately after treatment was fainting/ dizziness/light-headedness in, at worse (upper limit 95% CI) ~ 16 per 1000 treatment consultations. Up to 7 days after treatment, the risks were headache in, at worse ~ 4 per 100, numbness/tingling in upper limbs in, at worse ~ 15 per 1000, and fainting/dizziness/light-headedness in, at worse ~ 13 per 1000 treatment consultations.
Safety of treatment interventions is best established with prospective surveys,10 and this study is unique in that it is the only prospective survey on such a large scale specifically estimating serious adverse events following cervical spine manipulation. A significant proportion of chiropractors in the profession in the United Kingdom took part, and over 19,000 patients agreed to participate with very few patients eligible but not willing to do so. Despite the large number of treatment consultations (28,807), the loss to follow-up was low (1.4%).
There are a number of limitations of the study. As a large-scale study, it remains the case that, given the assumed rarity of serious adverse events following neck manipulation, an even larger study would have provided a more accurate estimate of the associated risks. However, this must be balanced by the feasibility and practicalities involved in conducting a study of this magnitude. All adverse events, which are per treatment consultations or procedures and not per patient, were recorded whether causally related to cervical spine manipulation or not. Similarly, patient-reported side effects could have been a description of preexisting symptoms or the development of new symptoms, and as such not incidental to the treatment. The validity of the study obviously relies heavily on the honesty of the chiropractors. We have no way of knowing whether chiropractors recruited treatment consultations in a consecutive manner, as they were asked to do, or in some other manner, which may have introduced bias. There is also the very real possibility of underreporting by the chiropractors, particularly since they did not report anonymously. This could have been on purpose, perhaps through fear of recrimination, or else unwittingly by failing to record the information correctly.
Similarly, patients may have been reluctant to report negative reactions in a face-to-face situation with their chiropractors. Other studies have encountered this same limitation, for example, prospective surveys investigating adverse events following acupuncture. 10,11 Unfortunately, in any surveillance exercise reporting adverse events by the practitioners themselves, underreporting remains a potential source of bias. At the time of the study, approximately 32% of the profession participated. Although this is a significant proportion, there still remains the possibility of respondent bias given that these were practitioners who volunteered to participate. Finally, it is possible that a serious adverse event(s) did occur in those treatment consultations lost to follow-up (1.4%). Since the object of this study, among others, was to estimate the incidence of rare adverse events, this small loss to follow-up is a proportionately greater limitation than it would be in studies estimating the incidence of common complications.
To help understand level of risk, numerical risk estimates have been expressed in literal terms.8 Using these definitions, the serious adverse events estimated in this study can be categorized as low to very low. The patientreported side effects of cervical spinal manipulation obtained in this study are lower than those previously reported, 4 which may be attributable in part to differences in sample sizes and reporting mechanisms.
The risk rates described in this study compare favorably to those linked to drugs routinely prescribed for musculoskeletal conditions in general practice.12 The risks reported here are also lower than those reported for acupuncture, [10, 11, 13] which were described as a “very safe intervention in the hands of a competent practitioner.” [14]
Given the large number of cervical spine manipulations administered by chiropractors, safety of this intervention is a public health issue. This study is the first large-scale prospective survey of cervical spine manipulations specifically recording adverse events following treatment. Although minor side effects were found to be relatively common, the risk of a serious adverse event, immediately and up to 7 days after treatment, was estimated to be low to very low in these consultations. On this basis, this survey provides evidence that cervical spine manipulation is a relatively safe procedure when administered by registered U.K. chiropractors.
Key Points
Manipulation of the cervical spine is a commonly used procedure in chiropractic treatment.
There is considerable speculation on the risk of serious adverse events, leaving patients and clinicians uncertain about the safety of chiropractic treatment.
Based on treatment outcomes obtained from 19,722 patients, the risk of a serious adverse event following cervical spine manipulation was estimated to be low to very low; risks of minor side effects, on the other hand, were relatively common.
Acknowledgement
The authors thank members of the British and Scottish Chiropractic Associations, and their patients, for their contribution to the pilot study and to the main study as well as Dr. David Brown, Dr. George Carruthers, Prof. Edzard Ernst, Dr. Kim Humphreys, Dr. Hugh Hurst, Dr. Sally Kilburn, Prof. Niels Grunnet-Nilsson, Dr. Dean Sluce, Prof. Peter Thomas and Dr. Adrian White who advised us in the peer-review stage of this study.
REFERENCES:
Michaeli A.
Reported occurrence and nature of complications following manipulative physiotherapy in South Africa.
Aust Physiother 1993;39: 309–15.Haldeman S, Carey P, Townsend M, Papadopoulos C.
Arterial Dissections Following Cervical Manipulation: The Chiropractic Experience
Canadian Medical Association Journal (CMAJ) 2001 2001 (Oct 2); 165: 905–906Rothwell DM, Bondy SJ, Williams JI.
Chiropractic Manipulation and Stroke:
A Population-based Case-control Study
Stroke 2001 (May); 32 (5): 1054-1060Hurwitz EL, Morgenstern H, Vassilaki M, et al.
Adverse reactions to chiropractic treatment and their effects on satisfaction
and clinical outcomes among patients enrolled in the UCLA Neck Pain Study.
J Manipulative Physiol Ther 2004;27:16–25.Ernst E.
Prevalence of use of complementary/alternative medicine: a systematic review.
Bull World Health Organ 2000;78:252–7.Edwards IR, Aronson JK.
Adverse drug reactions: definitions, diagnosis, and management.
Lancet 2000;356:1255–9.Hanley JA, Lippman-Hand A.
If nothing goes wrong, is everything all right?
JAMA 1983;249:1743–5.Calman KC.
Cancer: science and society and the communication of risk.
BMJ 1996;313:799–802.Ho AM, Dion PW, Karmakar MK, et al.
Estimating with confidence the risk of rare adverse events, including those with observed rates of zero.
Reg Anesth Pain Med 2002;27:207–10.White A, Hayhoe S, Hart A, et al.
Adverse events following acupuncture: prospective survey of 32 000 consultations with doctors and physiotherapists.
BMJ 2001;323:485–6.MacPherson H, Thomas K, Walters S, et al.
The York Acupuncture Safety Study: prospective survey of 34,000 treatments by traditional acupuncturists.
BMJ 2001;323:486–7.Trammer MR, Moore RA, Reynolds DJM, et al.
Quantitative estimation of rare adverse events which follow a biological progression:
a new model applied to chronic NSAID use.
Pain 2000;85:169–82.MacPherson H, Scullion A, Thomas K, et al.
Patient reports of adverse events associated with acupuncture treatment: a prospective national survey.
Qual Saf Health Care 2004;13:349–55.Vincent C.
The safety of acupuncture.
BMJ 2001;323:467–8.
Return to STROKE AND CHIROPRACTIC
Since 11-07-2007
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |