

Instrument-Assisted Delivery and the Prevalence of
Reduced Cervical Spine Range of Motion in InfantsThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Chiropractic Journal of Australia 2018 (Jun 15); 46 (2): 162–171 ~ FULL TEXT
OPEN ACCESS Christian Fludder, B.Chiro.Sc, M.Chiro, DACCP, Braden G. Keil, B.App.Sc. (Chiropractic), M.C.Sc. (Paediatrics), FICC, FACCP
Chiropractic Children’s Healthcare,
9 Lower Plenty Road,
Rosanna, VIC, 3084Introduction: Instrument-assisted delivery occurs regularly in Australia. This study aims to determine if there is a higher prevalence of restricted cervical spine range of motion (ROM) in infants born via instrumental delivery or Caesarean section compared to vaginal delivery without instrument assistance.
Methods: Data was collated from all 176 infants under 112 days of age in a paediatric chiropractic clinic. Details regarding method of delivery and instrumental assistance were obtained. Passive ROM assessment was recorded as either “Full” or “Reduced”.
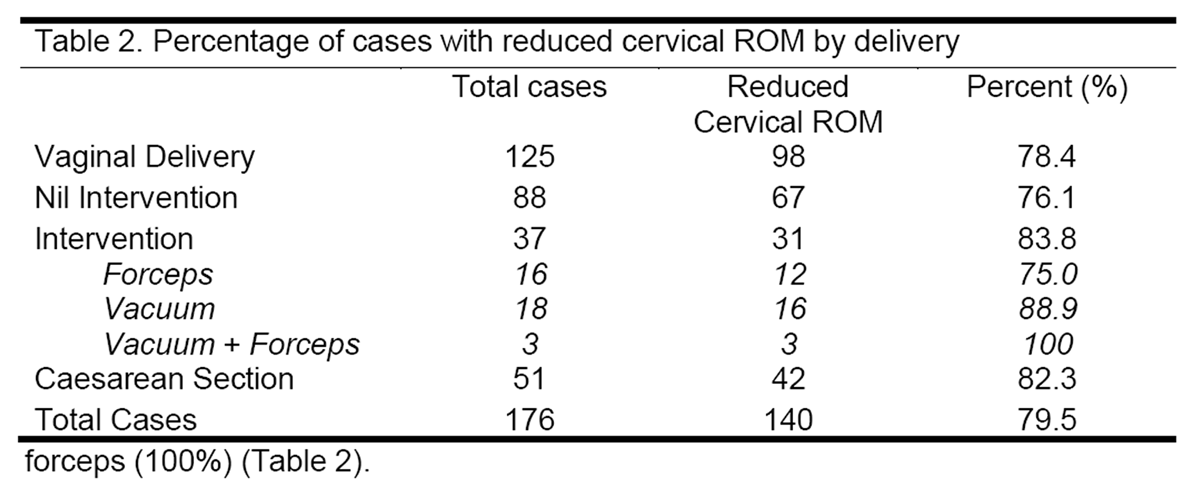
Results: Reduced cervical spine ROM was apparent in 76.1% of infants born vaginally without intervention (n=88), 75.0% with forceps assistance (n=16), 88.9% with vacuum-assistance (n=18), 100% born with vacuum and forceps (n=3), and 82.3% born via Caesarean section (n=51).
Conclusion: Vacuum-assisted delivery and Caesarean section delivery were associated with a higher prevalence of reduced cervical spine ROM when compared to vaginal delivery without assistance. Further research in prospective studies is recommended.
Keyword Indexing Terms: Cervical Range of Motion; Infants; Prevalence; Chiropractic
From the Full-Text Article:
Introduction
The use of instrument to aid in delivery, in the form of forceps or vacuum-assistance, is a frequent occurrence, with instrument assistance occurring in up to 19% of births in Australia. [1, 2] The morbidities associated with instrumental delivery are well documented [3], but there is little data available detailing instrumental delivery and its impact on cervical spine range of motion in infants.
There is evidence in adults that suggests in altering normal cervical spine motion, there is an associated increased risk of alterations in autonomic function [4–6], increased nociception [7], and cortical dysafferentation [8], but this information is lacking for the infant population. However, afferent systems and cortical perceptions of pain are well developed by 30 weeks’ gestation [9, 10], as are the autonomic nervous system and Vagal tone. [11] Cortical effects of altered cervical spine motion in infants has yet to be researched.
Normal values of range of motion in infants aged 2–10 months have been documented, with a mean rotation of 110°, and 75° of lateral flexion. [12] Ohman and Beckung stated that it is “rare for healthy infants to have an imbalance between left and right.”. [12] Restrictions in range of motion are typically attributed to changes in muscular tone. [13, 14] Two processes leading to increased muscle tone have been described; trauma directly to the soft tissue of the neck creates hypertonicity of muscles involved [3], and/or reflex activation of cervical musculature occurs secondary to increased nociception from local articulation. [15] Recent research has indicated that there is a threefold increased risk of birth trauma with forceps-assisted delivery and a fourfold with vacuum-assisted delivery. [3] Furthermore, the process of birthing places high amounts of force through the cervical spine, with up to 120N of compressive force reported for vaginal delivery [16] and over 200N for assisted delivery. [17, 18] This raises the hypothesis of whether the increased forces involved with assisted delivery increases the prevalence of reduced cervical range of motion.
This study aims to determine if there is a higher prevalence of restricted cervical spine range of motion as determined by 4 chiropractors with post-registration training in chiropractic paediatrics in infants born via instrument-assisted delivery (vacuum, forceps or vacuum and forceps) or caesarean section, compared to no instrument assistance vaginal delivery.
Methods:
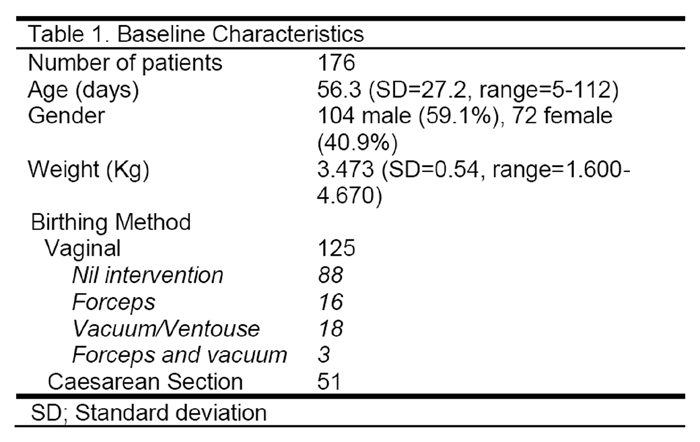
Data were collected from 176 consecutive infants with complete birth details, complete examination findings including birth weight, no previous chiropractic treatment, and 112 days of age or younger that presented to a children’s only chiropractic clinic between 1st January, 2010 to 31st December, 2010.

Table 1 Passive range of motion assessment of the cervical spine was performed with the parent/caregiver present while the infant was held supported in an upright position on the parent/caregiver’s leg to remove external conditions that may limit movement. Rotation was performed by bilaterally rotating the infant’s chin toward each shoulder around the transverse plane. Lateral flexion brought the infant’s ear to the ipsilateral shoulder in the coronal plane. Flexion was assessed by bringing the infant’s head into 30° rotation before flexing the head toward the chest along the sagittal plane. This was done to align the occipitoatlantal articulation to the sagittal plane. In concurrence with methods of range of motion assessment in previous studies, range of motion was decided to be “full” for rotation if the chin was above the acromion, for lateral flexion if the ear touched the shoulder, for flexion if the chin touched the anterior chest, and for extension if the occiput touched upper thoracic region. [13, 14] These methods of motion assessment have been found to have substantial and excellent level of intra- and inter-examiner reliability respectively for rotation and moderate for lateral flexion. [13] If an infant was unable to perform this motion, the finding was listed as “reduced”. Findings from 4 chiropractors with post registration chiropractic paediatric training were collated (Table 1).
Details regarding age at consultation, birth type (listed as vaginal (V), or Caesarean section (CS)), and birthing assistance data regarding forceps or vacuum extraction were recorded. Those born vaginally were categorised based on intervention, listed as nil intervention, forceps, vacuum, and both vacuum and forceps.
Statistical analysis was performed using JASP statistical analysis software. Contingency tables were created where infants with cervical spine ROM restriction were compared to those with normal ROM against infants born without instrumental assistance to those born via forceps, vacuum, or forceps and vacuum to generate a χ2 value. Further analysis was performed to determine the impact of weight and gender. Weights were normally distributed and separated into 6 groups. Differences with values of pŁ0.05 were considered significant, and all results were expressed with a 95% Confidence Interval.
Results:
Table 2
Table 3
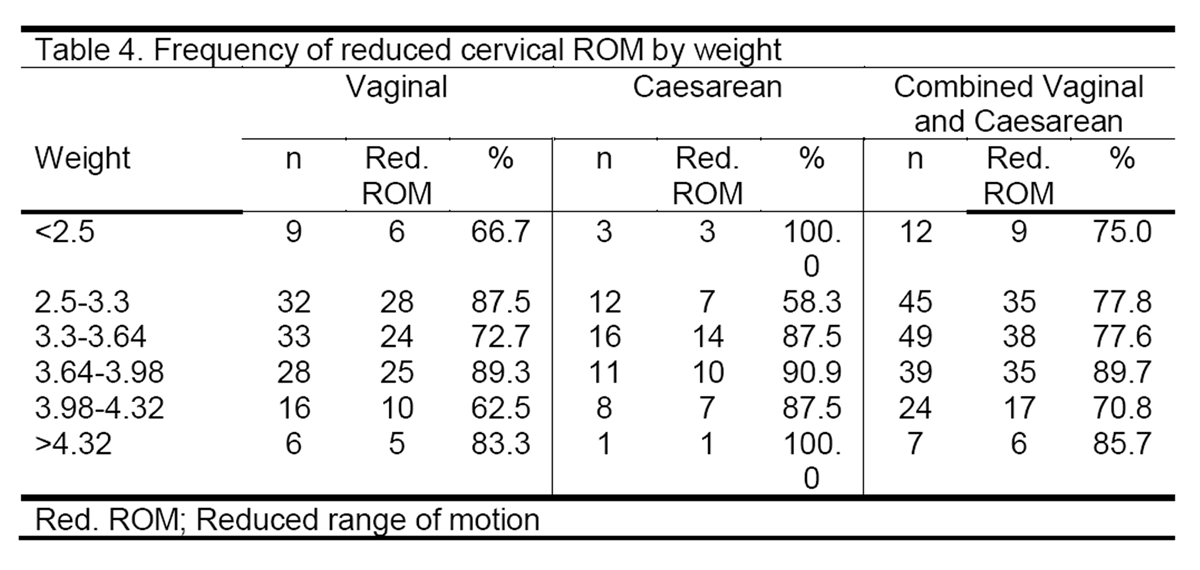
Table 4
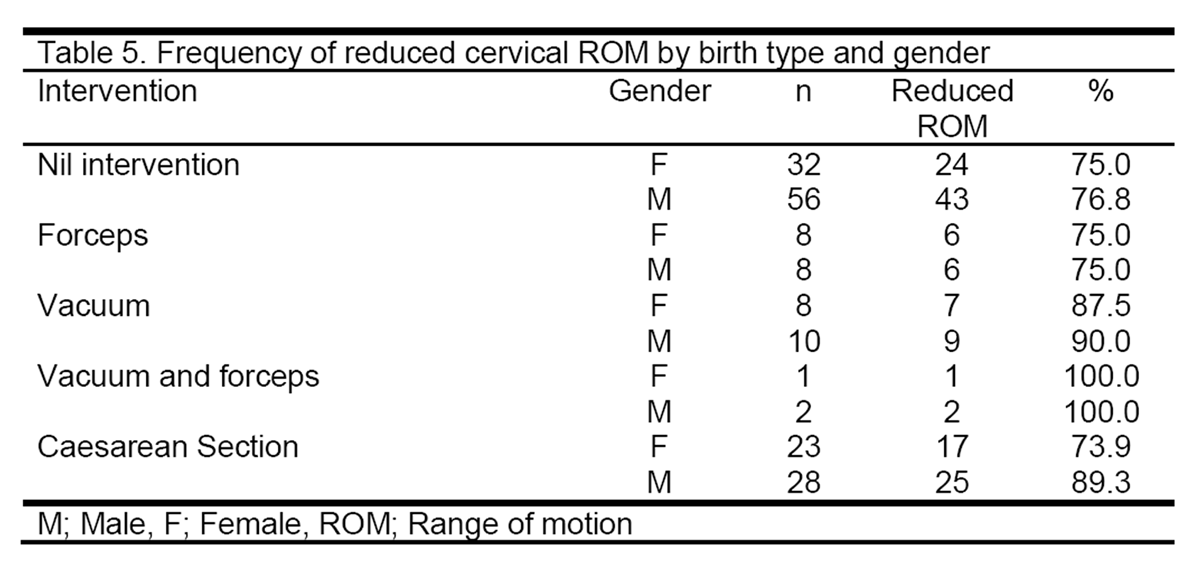
Table 5 In 125 cases of vaginal and 51 cases of caesarean section data, there were 98 cases with reduced cervical spine range of motion from vaginal delivery (78.4%) and 42 from caesarean section (82.3%). 67 cases born vaginally without intervention presented with reduced cervical spine range of motion (76.1%), 12 from forceps delivery (75.0%), 16 from vacuum-assistance (88.9%), and 3 from Vacuum with Chi-squared analysis of infants with or without reduced cervical ROM showed a not statistically significant difference between infants born vaginally compared to Caesarean section (χ2=0.348, df=1, p=0.55). There was a not statistically significant difference between nil intervention and forceps, vacuum, or forceps and vacuum assistance regarding cervical ROM (χ2=1.957, df=3, p=0.581).
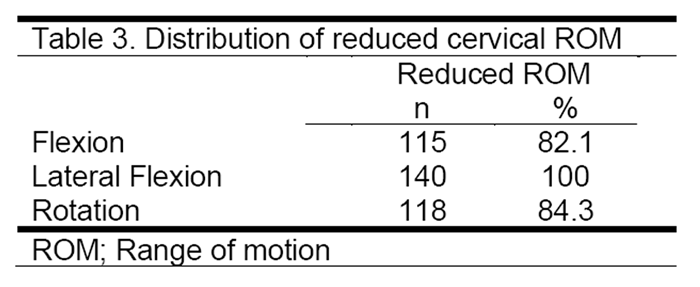
On range of motion analysis, 140 infants were observed to have restrictions in their range of motion (Table 2). Lateral flexion was most frequently reduced, with all infants with restrictions being limited in this motion (Table 3).
There was a modest increase in prevalence of reduced cervical ROM as weight increased,
with this peaking in the 3.64–3.98kg cohort (Table 4).
When assessing based on gender, there are strong similarities across all cohorts except that of those born via Caesarean section (Table 5). Chi-squared analysis of this was not statistically significant (χ2=1.323, df=1, p=0.25).
Discussion
The main result from this study demonstrated that in infants born with vacuum, and vacuum with forceps, we observe a higher prevalence of reduced cervical range of motion compared to infants born without assistance, forceps-assisted delivery or via Caesarean section. However, while we can observe a higher prevalence, we must note that statistical significance was not reached. This is likely due to the low numbers involved in each cohort and the already high prevalence of infants with reduced cervical spine ROM in infants born without intervention.
The use of instrument-assisted deliveries has steadily increased over time, with 2015 data indicating 19% of vaginal deliveries requiring instrument assistance [2], compared to 12.4% in 2011. [1] A recent study by Ashton–Miller et al examined the forces placed on foetal head during labour, with the authors estimating the forces applied to range from 15N (corresponding to a mass equivalent of 1.6 kilograms) at rest to 120N (12.2 kilograms mass equivalence) of compressive force during volitional contraction. [16] Additional studies have demonstrated up to 132N (13.5 kilograms mass equivalence) of tractional force with vacuum-assisted delivery [17], and 196N (20 kilograms mass equivalence) of tractional force with forceps intervention. [18] A recent study by Pettersson et al provided more information on forces involved with vacuum extraction, demonstrating significantly higher forces involved than previously reported. [19] Repeated attempts, posterior position or mid-cavity extractions showed much higher force involved – up to 452N, or the mass equivalence of 46 kilograms, with “33.5% of the vacuum extractions study employed a maximum traction force exceeding the suggested safe maximum force level of 216 N”. [19]
This is concerning as the risk for injury increases above 225N of tractional force, with above 290N seen as “excessively traumatic”. [20] The increased prevalence of cervical spine decreased range of motion after vacuum use found in this study is likely due to the increased tractional force associated with vacuum use. The structure of the infant cervical spine is different to that of an adult, with a more horizontal facet joint angle suggesting stronger biomechanical resistance to compressive rather tractional forces. [21] These findings suggest an under-appreciation of the forces being employed with vacuum delivery, and are certainly consistent with the higher prevalence of reduced cervical spine range of motion in the cohorts involving vacuum assistance. The relationship between vacuum forces and degree of cervical spine range of motion restriction needs further research.
Birthing injuries are defined as “structural or functional deteriorations to the neonate’s body due to a traumatic event at birth”. [3] There are well recognised risk factors associated with birth trauma including higher birth weight and instrumental intervention. [22–24] There is a four times higher chance of birth injury associated with forceps use and three times higher with vacuum extraction. [3] This is partially consistent with our data, with vacuum-assisted deliveries having a higher prevalence of reduced cervical spine range of motion than forceps-assisted or unassisted vaginal delivery.
Birth trauma has been reported to be of a higher incidence in vaginal delivery (30 per 1,000 live births) compared to caesarean section (10 per 1,000 live births) placing vaginal delivery itself as a potential risk factor. [3] This was not consistent with our data, suggesting four possibilities; firstly, the small size of our cohort has skewed the representation of infants presenting with reduced cervical spine range of motion, secondly, that cervical spinal range of motion assessment has been based on previous data from motion assessments in infants with muscular torticollis as reference; not normal, healthy neonates [12], thirdly, the lack of practitioner blinding in assessment produced a biased result, or fourthly, data did not include or assess cervical spine range of motion restriction. A review of 624 cases of infants with infantile torticollis found nearly 50% (304) had a history of requiring forceps or delivery by caesarean section, compared to 37.8% (236) normal vaginal, with over 70% of the cases involved demonstrating reduced cervical range of motion. [25] It is likely that the increased prevalence of cervical spine range of motion restriction associated with vaginal deliveries identified in this study is the result of a more detailed assessment of cervical spine restriction.
Birthweight has been stated as a risk factor for birth trauma, with infant birthweight of 4,000g to 4,500g associated with a twofold increase in birth trauma. [3] In our data we did observe a moderate increase in prevalence of reduced cervical spine ROM as weight increased in Caesarean cases but not in vaginally delivered cases.
One question that arises from this research is that of the impact of reduced cervical spine range of motion resulting from birth. In this study, 140 of the 176 cases presented with restrictions in cervical spine range of motion (79.5%), with 31 of 37 of infants being born with assistance having reduced cervical ROM (83.8%). One concern with reduced range of motion is the development of positional preference. In a 2006 study of 649 infants, Sergueef found a correlation between the development of deformational plagiocephaly and assisted delivery [26], and in a 2016 study of 150 infants with deformational plagiocephaly, over 90% had restrictions in cervical spine range of motion. [13] An additional concern is possible increased risk of developmental delay. In infants with plagiocephaly, Hutchison et al observed a higher prevalence of developmental delay based on results from the Ages and Stages Questionnaire (ASQ) in infants with neck dysfunction (41%) than those without (29%). [27] A 2017 systematic review of plagiocephaly and developmental delay concluded a that there is a strong association. [28]
In the neonatal and infant ages, it is difficult to use specific outcome measures such as pain or cognition tests due to immature cortical development. Evidence of alteration to autonomic function may be used to determine neurological insult. [29] Cervical spine involvement in altered autonomic function as reflected by improvement in heart rate variability upon correction of cervical spine joint dysfunction has been demonstrated. [4–6] Autonomic changes apparent with altered cervical spine function or demonstrated after correction of cervical spine dysfunction are likely to be a result of changes in Vagal nerve function. The Vagus nerve has a key role in gastrointestinal function and consequently may present with signs such as regurgitation or vomiting. This is explained by the role the Vagus nerve has in tonal regulation of the lower oesophageal sphincter. [30]
This may then suggest that the presence of regurgitation, vomiting, reflux or “Silent Reflux” is a reflection of altered autonomic function (Vagal nerve) secondary to altered cervical spine function. This study observed a high prevalence of reduced cervical spine range of motion in infants. It is likely that a significant number of these cases may have Vagal nerve involvement. Further research is needed to compare Vagal nerve function in infants with and without restrictions in cervical spine range of motion as well as Vagal nerve function changes after correction of any restriction in the cervical spine. Future research in this area is strongly recommended as current medical management of these symptoms with proton-pump inhibitors has not been found to be beneficial and may have significant negative outcomes. [31, 32]
There are several limitations with this retrospective analysis. There are small numbers involved in each cohort, a lack of blinding of the practitioner upon assessment, and a confounder based on neonates and infants with reduced cervical spine range of motion being more likely to attend a chiropractic clinic for evaluation. To address these limitations, future prospective studies with a larger cohort, with neonates preferably being assessed by a blinded practitioner shortly after birth, would reduce the impact of these confounders.
Conclusion:
There is a high prevalence of reduced cervical spine range of motion with unassisted vaginal birth, yet there is a higher prevalence involved with vacuum-assisted delivery. However, there was a not statistically significant difference between those born with assistance to those born without assistance or via Caesarean section. Further prospective studies with larger cohorts is recommended.
Ethics Approval and Consent to Participate
This study, as defined by section 5.1.8 of the National Statement of Ethical Conduct of Human Research (2007), carries only negligible risk and as such does not require Ethics Approval. Furthermore, it done in accordance with the Declaration of Helsinki (https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/).
Competing Interests
The authors declare that they have no competing interests
Authors’ Contributions
CF collated, analysed and interpreted patient data regarding presenting behaviours, and was a major contributor in writing the manuscript. BK developed the study concept and was also a major contributor in writing the manuscript.
REFERENCES:
Hilder L, Zhichao Z, Parker M, Jahan S, Chambers G.
Australia's mothers and babies 2012.
Canberra: AIHW; 2012.Australian Institute of Health and Welfare.
Australia's mother and babies 2015 - in brief.
Canberra: 2017.Akangire G, Carter B.
Birth Injuries in Neonates.
Pediatr Rev 2016;37:451–62.Win NN, Jorgensen AMS, Chen YS, Haneline MT.
Effects of Upper and Lower Cervical Spinal Manipulative Therapy on Blood Pressure
and Heart Rate Variability in Volunteers and Patients With Neck Pain:
A Randomized Controlled, Cross-Over, Preliminary Study
Journal of Chiropractic Medicine 2015 (Mar); 14 (1): 1–9Shafiq H, McGregor C, Murphy B.
The Impact of Cervical Manipulation on Heart Rate Variability.
Conf Proc IEEE Eng Med Biol Soc; 2014. pages 3406–9.Zhang J, Dean D, Nosco D, Strathopulos D, Floros M.
Effect of Chiropractic Care on Heart Rate Variability and Pain in a Multisite Clinical Study.
J Manipulative Physiol Ther 2006;29:267–74.Cavanaugh JM, Lu Y, Chen C, Kallakuri S.
Pain generation in lumbar and cervical facet joints.
J Bone Joint Surg Am 2006;88 Suppl 2:63–7.Lelic, D.; Niazi, I.K.; Holt, K.; Jochumsen, M.; Dremstrup, K.; Yielder, P.; Murphy, B.
Manipulation of Dysfunctional Spinal Joints Affects Sensorimotor Integration in the Prefrontal Cortex:
A Brain Source Localization Study
Neural Plast. 2016 (Mar 7); 2016: 3704964Maxwell LG, Malavolta CP, Fraga MV.
Assessment of pain in the neonate.
Clinics in Perinatology 2013;40:457–69.Lee SJ, Ralston HJP, Drey EA, Partridge JC, Rosen MA.
Fetal pain: a systematic multidisciplinary review of the evidence.
JAMA 2005;294:947–54.Mehta SK, Super DM, Connuck D, Salvator A, Singer L, Fradley LG, et al.
Heart rate variability in healthy newborn infants.
The American Journal of Cardiology 2002;89:50–3.Öhman AM, Beckung ERE.
Reference Values for Range of Motion and Muscle Function of the Neck in Infants.
Pediatric Physical Therapy 2008;20:53–8.Murgia M, Venditto T, Paoloni M, Hodo B, Alcuri R, Bernetti A, et al.
Assessing the Cervical Range of Motion in Infants With Positional Plagiocephaly.
Journal of Craniofacial Surgery 2016;27:1060–4.van Vlimmeren LA, van der Graaf Y, Boere-Boonekamp MM, L'Hoir MP, Helders PJM, Engelbert RHH.
Risk Factors for Deformational Plagiocephaly at Birth and at 7 Weeks of Age: A Prospective Cohort Study.
PEDIATRICS 2007;119:e408–18.Knutson GA, Owens EF.
Active and passive characteristics of muscle tone and their relationship to models of subluxation/joint dysfunction: Part I.
J Can Chiropr Assoc 2003;47:168–79.Ashton-Miller JA, DeLancey JOL.
On the Biomechanics of Vaginal Birth and Common Sequelae.
Annu. Rev. Biomed. Eng. 2009;11:163–76.Vacca A.
Vacuum-assisted delivery: An analysis of traction force and maternal and neonatal outcomes.
Aust N Z J Obstet Gynaecol 2006;46:124–7.Pearse WH.
Electronic recording of forceps delivery.
The American Journal of Obstetrics and Gynecology 1963;86:43–51.Pettersson K, Ajne J, Yousaf K, Sturm D, Westgren M, Ajne G.
Traction force during vacuum extraction: a prospective observational study.
BJOG: An International Journal of Obstetrics & Gynaecology 2015;122:1809–16.Wylie B.
Forceps traction, an index of birth difficulty.
YMOB 1963;86:38–42.Lustrin ES, Karakas SP, Ortiz AO, Cinnamon J, Castillo M, Vaheesan K, et al.
Pediatric Cervical Spine: Normal Anatomy, Variants, and Trauma.
RadioGraphics 2003;23:539–60.Muraca GM, Sabr Y, Lisonkova S, Skoll A, Brant R, Cundiff GW, et al.
Perinatal and maternal morbidity and mortality after attempted operative vaginal delivery at midpelvic station.
CMAJ 2017;189:E764–72.Goetzinger KR, Macones GA.
Operative Vaginal Delivery: Current Trends in Obstetrics.
Womens Health (Lond Engl) 2008;4:281–90.Patel RR, Murphy DJ.
Forceps delivery in modern obstetric practice.
BMJ 2004;328:1302–5.Cheng JC, Au AW.
Infantile torticollis: a review of 624 cases.
J Pediatr Orthop 1994;14:802–8.Sergueef N, Nelson KE, Glonek T.
Palpatory diagnosis of plagiocephaly.
Complementary Therapies in Clinical Practice 2006;12:101–10.Hutchison BL, Stewart AW, Mitchell EA.
Characteristics, head shape measurements and developmental delay in 287 consecutive infants
attending a plagiocephaly clinic.
Acta Paediatr. 2009;98:1494–9.Martiniuk ALC, Vujovich-Dunn C, Park M, Yu W, Lucas BR.
Plagiocephaly and Developmental Delay: A Systematic Review.
J Dev Behav Pediatr 2017;38:67–78.Task Force of the European Society of Cardiology and The North American Society
of Pacing and Electrophysiology. Heart rate variability. Standards of measurement, physiological interpretation,
and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing
and Electrophysiology.
Eur. Heart J.1996;17:354–81.Hornby PJ, Abrahams TP.
Central control of lower esophageal sphincter relaxation.
Am. J. Med. 2000;108 Suppl 4a:90S–98S.Tighe M, Afzal NA, Bevan A, Hayen A, Munro A, Beattie RM.
Pharmacological treatment of children with gastro-oesophageal reflux.
Cochrane Database Syst Rev 2014;49:CD008550.van der Pol RJ, Smits MJ, van Wijk MP, Omari TI, Tabbers MM, Benninga MA.
Efficacy of Proton-Pump Inhibitors in Children With Gastroesophageal Reflux Disease: A Systematic Review.
PEDIATRICS 2011;127:925–35.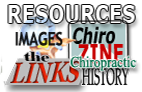
Return to PEDIATRICS
Since 10-01-2019
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |