FROM:
The Rubicon Group ~ FULL TEXT
 Click to increase size
Click to increase size
The term ‘subluxation’ has been used by the chiropractic profession for over a century. [1, 2] It is an important element of chiropractic practice, embedded in legislation and regulation, and its clinical implications have been, and continue to be scientifically explored. [2, 3]
The term subluxation, as used by chiropractors, is a researchable concept that is important to health and health care delivery. [1, 2, 4] The need to properly define this entity has been widely recognized as a high priority within the profession, as evidenced by the number of groups and organizations who have offered definitions of subluxation. [1, 2, 5–10]
Many of the past definitions do not provide a testable definition of chiropractic subluxation. [11] Some do not reflect the current research that supports a neurologically-centered model of subluxation. [2] The Rubicon Group (TRG) has utilized the current available scientific evidence to define the chiropractic subluxation.
Contemporary neurophysiological language and concepts, based on current scientific publications on the topic, have been used. As this definition is subject to ongoing scientific exploration that is likely to lead to new findings and understandings, modifications may be anticipated. However, this definition reflects what is currently known, and it is congruent with current neurophysiological scientific understanding
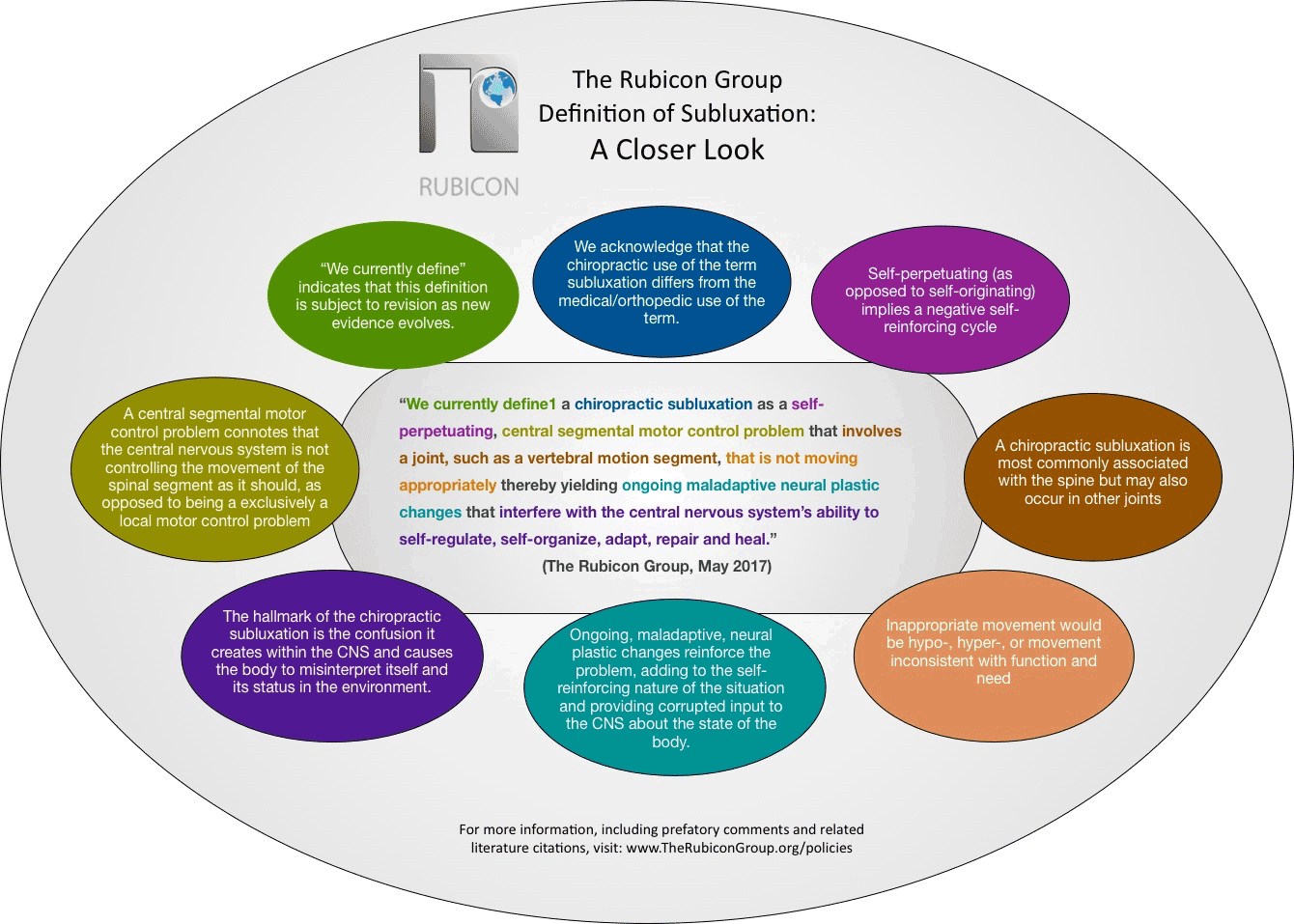
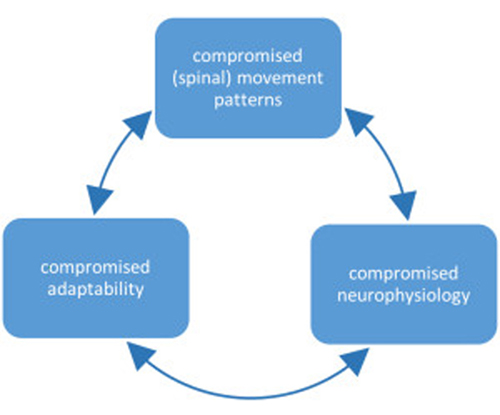
“We currently define a chiropractic subluxation as a self-perpetuating, central segmental motor control problem that involves a joint, such as a vertebral motion segment, that is not moving appropriately, resulting in ongoing maladaptive neural plastic changes that interfere with the central nervous system’s ability to self-regulate, self-organize, adapt, repair and heal.”
(The Rubicon Group, May 2017.)
There are three key elements, namely:
A chiropractic subluxation often relates to the spine and its connecting structures. [1] Chiropractic subluxation assessment generally involves evaluating the pathophysiological consequences of the central segmental motor control problem; [4, 12] these may include pain, asymmetry, biomechanical or postural changes (such as changes in relative range of intervertebral motion), changes in tissue temperature, texture and/or tone, and other findings that can be identified using special tests. [12] Once identified, subluxations are corrected using a variety of techniques including high velocity low amplitude chiropractic adjustments, instrument assisted adjustments, and lower force manual techniques and approaches. [13]
A growing body of scientific evidence has demonstrated that spinal function impacts central neural function in multiple ways, [3, 4, 14–19] and that improving spinal function has an impact on clinical outcomes. [20–24] Scientists have known for several decades that neurons continuously adapt in structure and function in response to our ever-changing environment. [25–27] This ability to adapt is known as ‘neural plasticity’, [27] and it is now well understood that the central nervous system can reorganize in response to altered input. [28–35]
Examples of increased sensory input that can lead to neural plastic changes include repetitive muscular activity [29, 36–41] such as typing or playing the piano, or repeated tactile sensory input such as occurs with blind Braille readers. [42] Similar central nervous system change or reorganization may take place due to a decrease in behavior or activity. [32, 43–49] Thus the concept, that alterations in paraspinal muscle function due to abnormal spinal movement patterns are capable of changing central neural function is totally congruent with current neuroscience understanding, as well as current scientific findings. [3, 4, 14–19]
[1] In the scientific literature, this can be known as hyperafferentation. Hyper–meaning increased, and afferentation – meaning the afferent nerves, which are the ones that go to the brain with information.
[2] In the scientific literature, this is often called deafferentation.
References:
Hart, J., 2016.
Analysis and Adjustment of Vertebral Subluxation as a Separate and Distinct Identity
for the Chiropractic Profession: A Commentary
Journal of Chiropractic Humanities 2016 (Oct 25); 23 (1): 46–52
Rosner, A.L., 2016.
Chiropractic Identity: A Neurological, Professional, and Political Assessment
Journal of Chiropractic Humanities 2016 (Dec); 23 (1): 35–45
Haavik, H and Murphy, B.
The Role of Spinal Manipulation in Addressing Disordered Sensorimotor Integration and
Altered Motor Control
J Electromyogr Kinesiol. 2012 (Oct); 22 (5): 768–776
Henderson, C. N.
The Basis for Spinal Manipulation: Chiropractic Perspective of Indications and Theory
Journal of Electromyography and Kinesiology 2012 (Oct); 22 (5): 632–642
Stephenson RW.
Chiropractic Textbook.
Davenport, Iowa: Palmer School of Chiropractic; 1927.
Practice Guidelines for Straight Chiropractic.
Paper presented at: Wyndham Conference; May 13–17, 1992, 1992;
Chandler, Arizona, USA.
Association of Chiropractic Colleges.
The Association of Chiropractic Colleges Position Paper # 1
ICA Rev. 1996;November/December.
C Lantz
The Vertebral Subluxation Complex PART 1:
An Introduction to the Model and Kinesiological Component
Chiropractic Research Journal 1989; 1 (3): 23-36
Gatterman MI, Hansen DT.
Development of chiropractic nomenclature through consensus.
J Manipulative Physiol Ther. Jun 1994;17(5):302–309.
Leach RA.
The chiropractic theories: a textbook of scientific research. 4th ed.
Baltimore: Lippincott Williams and Wilkins; 2004.
Owens E.
Chiropractic subluxation assessment: What the research tells us
J Can Chiro Assoc. 2002;46(4):215–220.
Triano J, Budgell B, Bagnulo A, Roffey B, Bergmann T, Cooperstein R.
Review of Methods Used by Chiropractors to Determine
the Site for Applying Manipulation
Chiropractic & Manual Therapies 2013 (Oct 21); 21 (1): 36
Cooperstein R, Gleberzon B.
Technique systems in chiropractic.
New York: Churchill-Livingstone; 2004.
Uthaikhup S, Jull G, Sungkarat S, Treleaven J.
The Influence of Neck Pain on Sensorimotor Function in the Elderly
Arch Gerontol Geriatr. 2012 (Nov); 55 (3): 667–672
Haavik, H and Murphy, B.
Subclinical Neck Pain and the Effects of Cervical Manipulation on Elbow Joint Position Sense
J Manipulative Physiol Ther. 2011 (Feb); 34 (2): 88–97
Pickar JG, Bolton PS.
Spinal Manipulative Therapy and Somatosensory Activation
J Electromyogr Kinesiol. 2012 (Oct); 22 (5): 785–794
Pickar JG.
Neurophysiological Effects of Spinal Manipulation
Spine J (N American Spine Society) 2002 (Sep); 2 (5): 357–371
Treleaven J.
Sensorimotor disturbances in neck disorders affecting postural stability,
head and eye movement control.
Man Ther. 2008;13(1):2–11.
Branstrom H, Malmgren-Olsson EB, Barnekow-Bergkvist M.
Balance performance in patients with Whiplash Associated Disorders and Patients
with prolonged Musculoskeletal Disorders.
Adv Physiother. 2001;3:120–127.
Martinez-Segura R, Fernandez-de-las-Penas C, Ruiz-Saez M.
Immediate Effects on Neck Pain and Active Range of Motion After a Single
Cervical High-velocity Low-amplitude Manipulation in Subjects Presenting
with Mechanical Neck Pain: A Randomized Controlled Trial
J Manipulative Physiol Ther 2006 (Sep); 29 (7): 511–517
Ozkara GO, Ozgen M, Ozkara E, Armagan O, Arslantas A, Atasoy MA.
Effectiveness of physical therapy and rehabilitation programs starting immediately
after lumbar disc surgery.
Turk Neurosurg. 2015;25(3):372–379.
Hawk C, Knorsa R, Lisi A, Ferrance RJ, Evans MW.
Chiropractic Care for Nonmusculoskeletal Conditions: A Systematic Review
With Implications For Whole Systems Research
J Altern Complement Med. 2007 (Jun); 13 (5): 491–512
Ruddock JK, Sallis H, Ness A, Perry RE.
Spinal Manipulation Vs Sham Manipulation for Nonspecific Low Back Pain:
A Systematic Review and Meta-analysis.
J Chiropr Med. Sep 2016;15(3):165–183.
Holt, KR, Haavik, H, Lee, ACL, Murphy, B, and Elley, CR.
Effectiveness of Chiropractic Care to Improve Sensorimotor Function Associated With Falls Risk
in Older People: A Randomized Controlled Trial
J Manipulative Physiol Ther. 2016 (May); (39) 4: 267–278
Kandel ER, Schwartz JH, Jessell TM.
Principles of Neural Science. 4 ed:
McGraw-Hill Companies; 2000.
Brown TH, Kairiss EW, Keenan CL.
Hebbian synapses: biophysical mechanisms and algorithms.
Annu Rev Neurosci. 1990;13:475–511.
Cooke SF, Bliss TV.
Plasticity in the human central nervous system Brain.
2006;129(Pt 7):1659–1673.
Fratello F, Veniero D, Curcio G, et al.
Modulation of corticospinal excitability by paired associative stimulation:
reproducibility of effects and intraindividual reliability.
Clin Neurophysiol. Dec 2006;117(12):2667–2674.
Tyc F, Boyadjian A, Devanne H.
Motor cortex plasticity induced by extensive training revealed by transcranial
magnetic stimulation in human.
Eur J Neurosci. Jan 2005;21(1):259–266.
Sessle BJ, Yao D, Nishiura H, et al.
Properties and plasticity of the primate somatosensory and motor cortex
related to orofacial sensorimotor function.
Clin Exp Pharmacol Physiol. Jan-Feb 2005;32(1–2):109–114.
Kaelin-Lang A, Sawaki L, Cohen LG.
Role of Voluntary Drive in Encoding an Elementary Motor Memory.
J Neurophysiol. February 1, 2005 2005;93(2):1099–1103.
Weiss T, Miltner WH, Liepert J, Meissner W, Taub E.
Rapid functional plasticity in the primary somatomotor cortex and perceptual
changes after nerve block.
Eur J Neurosci. Dec 2004;20(12):3413–3423.
Tinazzi M, Valeriani M, Moretto G, et al.
Plastic interactions between hand and face cortical representations in
patients with trigeminal neuralgia: a somatosensory-evoked potentials study.
Neuroscience. 2004;127(3):769–776.
Sanes JN, Donoghue JP.
Plasticity and primary motor cortex.
Annu Rev Neurosci. 2000;23:393–415.
Liepert J, Bauder H, Wolfgang HR, Miltner WH, Taub E, Weiller C.
Treatment-induced cortical reorganization after stroke in humans.
Stroke. Jun 2000;31(6):1210–1216.
Yahagi S, Takeda Y, Ni Z, et al.
Modulations of input-output properties of corticospinal tract neurons by
repetitive dynamic index finger abductions.
Exp Br Res. 2005/02// 2005;161(2):255–264.
Renner CI, Schubert M, Hummelsheim H.
Selective effect of repetitive hand movements on intracortical excitability.
Muscle Nerve. Mar 2005;31(3):314–320.
Schubert M, Kretzschmar E, Waldmann G, Hummelsheim H.
Influence of repetitive hand movements on intracortical inhibition.
Muscle Nerve. Jun 2004;29(6):804–811.
Byl NN, Merzenich MM, Cheung S, Bedenbaugh P, Nagarajan SS, Jenkins WM.
A primate model for studying focal dystonia and repetitive strain injury:
effects on the primary somatosensory cortex.
Phys Ther. Mar 1997;77(3):269–284.
Byl NN, Melnick M.
The neural consequences of repetition: clinical implications of a learning hypothesis.
J Hand Ther. Apr-Jun 1997;10(2):160–174.
Nudo R, Milliken G, Jenkins W, Merzenich M.
Use-dependent alterations of movement representations in primary motor cortex
of adult squirrel monkeys.
J. Neurosci. January 15, 1996 1996;16(2):785–807.
Pascual-Leone A, Torres F.
Plasticity of the sensorimotor cortex representation of the
reading finger in Braille readers.
Brain. 1993;116(Pt 1):39–52.
Tinazzi M, Rosso T, Zanette G, Fiaschi A, Aglioti SM.
Rapid modulation of cortical proprioceptive activity induced by transient
cutaneous deafferentation: neurophysiological evidence of short-term
plasticity across different somatosensory modalities in humans.
Eur J Neurosci. 2003;18(11):3053–3060.
Murphy BA, Haavik Taylor H, Wilson SA, Knight JA, Mathers KM, Schug S.
Changes in median nerve somatosensory transmission and motor output following
transient deafferentation of the radial nerve in humans.
Clin Neurophysiol. 2003;114(8):1477–1488.
Murphy B, Dawson N.
The effects of repetitive contractions and ischemia on the ability to discriminate
intramuscular sensation.
Somatosens Mot Res. 2002;19(3):191–197.
Hallett M, Chen R, Ziemann U, Cohen LG.
Reorganization in motor cortex in amputees and in normal volunteers after
ischemic limb deafferentation.
Electroencephalogr Clin Neurophysiol Suppl. 1999;51:183–187.
Tinazzi M, Zanette G, Polo A, et al.
Transient deafferentation in humans induces rapid modulation of primary sensory cortex
not associated with subcortical changes: a somatosensory evoked potential study.
Neurosci Lett. 1997;223(1):21–24.
Brasil-Neto JP, Valls-Sole J, Pascual-Leone A, et al.
Rapid modulation of human cortical motor outputs following ischaemic nerve block.
Brain. 1993;116(Pt 3):511–525.
Brasil-Neto JP, Cohen LG, Pascual-Leone A, Jabir FK, Wall RT, Hallett M.
Rapid reversible modulation of human motor outputs after transient deafferentation
of the forearm: a study with transcranial magnetic stimulation.
Neurology. 1992;42(7):1302–1306.

Return to SUBLUXATION
Since 3–10–2018
|



