

Remission of Recalcitrant Dermatomyositis
Following a Chiropractic AdjustmentThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Family Med Primary Care 2019 (Nov 15); 8 (11): 3742–3744 ~ FULL TEXT
OPEN ACCESS Eric C. P. Chu, Fa-Sain Lo, and Amiya Bhaumik
New York Chiropractic and Physiotherapy Centre,
New York Medical Group,
Hong Kong, China

Dermatomyositis (DM) is an idiopathic inflammatory myopathy characterized by progressive muscle weakness and pathognomonic skin eruptions. Systemic corticosteroid with or without an immunosuppressive agent is the current treatment of choice in most cases. Cutaneous disease in DM is often refractory and can become the most challenging component to manage effectively. Here, we report a case of recalcitrant DM in a 66-year-old female who sought chiropractic attention for recent episodes of pain and paresthesia in the neck and exacerbation of joint pain. As expected, the musculoskeletal complaints including neck pain, peripheral arthralgia, and muscle weakness that resolved within 1 month after starting treatment. Unexpectedly, dramatic remission of the characteristic skin rashes occurred concurrently. The underlying therapeutic mechanisms of chiropractic remain elusive. This case highlights the importance of family physicians becoming familiar with diagnosing the condition and using a multidisciplinary team approach to treat recalcitrant DM.
KEYWORDS: Chiropractic; dermatomyositis; muscle weakness; skin eruption
From the FULL TEXT Article:
Introduction
Dermatomyositis (DM) is a rare inflammatory myopathy, having a prevalence of fewer than 10 cases per one million people. [1] The pathogenesis is considered to be microangiopathy affecting the skin and muscles, [2] producing rashes, and proximal muscle weakness. This systemic disorder may also affect the joints, esophagus, lungs and less commonly, the heart. The exact cause of DM remains unknown. However, it expresses similar symptoms with autoimmune diseases such as lupus, polymyositis, and necrotizing myopathy. Creatine kinase (CK) is widely used to diagnose myopathies and to follow therapeutic response. However, a CK level does not correlate with the severity of the symptoms. [3] Numerous cytokines can, beneath their action on immune cells, affect muscle and skin cell metabolism and induce inflammation in muscle tissue. Cytokines such as interleukin (IL-1β, IL-6, IL-18) and tumor necrosis factor (TNF-α) are associated with global disease activity in DM. [4] An association with other connective tissue disorders and malignancy makes this diagnosis particularly important to primary care physicians. [1, 3] The mainstay goal of treatment for DM has been aimed at suppressing, or modifying the immune system. A multidisciplinary approach involving family physicians, rheumatologists, dermatologists, and physiotherapists is important in the treatment of classic DM.
Case Report
A 66-year-old female with confirmed dermatomyositis (DM) presented to our chiropractic clinic complaining of long-standing polyarthralgia, skin rashes, and malaise. Thirteen years prior to her presentation, she had been admitted to hospital due to complaints of polyarthralgia, muscle weakness, and a 10-lb body weight loss. She also experienced periorbital swelling and violaceous rash on the forehead, cheeks, V-shape of the neck, and forearms. Investigations at that time showed increased levels of creatine kinase 1658 IU/L (CK reference range: 45–235), lactate dehydrogenase 484 U/L (LDH reference range: 103-–199) and anti-nuclear antibody titer 1:2560 (ANA reference range: <1:40). Histological features of skin biopsy obtained from the chest wall and of muscle biopsy taken from the left deltoid muscle were consistent with dermatomyositis.
The patient was started on prednisone at a high dose plus azathioprine (an immunosuppressant), which resulted in an improvement in the CK levels and overall muscle strength power of the four limbs. However, the skin lesions and peripheral polyarthralgia were refractory, despite aggressive systemic treatments over the past decade. The maintenance regimen consisted of daily oral prednisolone 15 mg, azathioprine 50 mg, and hydroxychloroquine 200 mg (a disease-modifying antirheumatic drug). Biochemical monitoring was performed every 3 months.
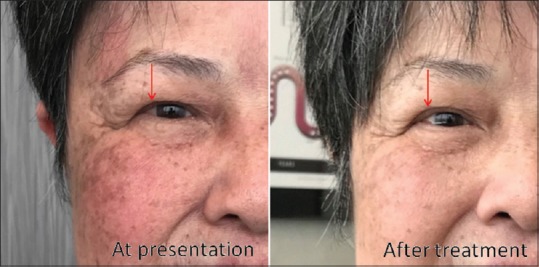
Figure 1
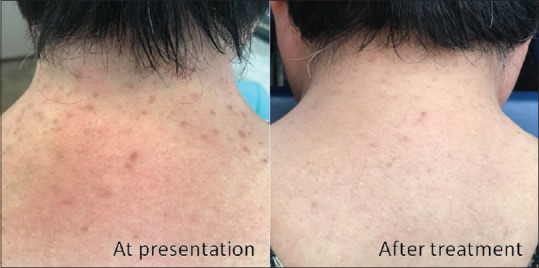
Figure 2 For a recent episode of pain and paresthesia in the neck with an exacerbation of polyarthralgia, the patient sought chiropractic attention. Upon presentation, she utilized a cane to assist with ambulation, and had difficulty climbing stairs and raising her arms. She had mostly characteristic skin manifestations of DM including Gottron's papules, heliotrope rash, shawl-sign rash, periungual erythema, and calcinosis cutis. The examination showed moderate restriction of cervical motion. The patient's pain and paresthesia followed along the left C7 dermatome. According to the Medical Research Council Scale, muscle strength power was 4/5 for the shoulders and 4/5 for the hips bilaterally. In addition, laboratory tests revealed unremarkable inflammatory markers. Radiographs and MRI of cervical and lumbar spine revealed degenerative spondylosis, cervical disc protrusions, and narrowing of the C6/7 left intervertebral foramen, with likely a left C7 nerve root compression.
Chiropractic treatment included ultrasound therapy, manual spinal adjustment, and spinal traction at the lower cervical and upper thoracic regions. Treatment was rendered three times per week for a period of 4 weeks. As expected, nuchal symptoms and peripheral arthralgia reduced after 12 chiropractic sessions. Shoulder muscle strength power had improved to 4+/5 and hip muscle strength power returned to 5/5. She had no difficulty raising both arms overhead and climbing stairs. Unexpectedly, a dramatic remission of her violaceous facial rash, periorbital edema, and the shawl-sign eruption [Figures 1 & 2] occurred concurrently. One month after completion of treatment, the patient resumed most activities of daily living.
Discussion
Cutaneous manifestations play an important role in the DM diagnosis. [2, 4] According to the 2017 European League Against Rheumatism/American College of Rheumatology (EULAR/ACR) classification criteria, patients with pathognomonic skin rashes (heliotrope rash, Gottron's papules and/or Gottron's sign) of DM are accurately classified without including muscle biopsy data. A muscle biopsy is recommended for the patient without these skin manifestations. For patients without muscle involvement, a skin biopsy is performed to further support a DM diagnosis. [5] Our patient fulfilled the EULAR/ACR criteria plus positive skin and muscle biopsies for DM. While cancer is also a specific trigger for some cases of DM, [3] the clinical course and subsequent workup excluded internal malignancy. Given the refractory features of this case, the patient's own observations about treatment outcomes, and the timing of cutaneous improvements following chiropractic adjustment [Figures 1 and 2], it is hard to consider that the clinical remission was spontaneous, although that is a possibility. With regard to the prime pathophysiology, DM is an inflammatory process. It is reasonable to assume that chiropractic efficacy is possibly related to reducing inflammation via certain neuroimmunological processes.
Chiropractic manipulation has been described to boost the immune system on various aspects, including increased numbers of immune cells (lymphocytes and natural killer cells), [6] increased antibody synthesis (IgG and IgM), [7] reduced secretion of proinflammatory cytokines (IL-1β and TNF-α), [7] and normalization of inflammatory markers (IL-6 and C-reactive protein). [8] According to the cholinergic anti-inflammatory pathway proposed, tonic stimulation of the vagus nerve moderates the overproduction of proinflammatory cytokines and protects the body from the harmful effects of excessive inflammation. [9] We speculate that cervical manipulations unintendedly trigger the baroreceptors of the carotid sinus, leading to an interaction between vagus nerve stimulation and cholinergic anti-inflammatory reaction. [10] Moreover, manipulative treatment can help patients stretch the muscles and tendons, release nerve root compression, regain joint function, and prevent muscle atrophy. The therapeutic goal is to maintain function and prevent or minimize sequelae. There is limited research on spinal adjustment for inflammatory diseases and even scarcer wherein symptoms are related to rare diseases like DM. Further research to better clarify the role of chiropractic is necessary.
Conflicts of interest
The authors have no conflicts of interest to declare
References:
Koler RA, Montemarano A.
Dermatomyositis.
Am Fam Physician. 2001;64:1565–72Muro Y, Sugiura K, Akiyama M.
Cutaneous manifestations in dermatomyositis:
Key clinical and serological features- A comprehensive review.
Clin Rev Allergy Immunol. 2016;51:293–302Hu T, Vinik O.
Dermatomyositis and malignancy.
Can Fam Physician. 2019;65:409–11Cassius C, Le Buanec H, Bouaziz JB, Amode R.
Biomarkers in adult dermatomyositis: Tools to help the diagnosis and predict the clinical outcome.
J Immunol Res. 2019;2019:9141420Patel B, Khan N, Werth VP.
Applicability of EULAR/ACR classification criteria for dermatomyositis to amyopathic disease.
J Am Acad Dermatol. 2018;79:77–83.e1Allen JM.
The effects of chiropractic on the immune system: A review of the literature.
Chiro J Aust. 1993;23:132–5. [Google Scholar]Teodorczyk-Injeyan JA, McGregor M, Ruegg R, Injeyan S.
Interleukin 2-regulated In Vitro Antibody Production Following A Single
Spinal Manipulative Treatment in Normal Subjects
Chiropractic & Osteopathy 2010 (Sep 8); 18: 26Roy RA, Boucher JP, Comtois AS.
Inflammatory Response Following a Short-term Course of Chiropractic
Treatment in Subjects with and without Chronic Low Back Pain.
Journal of Chiropractic Medicine, 2010 (Sep);9 (3): 107-114Tracey KJ.
The inflammatory reflex.
Nature. 2002;240:853–9Chu EC, Bellin D.
Remission of myasthenia gravis following cervical adjustment.
AME Case Rep. 2019;3:9.
Return to CASE STUDIES
Since 12-11-2019
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |