

Agents of Change: How Do Complementary and Alternative
Medicine Providers Play a Role in Health Behavior Change?This section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Altern Ther Health Med. 2011 (Jan); 17 (1): 22–30 ~ FULL TEXT
Pamela A. Williams-Piehota, PhD; Fuschia M. Sirois, PhD; Carla M. Bann, PhD; Karen B. Isenberg, MPH; Edith G. Walsh, PhD
RTI International,
Research Triangle Park,
North Carolina, USA.
ppiehota@rti.org

BACKGROUND: Recent investigations indicate that complementary and alternative medicine (CAM) use may be conducive to health behavior change.
OBJECTIVE: The goal of this study was to investigate how this change occurs.
METHODS: Using Social Cognitive Theory (SCT) and Self-determination Theory (SDT) as guiding frameworks, we surveyed a convenience sample of 216 CAM consumers abouttheir CAM therapy and iors and conducted focus groups with 36 CAM consumers.
RESULTS: Consumers reported encouragement from providers and improved energy resulting from treatments as reasons for making health behavior changes. Multivariate analysis showed that increased odds of self-reported dietary change were significantly associated with increasing body awareness as a result of therapy, endorsing the statement that sustained improvement for their health conditions required self-care, using an acupuncturist, and being 44 years or younger. Comparable results were found for exercise change, except using an acupuncturist was a significant negative predictor and age was not significant. Focus group findings echoed these themes.
CONCLUSION: This initial investigation into how CAM providers may play a role in health behavior change suggests that provider support, increased responsibility for one's health, and the CAM treatments themselves contribute to behavior change, although additional research in this area is warranted.
From the FULL TEXT Article:
Background
The importance of healthy dietary and physical activity behaviors for primary and secondary prevention of disease is well documented. Physical inactivity and unhealthy diet are major contributors to the obesity epidemic in the United States and worldwide, [1] with more than a quarter of US adults not engaging in any leisure-time physical activity and less than a quarter eating the recommended daily amount of fruits and vegetables. [2] Despite the importance of these behaviors for promoting and maintaining health, getting people to make positive health behavior changes remains a challenge.
Emerging research indicates that the use of complementary and alternative medicine (CAM) may be one possible avenue for changing health behaviors. The desire to maintain and improve health and physical fitness levels is an often-reported reason for using CAM. [3, 4] CAM use is associated with the practice of positive health behaviors [5, 6] and may be conducive to health behavior change. [7] However, how this change occurs — through the support of CAM providers, as part of increased responsibility for one’s health, or facilitated by the outcomes of CAM therapies — has not been investigated previously. This study explores how CAM providers play a role in health behavior change.
Complementary and Alternative Medicine Use and Health Behaviors
A growing literature has documented the links between CAM use and positive health behaviors. Aside from making more frequent use of health care services, [8–11] CAM consumers also engage in a variety of health-promoting behaviors to a greater extent than non–CAM consumers. For example, CAM consumers are more likely to get vaccinations [60] and to use a variety of preventive health services, [12, 13] including cancer screening. [14] Associations between CAM use and other positive health behaviors, such as a healthy diet and physical activity, have been noted in national surveys from the United States, [5, 15] Canada, [16] Germany, [17] and Australia. [18] Moreover, CAM use has been linked to practicing fewer risky health behaviors such as smoking and consuming alcohol. [5, 19]
Indeed, the portrait of CAM consumers as health-minded and motivated to take an active role in their health is well-established in the CAM literature. [9, 20] Whether the desire for a healthy lifestyle is a product or precursor of CAM use is an ongoing question that may be best resolved with longitudinal research. [21, 22] Nonetheless, current research suggests that CAM providers may play a role in their clients’ health behavior changes. In one qualitative investigation, patients reported that the relationship with their CAM providers changed their perceptions of health and caused them to take greater responsibility for their health, which in turn caused them to make health behavior changes. [23] Similarly, in a qualitative study, men with prostate cancer reported making significant lifestyle changes to improve their health as a result of their CAM use. [7]
In another study, 61% of acupuncture patients reported making some sort of lifestyle change since beginning therapies. [24] A large qualitative investigation of US military veterans using CAM noted that many had made significant dietary changes since starting CAM use. [4] Similarly, a survey of network spinal analysis clients found that use of this holistic form of chiropractic care was linked to a variety of health behavior changes, including increases in physical activity, improvements in diet, and reductions in risky health behaviors. [25] More compelling evidence of the potential effects of CAM use on health behavior changes comes from a recent prospective study of shiatsu clients. Three quarters of clients received advice from their therapists regarding diet, exercise, and other health-promoting changes, and 6 months later, the majority reported making lifestyle changes as a result of their shiatsu treatment. [26]
Explaining Health Behavior Change via complementary
and alternative medicine Providers
These investigations suggest that CAM providers may play a crucial role in the health behavior changes made by their patients. How this change occurs — directly, via aspects of the patient-provider relationship, or indirectly, through the delivery of effective therapies — has not been fully investigated. Two theories that may provide useful frameworks for understanding how CAM providers play a role in health behavior change are social cognitive theory (SCT) [27, 28] and self-determination theory (SDT). [28]
Social Cognitive Theory
Within SCT, self-efficacy is a central concept that refers to belief in one’s ability to successfully perform a specific behavior to bring about a desired outcome. [27] The value of self-efficacy in health behavior change is well established, [28, 30] with evidence that increasing self-efficacy leads to health behavior change. [31]
Self-efficacy is important for both initiating and maintaining health behavior change. [27] According to SCT, efficacy and outcome expectancies are discrete but functionally linked concepts that explain how behavior is regulated by forethought. [28] Outcome expectancies are the expectations that engaging in certain behaviors will lead to desired outcomes, whereas efficacy expectancies are based on beliefs about being capable of performing these behaviors. [27] Outcome expectancies motivate behavior change by linking behaviors to outcomes and are therefore most critical for the development of intentions to engage in behaviors. Once intentions are formed, efficacy expectancies provide the chief motivation to initiate and maintain behavior change.
Successful performance of a behavior reinforces self-efficacy beliefs and motivates future behavior. [27] In addition to being fostered by these mastery experiences, self-efficacy can also be encouraged by vicarious experiences (observing others with more experience modeling the behavior and its outcomes); via social persuasions (encouraging statements made by others regarding the likelihood of success); and through feedback provided by physical and emotional states experienced in anticipation of engaging in the behavior. Thus, improving physical and emotional well-being can increase self-efficacy beliefs. [28] It is possible, therefore, that improvements in physical and emotional well-being resulting from CAM therapies and awareness of these improvements are instrumental in the health behavior changes reported by CAM consumers. For example, perceptions of autonomic arousal have been found to significantly influence self-efficacy beliefs for challenging physical tasks. [32]
Body awareness is a multifaceted concept that includes experiencing and identifying the inner sensations and overall state of the body, as well as attending to bodily information and changes in response to emotional and environmental shifts. [33] Enhanced body awareness is an outcome of mind-body therapies such as yoga [34, 35] and has been linked to the use of a greater number of CAM therapies. [36] When defined to include body management and mobilizing one’s physical resources, increasing body awareness is the intention of CAM movement therapies such as the Feldenkrais Method and the Alexander Technique. [29] Also, some touch therapies, such as massage and craniosacral therapy, assist patients with identifying and modulating their physical responses to stress. [37]
There is some evidence that increased body awareness may facilitate health behavior change. One study found that body awareness training resulted in improved stress and symptom management, as well as positive lifestyle changes. [38] In a follow-up study, increased self-efficacy was linked to sustained lifestyle changes. [39]
Self-determination Theory
SDT [29, 40] also has been successfully applied to understanding health behavior change. [41–43] According to this framework, intentional behavior can be viewed as varying along a continuum from being controlled or directed by external forces to being autonomous and intrinsically motivated. [40, 44] Behavior change is better maintained when the regulation of health behaviors is self-determined, when the values and skills for change are internalized. [42] Guidance from outside sources supporting, not directing, an individual’s autonomous choice to make behavior changes promotes sustained change through increasing intrinsic motivation. [44] From this perspective, autonomy support through providing resources, both social and informational, to assist with positive health behaviors may be one way that CAM providers help facilitate behavior change.
The Present Study
Despite the mounting evidence that provider-delivered CAM may facilitate health behavior change, little is known about how this change occurs. With SCT and SDT as guiding explanatory frameworks, we quantitatively and qualitatively examined how several health behavior changes may be facilitated by CAM use. Because our primary interest was how CAM providers may be involved in their patients’ behavior change and not whether they were involved, we opted to examine our hypotheses among people currently using provider-delivered CAM who reported deriving some benefit from their therapy. First, we hypothesized that the outcomes of CAM therapies, specifically increases in body awareness, would facilitate the practice of positive health behaviors such as improved diet and increased physical activity. Consistent with SCT, body awareness can be viewed as a means by which people monitor and evaluate their physical and emotional states and thereby regulate their behaviors.
Second, we hypothesized that increased responsibility for one’s health achieved by the CAM therapies would be positively associated with health behavior change. From the perspective of SCT, believing that self-care is needed in addition to CAM treatments reflects outcome expectancies that link the practice of positive health behaviors with sustaining any improvements gained by CAM therapies. When viewed through the lens of SDT, these beliefs reflect that behavior is autonomously motivated.
Third, we hypothesized that autonomy support from CAM providers would be an additional means through which health behavior change occurs. In line with SDT, the provision of informational and social resources (eg, networking) for making healthy lifestyle changes also could explain how CAM providers influence the health behaviors of their clients. To address these research questions, we used a mixed methods research approach. Our qualitative approach involved conducting a series of focus groups to identify the benefits and outcomes most salient to CAM consumers and to illustrate how CAM providers may have played a role in the health behavior changes reported. We then administered a survey to a larger sample of CAM consumers to examine further the proposed associations between behavioral outcomes and the relevant theoretical constructs from SCT and SDT.
Methods
We obtained institutional review board approval from RTI International (Research Triangle Park, North Carolina) to conduct this research and carried out the research in accordance with universal ethical principles. Informed consent was obtained from all participants.
Participants and RecruitmentFocus Groups. We conducted five focus groups, each consisting of six to eight participants, for a total of 36 participants. Participants were primarily white and non-Hispanic (92%, 33/36), female (83%, 30/36), and well educated (58% with college degrees, 21/36); two-thirds were over age 45; and participants had a broad range of incomes (not shown). Individuals were eligible for this study if they were 21 years of age or older, received treatments by one or more CAM providers for a health problem in the last year, found their treatments to be beneficial, and felt comfortable and willing to discuss their experiences in a group. Participants were recruited with the assistance of local CAM providers who provided a wide range of CAM services representing the five types of CAM services that have been defined by the National Center for Complementary and Alternative Medicine:
whole medical systems (eg, naturopathy, [1] homeopathy, [2] and traditional Chinese medicine [3]);
biologically based practices (eg, use of botanicals, specialized diets, and dietary supplements);
manipulative and body-based practices (eg, chiropractic, massage, Alexander Technique, Feldenkrais Method, and craniosacral therapy [4]);
mind-body interventions (eg, yoga and hypnosis); and energy medicine (eg, acupuncture, Reiki [5]).We focused on CAM modalities that were provider-based rather than self-care practices.

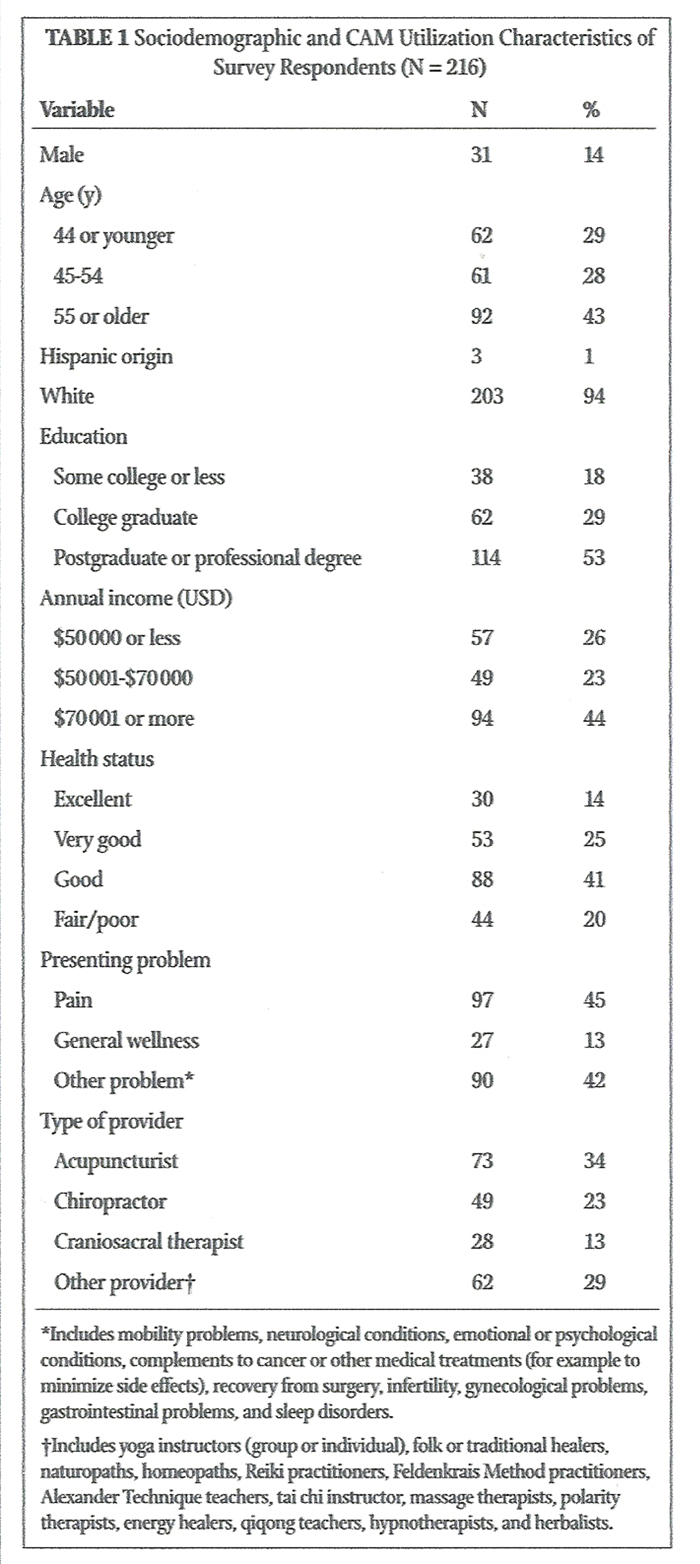
Table 1 Survey. A convenience sample of 216 current CAM consumers completed an anonymous survey distributed through one of three methods: 1,463 surveys were distributed with postage-paid return envelopes through 40 individual CAM providers and health centers; 38 surveys via e-mail to individuals who expressed interest during focus group recruitment; and an unknown but presumably small number of surveys downloaded from the RTI International internal website. To encourage participation, providers were given flyers to post in reception areas, information cards for providers to distribute, and copies of the survey with prepaid envelopes attached to ensure confidentiality. As participation was based on self-selection, it is difficult to estimate the exact refusal rates. Table 1 presents sociodemographic characteristics of the survey respondents, the most significant issues for which they sought provider-delivered CAM treatment in the last 12 months, and the types of CAM providers that they visited most often to treat those issues.
Measures
Focus Groups. Each focus group discussion was conducted in person, audio-recorded, and lasted approximately 2 hours. A focus group moderator led the discussion using a semistructured guide with questions addressing several domains. These included reasons for seeking CAM, types of CAM utilized, behavior change attributed to CAM, physical and emotional outcomes resulting from CAM, and health education resources/information received from CAM provider.
Health Behavior Changes. We created three dependent variables based on a series of questions about health behavior changes made as a result of treatment by the CAM provider visited most often in the last 12 months (for the respondent’s main reason for seeking CAM). An “any behavior change” variable included improving diet, quitting smoking, reducing alcohol consumption, or increasing exercise. We also evaluated improving diet and increasing exercise as two separate dependent variables.
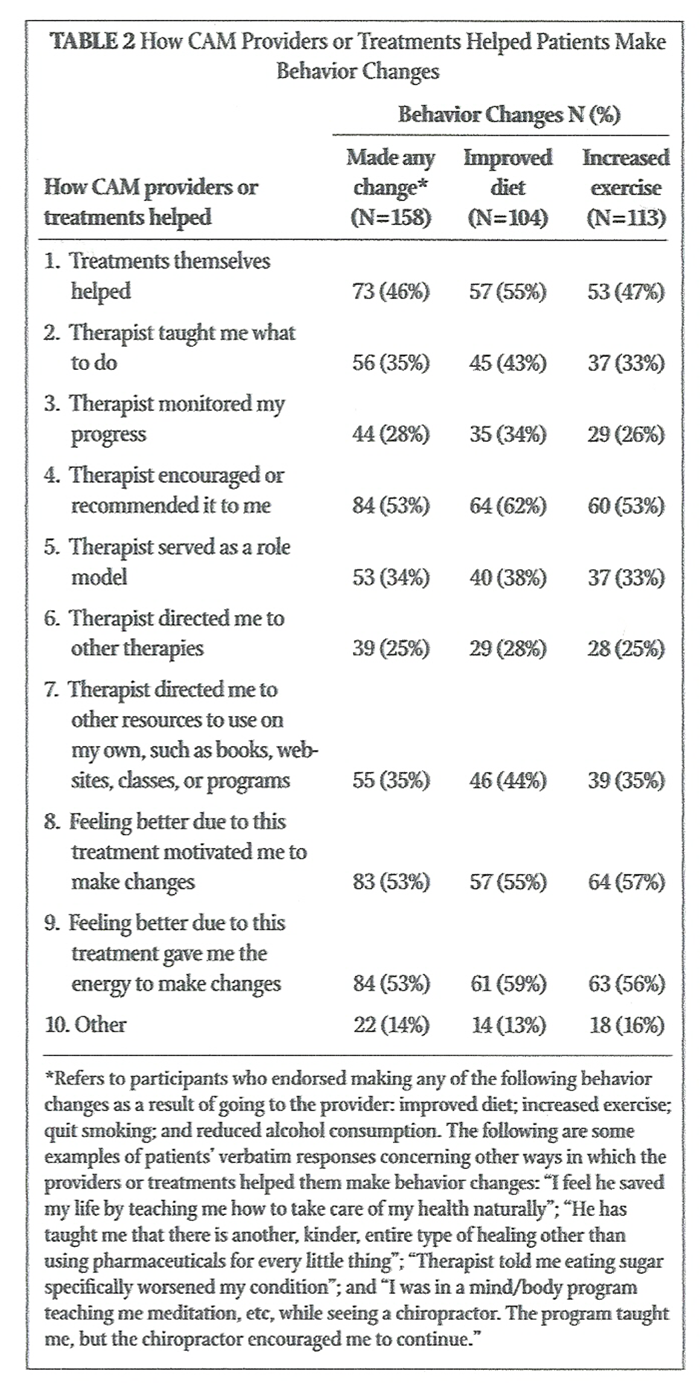
Table 2 Participants who indicated making any of these health behavior changes were then asked to respond “yes” or “no” to nine statements about how going to their CAM providers helped them to make those changes. These statements included direct and indirect ways the providers or the treatments may have contributed to health behavior changes (Table 2). We also asked those respondents who had experienced improvement in their presenting problems due to treatment by their main CAM provider whether they believed that sustained improvement required selfcare (eg, diet or exercise).
Body Awareness. The eight-item RTI Body Awareness Scale45 evaluates the degree to which an individual is able to identify and modulate physical responses to stress. Items begin with the stem, “As a result of receiving treatments from this therapist, . . .” Items such as “Are you more aware of your body in general?” and “Are you better able to release tension in your body?” are scored with response options including “no”; “yes, a little”; and “yes, a lot.” The mean score in the survey sample was 2.30 (SD=0.56), and the Cronbach’s a was 0.90.
Networking. The RTI Networking Scale [45, 46] consists of four items scored on a dichotomous rating scale with 1 (yes) and 2 (no).
Items included(a) “My therapist recommends other activities or resources that might help me
(eg, books, websites, classes, support groups)”;
(b) “I participate in new activities as a result of my therapist’s recommendations
(eg, classes or support groups)”;
(c) “I meet other people with similar problems through my therapist”; and
(d) “I meet other people with similar interests through my therapist.”The mean score in the current sample was 1.20 (SD=1.14).
Analytic StrategyFocus Groups. Each focus group’s comments were transcribed and then reviewed by two research analysts to examine common themes that emerged across all discussions. In particular, we reviewed each of the focus group transcripts to identify statements that could provide illustrative examples and context for our survey findings. We inductively coded statements regarding health behavior change attributed to CAM, physical and emotional outcomes of CAM, and health education resources/information received from CAM provider.
Survey. We first conducted descriptive analyses of the types of health behavior changes made by calculating the percentages of participants who reported(a) improving their diet,
(b) increasing their exercise, and
(c) making any health behavior change due to their CAM treatment.To identify how these changes were made, we determined the percentage of participants who reported each of the possible ways in which their providers or treatments may have helped them make the change. We then conducted a series of logistic regression models to identify which factors were associated with changing diet, increasing exercise, or making any health behavior change. We included the same independent variables in each of these three models: gender, age, health status, presenting problem, type of provider, body awareness (hypothesis 1), whether the participant endorsed that sustained improvement required self-care (hypothesis 2), and networking (hypothesis 3).
Results
Overview of Health Behavior Changes
Overall, 77% of survey participants reported that sustained improvement for their presenting problem required self-care, with a similar number (73%) making a health behavior change as a result of seeking treatment from a CAM provider. Of those who reported making a health behavior change, 66% reported improved diet as a result of going to the provider, and 72% reported increased exercise. Other self-reported behavior changes included 1% who quit smoking and 8% who reduced alcohol consumption.
Based on the focus group data, participants frequently cited dietary and exercise behavior changes as a result of CAM therapy. Dietary changes attributed to CAM therapy ranged from eliminating or reducing certain foods to adopting new dietary practices. For example, one focus group participant commented, “I changed my diet. Part of what I went to . . . acupuncture for was that . . . I was eating very large amounts of sugar.” Another said, “I drink more water and I have quit drinking coffee.”
Increases in exercise were also attributed to CAM therapy, ranging from vigorous activities, such as running, to moderate activities, such as walking or yoga, and were done for reasons such as reduced pain and greater energy following CAM therapy. For example, one focus group participant stated, “I have increased my exercise. Yoga has gotten [me] much stronger and I also run 3 miles a day.” Another focus group participant explained, “I was having severe shoulder and back pains . . . I thought of taking Tai Chi because the physical therapist was talking about it. So once a week I went and within a month I had no problems at all just doing that and then I started yoga classes.”
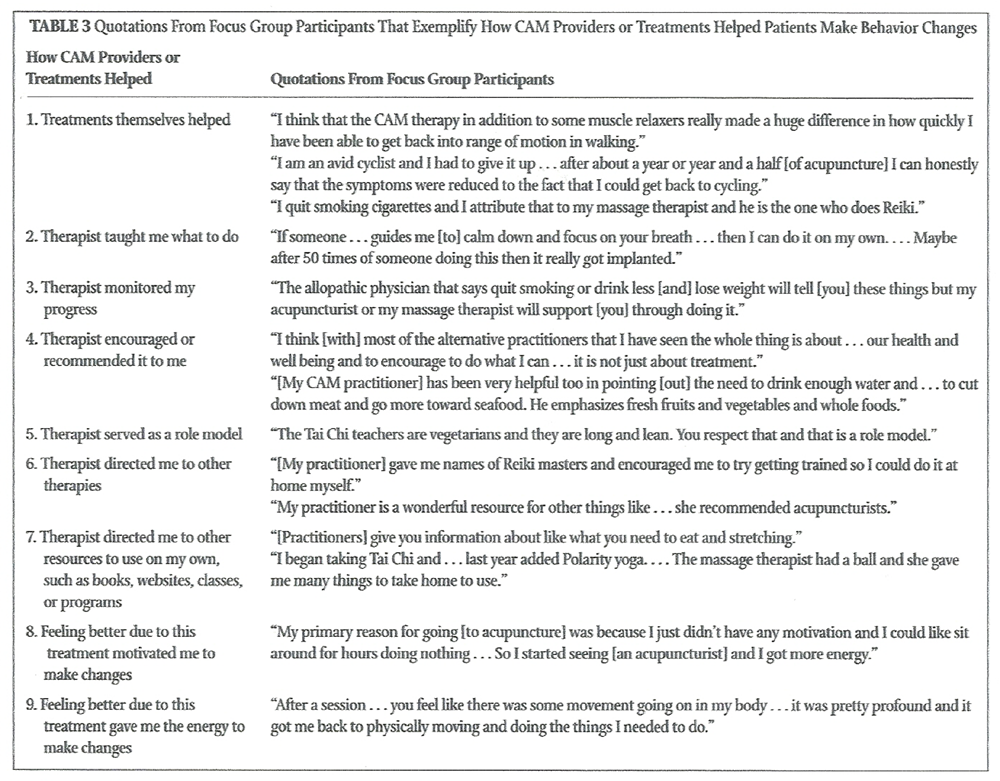
Table 3 How CAM Providers or Treatments Helped Patients Make Behavior Changes. Table 2 presents how receipt of CAM therapy supported health behavior changes. The majority of respondents making behavior changes as a result of going to their CAM providers reported doing so because their providers encouraged or recommended it (53%) and because feeling better due to their treatment motivated them (53%) or gave them energy to make changes (53%). In addition, for the subsets of respondents who improved their diet and increased exercise, many reported that the treatments themselves helped (55% and 47%, respectively). Table 3 provides examples from the focus groups illustrating each of these ways that CAM therapy helped.
Theoretical Predictors of Health Behavior Changes. The qualitative and quantitative findings highlight the importance of the hypothesized predictors based on SCT and SDT (ie, body awareness, endorsing that sustained improvement requires selfcare, and networking). When asked about the physical and emotional outcomes of CAM therapy during focus groups, several participants mentioned that CAM therapies helped them to become more aware of their bodies and health and the connections between their behaviors and their health. For example, one participant said, “This is a strong change in my lifestyle after seeing a couple of practitioners. I am much more alert to any bodily changes or psychological changes and I am much more alert to treating them or getting them treated immediately.”
Similarly, another participant stated that “It isn’t so much for me a symptom and treatment as much as it has been a very different way of life and looking at my body and my health. . . . To think not about so much the cause and effect symptoms but to think more about my overall wellness.” Further, one participant, referring to dietary changes made and the recognition that sustained improvement required self-care, explained, “It seems that when you feel good you want to do things that feel good. I think you are [also] more aware of things that don’t feel good [as a result of CAM treatment].” Another participant said, “I feel like I keep getting healthier from doing CAM things and taking care of myself and getting treatment.”
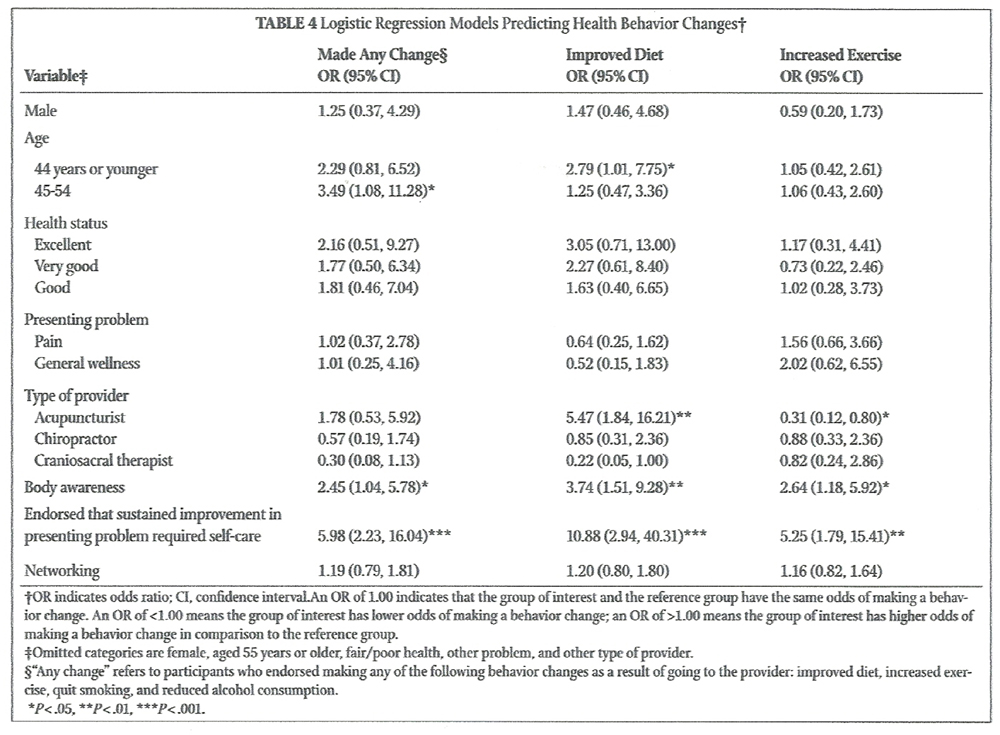
Table 4 Table 4 presents the results of logistic regression models with demographic and theoretical variables predicting health behavior changes. Across all three models, there were few demographic differences between those who made health behavior changes and those who did not. Participants aged 44 years or younger were more likely to improve their diet than older respondents (aged 55 or older), while those who were aged 45 to 54 were more likely to make any positive behavior change when compared to the same group (aged 55 or older). Clients receiving acupuncture were more likely to make dietary changes; however, they were less likely to increase exercise when compared to those seeing providers in the “other” category.
When examined individually (without controlling for endorsing that sustained improvement required self-care or body awareness), networking was significantly related to changes in diet (odds ratio [95% confidence interval] = 1.51 [1.09, 2.08], P=.013) and exercise (OR [95% CI]=1.37 [1.01, 1.86], P= .042), controlling for sociodemographics; however, it was no longer a significant predictor when the other independent variables were included in the model (Table 4). Clients with greater body awareness or who reported that sustained improvement required self-care were significantly more likely to make dietary, exercise, or other positive health behavior changes, after controlling for the other variables
Discussion
This study aimed to answer the question: How do CAM providers play a role in health behavior change? With Social Cognitive Theory (SCT) and Self-determination Theory as guiding frameworks, we examined how health behavior changes, particularly diet and exercise changes, occur in this context: facilitated by the success of CAM therapy, as part of increased responsibility for one’s health, or through the support of CAM providers. Our findings indicate that behavior changes occur through each of these mechanisms. We found qualitative evidence that changes were facilitated by the success of CAM therapy: CAM consumers who made behavior changes directly cited the success of the therapies in helping them make behavior changes.
They also reported that feeling better because of their therapies motivated them and gave them energy to make changes. Further, our quantitative analysis found that increases in body awareness due to CAM therapy promoted improved diet and increased exercise. Consistent with SCT, it appears that monitoring and evaluating the impact of tension and emotions on their bodies and making the connection between dietary and exercise habits and how they feel may have motivated these CAM consumers to make changes. Although we did not directly test for this effect, it seems reasonable to posit that both outcome and efficacy expectancies may have been enhanced by doing so.
Our findings also provide some evidence that behavior change may occur as part of increased responsibility for one’s health, as demonstrated by the linkage of behavior change with the recognition that sustained improvement in one’s health condition requires taking care of oneself through diet, exercise, and other means of self-care. These beliefs reflect increased outcome expectancies from an SCT perspective, and the subsequent behavior changes reflect autonomously motivated behavior from SDT. As several participants noted, the use of CAM made them more aware of how their behaviors and their health were linked. According to SCT, these outcome expectancies motivate behavior by providing the first steps for the development of intentions to engage in behaviors which are then fueled by efficacy expectancies. [27] This awareness in combination with the encouragement and role modeling (efficacy expectations) that participants reported receiving from their CAM providers is one possible explanation of how health behaviors may be promoted in this context.
Finally, we found some evidence that support from CAM providers in the form of encouragement and recommendations, which can be viewed as autonomy support from the SDT perspective, helps CAM consumers make behavior changes. Though CAM providers’ informational and social support (networking) was not a significant predictor when directly compared with increased body awareness and the recognition that sustained improvement required self-care, CAM consumers said that their providers helped them to make behavior changes by teaching them what to do, monitoring their progress, encouraging or recommending behaviors to them, serving as role models, and directing them to other therapies and resources. This finding is consistent with research and theory on the central importance of the provider relationship in CAM care and the holistic model of care underlying CAM that necessarily implies a participatory, patient-centered relationship. [47, 48] Indeed, a preference for a patient-centered style is associated with the decision to use CAM. [49]
Research indicates thatfeelings of trust, [23, 50]
acceptance, [23]
empowerment, [51, 52] and
being supported and cared for [53, 64]are key qualities that consumers feel distinguish CAM care from conventional care. These qualities, along with the increased time that CAM providers tend to spend with clients, provide an appropriate if not ideal context for supportive interactions to flourish. According to SDT, this type of autonomy support from CAM providers would allow their clients to develop intrinsic motivations for making such changes as they learn to value and take personal responsibility for their health.
Our findings extend previous research that supports the idea that CAM use leads to health behavior change, primarily qualitative studies in which patients declared explicitly that CAM use was the reason for their healthful lifestyle changes. [4, 7, 23] This study is unique in that it is the only study that we are aware of that has applied two health behavior change theories, SCT [27, 55] and SDT, [29, 44] as explanatory conceptual frameworks to attempt to explain how behavior change occurs in this context. Consistent with SDT, we found evidence that autonomy support (the provision of social networking) led to behavior change. While we found it was important, it was not as important as body awareness (physical experiences from SCT) and recognizing that sustained improvement requires self-care (outcome expectancies from SCT). In some ways, these findings are similar to Long’s [26] proposition that a supportive treatment environment and practitioner relationship and client openness and readiness to change are critical factors to promote client self-care and lifestyle changes in the context of receiving CAM treatment. Our findings extend the notion that commitment and readiness to change are critical for actual change to occur by further suggesting that the formation of outcome expectancies that connect self-care with health improvement is also necessary. Understanding that the regular practice of any health promoting self-care practice is essential to achieve lasting improvement in health is another important way that CAM treatment may facilitate health behavior change.
Limitations
The findings from this study should be considered within the context of several limitations. Our study population was a relatively small convenience sample of people who likely held pro-CAM attitudes. Indeed, the focus group participants were specifically selected because they believed that CAM therapy had been beneficial to them. Because we were interested in how CAM providers may be involved in health behavior change rather than simply whether such change occurred, this sampling methodology was appropriate. The recruitment technique for survey participants was not ideal, in part because participation was based on self-selection. Calculating a true survey response rate is difficult because we cannot determine how many people actively decided to participate; however, our approach yielded 216 completed surveys out of 1500 distributed, roughly a 15% return. We could have achieved a higher response rate if we had been able to distribute surveys directly to participants and prompt them to reply through follow-up postcards and telephone calls.
In addition, while we attempted to recruit patients from a broad range of CAM providers, most patients in our sample received treatment from acupuncturists and chiropractors. The restricted heterogeneity in participant sociodemographic and CAM utilization characteristics limits the generalizability of these findings. Further research with more representative samples will help clarify the mechanism for the relationship between CAM use and health behavior change more broadly and by specific CAM modality, as there is evidence that treatment-related expectancies are differentially associated with CAM modalities. [21]
This was a cross-sectional study, and the absence of longitudinal data constrains us from examining how CAM providers and CAM therapy itself impact and sustain behavior changes over time. Nonetheless, our questions specifically directed participants to answer with respect to any changes they perceived as a result of CAM therapies. Although we drew on SCT and SDT to hypothesize how behavior changes occur in this context, we did not strictly measure the theoretical constructs as delineated by these theories. Rather, our measures were proxies for these constructs. Indeed, the networking scale captures only a portion of autonomy support — the provision of social and informational resources — and this may have contributed to its lack of significance in the multivariate models. A full and direct test of SDT and SCT models in terms of health behavior change in this context is warranted. Finally, given the complexity of examining the role of CAM providers in health behavior change, unpacking the likely role of confounding factors in the relationship between CAM use and health behavior changes should be examined more thoroughly.
Implications and Conclusion
Even with these considerations, our findings provide insight into the role that CAM providers and treatments play in health behavior change. It is important to understand what motivates individuals to perform health behaviors because they play an important role in disease prevention and control and because adherence rates are poor. [3] Given the benefits of these health behaviors and the general lack of response and difficulty of adhering to recommended guidelines, it is important to investigate further any avenues that may successfully lead to healthy lifestyle changes. Our findings suggest some ways that provider-delivered CAM therapies may support such changes.
Our findings also highlight the utility of applying health behavior change theories such as Social Cognitive Theory (SCT) and Self-determination Theory to understanding how health care providers in general may play a role in promoting healthful lifestyle changes. Relatively few studies that have used SDT to examine how primary care providers may help sustain health behavior change, but those that have indicate that autonomy support is key for increasing behavior change motivation. Physician autonomy support was significantly associated with glycemic control among diabetic patients in one study [56] and longterm medication adherence among outpatients in another study. [57] Although the concept of self-efficacy is well studied in the literature with respect to individual patient levels and the relation to health behaviors, few if any investigations have used SCT to examine the role of primary care physicians with respect to health behavior change. Further research applying these theories is needed to examine potential differences between CAM and conventional care regarding the types of autonomy support provided and the ways in which self-efficacy is encouraged.
The findings show that some CAM providers serve as health coaches (advising, monitoring, encouraging), role models, and agents of change that promote behavior change. Frequent, hourlong visits could support CAM providers’ ability to discuss and encourage lifestyle changes with their clients. [58] Given the range of activities supporting health behavior change that CAM consumers reported, our findings suggest that CAM providers may be an untapped resource for motivating health behavior change that could serve as a complement to the usually brief encounters with medical care providers. This may be especially important as models of health care shift toward becoming more comprehensive, such as in integrative medicine, where conventional and CAM treatments are delivered in a coordinated manner to better address patients’ health concerns.
Given that research on the role of CAM utilization for health behavior change is in its infancy, many questions remain. Further exploration is needed into what motivates people to strive for and maintain optimal health and how CAM therapies can be used to create and sustain motivation for health behavior change.
References:
World Health Organization.
The World Health Report 2002: Reducing Risks, Promoting Healthy Life.
Geneva, Switzerland: World Health Organization; 2002.Mokdad AH, Bowman BA, Ford ES, Vinicor F, Marks JS, Koplan JP.
The continuing epidemics of obesity and diabetes in the United States.
JAMA. 2001;286(10):1195-1200.Williamson AT, Fletcher PC, Dawson KA.
Complementary and alternative medicine: Use in an older population.
J Gerontol Nurs. 2003;29(5):20-28.Kroesen K, Baldwin CM, Brooks AJ, Bell IR.
US Military Veterans' Perceptions of the Conventional Medical Care System
and Their Use of Complementary and Alternative Medicine
Family Practice 2002 (Feb); 19 (1): 57–64Nahin RL, Dahlhamer JM, Taylor BL, et al.
Health behaviors and risk factors in those who use complementary and alternative medicine.
BMC Public Health. 2007 Aug 27;7:217.Stokley S, Cullen KA, Kennedy A, Bardenheier BH.
Adult vaccination coverage levels among users of complementary/alternative medicine—results from the 2002 National Health Interview Survey (NHIS).
BMC Complement Altern Med. 2008 Feb 22;8:6.White MA, Verhoef MJ, Davison BJ, Gunn H, Cooke K.
Seeking mind, body and spirit healing—why some men with prostate cancer choose CAM (complementary and alternative medicine) over conventional cancer treatments.
Integr Med Insights. 2008 Feb1;3:1-11.Sirois FM.
Treatment seeking and experience with complementary/alternative medicine: a continuum of choice.
J Altern Complement Med. 2002;8(2):127-134.Sirois FM.
Provider-based complementary and alternative medicine use among three chronic illness groups: associations with psychosocial factors and concurrent use of conventional health-care services.
Complement Ther Med. 2008;16(2):74-80.Al-Windi A.
Determinants of complementary alternative medicine (CAM) use.
Complement Ther Med. 2004;12(2-3):99-111.Ni H, Simile C, Hardy AM.
Utilization of complementary and alternative medicine by United States adults: Results from the 1999 National Health Interview survey.
Med Care. 2002;40(4):353-358.Druss BG, Rosenheck RA.
Association between use of unconventional therapies and conventional medical services.
JAMA. 1999;282(7):651-656.Garrow D, Egede LE.
Association between complementary and alternative medicine use, preventive care practices,
and use of conventional medical services among adults with diabetes.
Diabetes Care. 2006;29(1):15-19.Downey L, Tyree PT, Lafferty WE.
Preventive screening of women who use complementary and alternative medicine providers.
J Womens Health (Larchmt). 2009;18(8):1133-1143.Sharpe P, Blanck HM, Williams JE, Ainsworth BE, Conway JM.
Use of complementary and alternative medicine for weight control in the United States
J Altern Complement Med. 2007;13(2):217-222.Millar WJ.
Patterns of use—alternative health care practitioners.
Health Rep. 2001;13(1):9-21.Mitzdorf U, Beck K, Horton-Hausknecht J, et al.
Why do patients seek treatment in hospitals of complementary medicine?
J Altern Complement Med. 1999;5(5):463-473.Robinson AR, Crane L, Davidson AJ, Steiner JF.
Association between use of complementary/alternative medicine and health-related behaviors
among health fair participants.
Prev Med. 2002;34(1):51-57.Foltz V, St Pierre Y, Rozenberg S, et al.
Use of complementary and alternative therapies by patients with self-reported chronic back pain:
a nationwide survey in Canada.
Joint Bone Spine. 2005;72(6):571-577.Bishop FL, Yardley L, Lewith GT.
A systematic review of beliefs involved in the use of complementary and alternative medicine.
J Health Psychol. 2007;12(6):851-867.Bishop FL, Yardley L, Lewith GT.
Why do people use different forms of complementary medicine? Multivariate associations between
treatment and illness beliefs and complementary medicine use.
Psychol Health. 2006;21(5):683-698.Sirois FM, Gick ML.
An investigation of the health beliefs and motivations of complementary medicine clients.
Soc Sci Med. 2002;55(6):1025-1037.Cartwright T, Torr R.
Making sense of illness: the experiences of users of complementary medicine.
J Health Psychol. 2005;10(4):559-572.Gould A, MacPherson H.
Patient perspectives on outcomes after treatment with acupuncture.
J Altern Complement Med. 2001;7(3):261-268.Schuster TL, Dobson M, Jauregui M, Blanks RH.
Wellness lifestyles II: Modeling the dynamic of wellness, health lifestyle practices,
and Network Spinal Analysis.
J Altern Complement Med. 2004;10(2):357-367.Long AF.
The potential of complementary and alternative medicine in promoting wellbeing and critical
health literacy: a prospective, observational study of shiatsu.
BMC Complement Altern Med. 2009 Jun 18;9:19.Bandura A.
Self-efficacy: toward a unifying theory of behavioral change.
Psychol Rev. 1977;84(2):191-215.Bandura A.
Health promotion from the perspective of social cognitive theory.
In: Norman P, Abraham C, Conner M, eds.
Understanding and Changing Health Behavior:
From Health Beliefs to Self-Regulation.
Amsterdam, Netherlands: Harwood Academic Publishers; 2000:299-339.Deci EL, Ryan RM.
Intrinsic Motivation and Self-determination in Human Behaviour.
New York, NY: Plenum Press; 1985.Schwarzer R, Fuchs R.
Self-efficacy and health behaviours.
In: Conner M, Norman P, eds.
Predicting Health Behaviour: Research and Practice With Social Cognition Models.
Buckingham, England: Open University Press; 1996:163-196.Strecher VJ, DeVellis BM, Becker MH,
Rosenstock IM. The role of self-efficacy in achieving health behavior change.
Health Educ Behav. 1986;13(1):73-92.Feltz DL, Mugno DA.
A replication of the path analysis of the causal elements in Bandura’s theory of self-efficacy
and the influence of autonomic perception.
J Sport Psychol. 1983;5(3):263-277.Price CJ, Thompson EA.
Measuring dimensions of body connection: body awareness and bodily dissociation.
J Altern Complement Med. 2007;13(9):945-953.Daubenmier JJ.
The relationship of yoga, body awareness, and body responsiveness to self-objectification
and disordered eating.
Psychol Women Q. 2005;29(2):207-219Impett EA, Daubenmier JJ, Hirschman AL.
Minding the body: Yoga, embodiment, and well-being.
Sex Res Soc Pol. 2006;3(4):39-48.Owens JE, Taylor AG, Degood D.
Complementary and alternative medicine and psychologic factors:
toward an individual differences model of complementary and alternative
medicine use and outcomes.
J Altern Complement Med. 1999;5(6):529-541.Walsh EG.
Geriatric applications of craniosacral therapy: established allied professionals’ use of
a complementary modality.
Int J Healing Caring. 2007;7(1).Landsman-Dijkstra JJ, van Wijck R, Groothoff JW, Rispens P.
The short-term effects of a body awareness program: better self-management of health problems
for individuals with chronic a-specific psychosomatic symptoms.
Patient Educ Couns. 2004;55(2):155-167.Landsman-Dijkstra JJ, van Wijck R, Groothoff JW.
The long-term lasting effectiveness on self-efficacy, attribution style, expression of emotions
and quality of life of a body awareness program for chronic a-specific
psychosomatic symptoms.
Patient Educ Couns. 2006;60(1):66-79.Deci EL, Ryan RM.
The “what” and the “why” of goal pursuits:
human needs and the selfdetermination of behavior.
Psychol Inq. 2000;11(4):227-268.Williams GC, Minicucci DS, Kouides RW, et al.
Self-determination, smoking, diet and health.
Health Educ Res. 2002;17(5):512-521.Ryan RM, Patrick H, Deci EL, Williams GC.
Facilitating health behaviour change and its maintenance:
interventions based on Self-Determination Theory.
Eur Health Psychol. 2008;10(1):2-5.Ryan RM, Frederick CM, Lepes D, et al.
Intrinsic motivation and exercise adherence.
Int J Sport Psychol. 1997;28:335-354.Deci EL, Ryan RM.
The support of autonomy and the control of behavior.
J Pers Soc Psychol. 1987;53(6):1024-1037.Walsh EG, Bann C, Greene AM, et al.
Measuring social health outcomes for CAM research.
J Compl Integr Med. 2007;4(1):42.Bann CB, Walsh EG, Sirois FM, Kline T.
Measuring provider support in complementary and alternative medicine.
Paper presented at: 5th Annual IN-CAM Symposium;
November 7-9, 2008; Toronto, Ontario.Paterson C, Britten N.
Acupuncture as a complex intervention: a holistic model.
J Altern Complement Med. 2004;10(5):791-801.Verhoef MJ, Vanderheyden LC, Dryden T, Mallory D, Ware MA.
Evaluating complementary and alternative medicine interventions:
in search of appropriate patient-centered outcome measures.
BMC Complement Altern Med. 2006 Nov 21;6:38.Sirois FM, Purc-Stephenson RJ.
Consumer decision factors for initial and long-term use of
complementary and alternative medicine.
Compl Health Pract Rev. 2008;3(1):3-19.D’Crus A, Wilkinson JM.
Reasons for choosing and complying with complementary health care: an in-house study on a
South Australian clinic.
J Altern Complement Med. 2005;11(6):1107-1112.Shinto L, Yadav V, Morris C, Lapidus JA, Senders A, Bourdette D.
The perceived benefit and satisfaction from conventional and complementary and alternative
medicine (CAM) in people with multiple sclerosis.
Complement Ther Med. 2005;13(4):264-272.Barrett B, Marchand L, Scheder J, et al.
Themes of holism, empowerment, access, and legitimacy define complementary, alternative,
and integrative medicine in relation to conventional biomedicine.
J Altern Complement Med. 2003;9(6):937-947.Luff D, Thomas KJ.
‘Getting somewhere’, feeling cared for: patients’ perspectives on complementary
therapies in the NHS.
Complement Ther Med. 2000;8(4):253-259.Mercer SW, Reilly D.
A qualitative study of patient’s views on the consultation at the Glasgow Homoeopathic Hospital,
an NHS integrative complementary and orthodox medical care unit.
Patient Educ Couns. 2004;53(1):13-18.Bandura A.
Social Foundations of Thought and Action: A Social Cognitive Theory.
Englewood Cliffs, NJ: Prentice Hall; 1985.Williams GC, McGregor HA, King D, Nelson CC, Glasgow RE.
Variation in perceived competence, glycemic control, and patient satisfaction:
relationship to autonomy support from physicians.
Patient Educ Couns. 2005;57(1):39-45.Williams GC, Rodin GC, Ryan RM, Grolnick WS, Deci EL.
Autonomous regulation and long-term medication adherence in adult outpatients.
Health Psychol. 1998;17(3):269-276.Sirois FM. Comment on
“Preventive screening of women who use complementary and alternative medicine providers”.
J Womens Health (Larchmnt). 2009;18(8):119-120.
Return to ALT-MED/CAM ABSTRACTS
Since 6-04-2018
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |