

The Association Between Psychological and
Social Factors and Spinal Pain in AdolescentsThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: European Journal of Pediatrics 2019 (Mar); 178 (3): 275–286 ~ FULL TEXT
Sarah Batley & Ellen Aartun & Eleanor Boyle & Jan Hartvigsen & Paula J. Stern & Lise Hestbćk
Graduate Studies,
Canadian Memorial Chiropractic College,
6100 Leslie Street,
Toronto, M2H 3J1, Canada.
sbatley@cmcc.ca
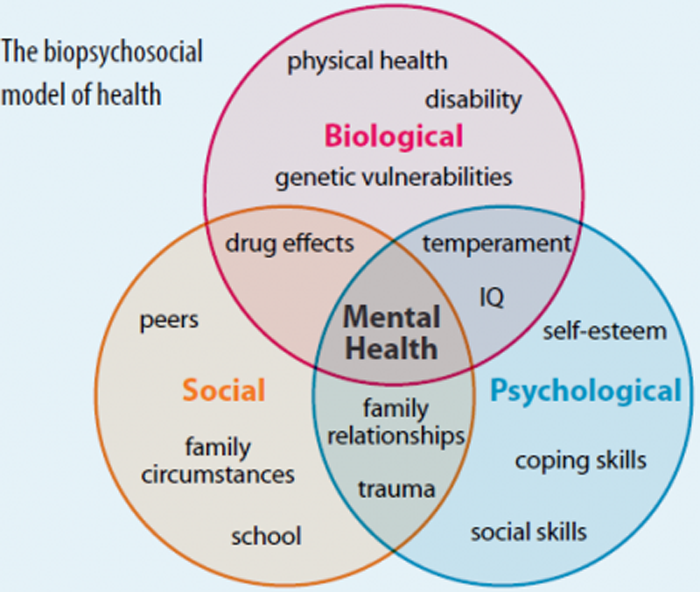
Spinal pain, back pain, and/or neck pain begins early in life and is strongly associated with spinal pain in adulthood. Understanding the relationship between psychological and social factors and adolescent spinal pain may be important in both the prevention and treatment of spinal pain in this age group. We aimed to determine if psychological and social factors were associated with spinal pain in a cross-sectional study of a school-based cohort of 1,279 Danish adolescents aged 11–13, who were categorized into “any” and “substantial” spinal pain.
“Substantial spinal pain” was defined as a lifetime frequency of “sometimes” or “often” and a pain intensity of at least two on the revised Faces Pain Scale. Logistic regression analyses, stratified by sex, were conducted for single and all variables together. Eighty-six percent of participants reported “any spinal pain” and 28% reported “substantial spinal pain”. Frequency of psychological and social factors was significantly higher in those with spinal pain compared to those without. As the frequency of psychological and social factors increased, the odds of both “any spinal pain” and “substantial spinal pain” also increased.
Conclusion: Psychological and social factors may be important determinants in adolescent spinal pain.
KEYWORDS: Adolescent; Back pain; Psychological factor; School children; Social factor; Spinal painAbbreviations
CI = Confidence interval
HBSC = Health Behaviour in School-Aged Children
OR = odds ratio
rFPS = Revised Faces Pain Scale
SP = spinal pain
YSQ = Young Spine Questionnaire
SES = Socioeconomic status
From the FULL TEXT Article
Introduction
Spinal pain (SP) is a major public health concern globally with low back pain and neck pain as leading causes of years lived with disability. [30] SP begins early in life and prevalence increases rapidly during adolescence to reach adult levels by age 18. [4, 8] Thus, SP in adolescence is very common with some studies citing lifetime prevalence rates as high as 86%. [1] The majority of this SP is mild with few consequences; however, a smaller portion of adolescents have more persistent and recurring pain that impacts their daily lives and well-being. [1] Negative consequences of adolescent SP include absence from school, healthcare-seeking behavior, avoidance of sports and activities, as well as decreased quality of life. [19, 20]
SP in adolescence is strongly associated with SP in adulthood. [11, 14] The literature on SP in adult populations illustrates that SP and psychological and social factors are strongly related. [13, 22, 25] A few studies have shown that psychological and social factors are also related to SP in adolescence [7, 24, 28, 31], but this is not as well established. Studies conducted on this age group have found that higher levels of stress, depression, negative behavior, emotional problems, poorer overall well-being, and higher levels of peer problems increase the odds of reporting SP. [7, 24, 28, 31]
Therefore, the primary objective of this study was to determine if psychological and social factors are associated with SP in a cohort of Danish adolescents aged 11–13 years.
Methods
Study design
This study was cross sectional in nature and was a secondary analysis of baseline data collected in May and June of 2010 in connection with the School site, Play spot, Active transport, Club fitness, and Environment (SPACE) study. [29]
Setting and data collection
The SPACE study was conducted at 14 schools in the Region of Southern Denmark. It was designed to test the effect of optimizing the physical environment around the schools to promote physical activity. [29] At baseline, the students completed an e-survey that included questions about SP as well as psychological and social factors. The survey was completed under supervision of the teacher during class time.
Participants
Students at the participating schools aged 11 to 13 years (n = 1,348) were eligible for the study. Those who assented and responded to all of the SP-related questions were included in this study.
Ethics
For the SPACE study, a letterwas sent to parents informing them of the study and that they could withdraw their child’s participation at any time. For more details, see the SPACE protocol. [29] The Regional Ethics Committee for Southern Denmark was advised about the study and data collection. Under Danish law, no ethics approval was needed because the study did not include any invasive tests or interventions. Approval was obtained from the Danish Data Protection Agency (#2010-41-5147). For the current study, Research Ethics Board approval was obtained from Canadian Memorial Chiropractic College (#172011).
VariablesSpinal pain (dependent variables) The Young Spine Questionnaire (YSQ), embedded in the SPACE e-survey [29], was used to assess lifetime occurrence of SP. The YSQ was developed for 9–11-year olds and has satisfactory feasibility, content validity, and item agreement between questionnaire scores and interview findings. [21]
The YSQ assesses the three spinal regions, neck, mid back, and low back, separately. For lifetime prevalence of pain, the participant was asked: “Have you ever had pain in your (specific region listed)?” with the response categories of “often”, “sometimes”, “once or twice”, and “never”. The participants who responded at least “once or twice” were asked to assess their worst pain ever using the revised Faces Pain Scale (rFPS). This scale is based on six faces that illustrate progressively worsening pain and can be scored from 0, representing no pain, to 5, representing worst imaginable pain. The rFPS has been found to be valid and appropriate for use in assessing pain intensity in children over the age of 4. [16]
The three spinal pain regions were collapsed into one category indicating SP in any region. A previous study on this population found that there was a high overlap of pain between the three spinal regions. [1] “Any SP” was defined as any frequency of SP above “never” regardless of intensity level. “Substantial SP” was defined as a frequency of “sometimes” or “often” in at least one spinal region with a corresponding pain intensity of at least 2 on the rFPS. Stallknecht et al. previously used this method of defining SP from the YSQ. [28]
Psychological and social factors (independent variables) Data on psychological and social factors was collected using questions from the Health Behaviour in School-Aged Children: World Health Organization Collaboration Cross- National Survey (HBSC) [27] that was embedded in the SPACE e-survey. [29] The HBSC questions are subject to validation studies and piloting at national and international levels. [27] The four-item psychological subscale has been found to have good internal validity, convergent validity, and discriminant validity. [10]
For each of the psychological variables, the questionnaire asks them: “In the past six months, how often have you been feeling low/bad mood/nervousness/difficulty sleeping?”. The response categories were “every day”, “more than once a week”, “almost every week”, “almost every month”, and “rarely or never”. The social variables related to loneliness and pupil acceptance and the questions were: “Do you feel lonely?” with the response options: “no”/“sometimes”/“often”/“very often”, and “Other pupils accept me as I am?” with the response options: “Strongly agree”/“agree”/“neither agree nor disagree”/“disagree”/“strongly disagree”.
Other variables of interest
Age, socioeconomic status (SES), smoking, and alcohol were identified as covariates. Low SES has been shown to be associated with poorer overall health and there is high-quality evidence from a recent systematic review to suggest that low SES is a risk factor for developing musculoskeletal pain in adolescents. [17] Low SES is also associated with higher levels of mental health problems. [26] SES was based on the father’s occupation at follow-up 2 years later and coded according to the Danish Occupational Social Class Measure. [6] SES was classified as high, middle, or low based on these ratings. Smoking has been shown to increase the odds of reporting LBP, and alcohol consumption has been found to be positively associated with current LBP in adolescents and young adults. [12, 15, 23] Smoking and alcohol consumption have also been identified as risk factors for mental health problems in adolescents. [3, 5] A participant was considered to smoke if they reported smoking at least once every week and to drink if they reported drinking alcohol at least once every month.
Data analysis
Descriptive statistics were used to present the study cohort in terms of psychological and social factors aswell as SP. Results are presented as frequencies and percentages.
We constructed multiple logistic regression models to determine the association between the psychological and social variables and the two outcomes. The models were adjusted for age and SES, but due to rather small proportions of children smoking and drinking, these variables were not included (n = 6 and n = 86, respectively). We also checked if any interactions existed between the psychological and social variables. All regression analyses were stratified by sex. Adjusted odds ratios (OR) with 95% confidence intervals (CI) were reported.
To determine if there was an independent relationship between the psychological and social variables and the two outcomes, an exploratory factor analysis was first conducted for each of the constructs to determine if they would load onto the same factor, because a scoring system to estimate a combined score has not been created previously.
The psychological variables loaded onto the same factor; therefore, a scoring system was developed where a value of “0” to “4” was assigned to the response categories (“0” = never/ rarely, “1” = almost every month, “2” = almost every week, “3 = more than once per week, and “4” = almost every day). The values were summed across the four variables to reach a composite psychological score that could range from “0” to “16”. There was no linear relationship between the composite psychological score and the two outcomes, and we therefore categorized the score into three categories: (1) no psychological complaints (value of 0), (2) low composite psychological score (value of 1 to 4), and (3) high composite psychological score (value of 5 to 16). A one-factor solution for the social variables could not be found. The regression analyses described above were repeated for the composite psychological score.
Statistical significance was set at a p value of less than 0.05 (p < 0.05) for all analyses.
All statistical analyses were carried out in Stata 15.0 (StataCorp, College Station, Texas, USA).
Discussion
In this sample of Danish adolescents, the odds of reporting “any SP” or “substantial SP” were greatly increased with higher frequencies of psychological factors with ORs ranging from 2 to 13. Participants reporting “any SP” or “substantial SP” reported significantly higher frequencies of all four psychological factors than those without SP. Furthermore, reporting multiple psychological factors with higher frequencies, indicated by a higher composite psychological score, resulted in an increased OR of reporting SP.
Recently, Stallknecht et al. found that Danish adolescents aged 10–14 reporting medium and high values of stress had an increased OR of reporting SP compared to those reporting no stress. [28] Adolescents who reported poorer general wellbeing also had increased odds for reporting SP compared to those who reported better well-being. [28] Similarly, in Dutch adolescents aged 12–16, stress and depressive symptoms were found to be associated with neck pain/shoulder pain and low back pain. [7] Two British studies assessed emotional factors in British adolescents aged 11–14 using the Strengths and Difficulties Questionnaire and both found that participants reporting high levels of “negative” behavior were significantly more likely to report low back pain. [24, 31] Another British study found that children aged 11–14 who reported higher levels of psychosocial difficulties were more likely to develop LBP compared to their peers. [18]
Previous studies have shown inconsistent evidence for the effect of sleep quantity on back pain onset in adolescents. [2] There is moderate evidence of no higher risk of poor sleep quality with back pain onset. [2] There is moderate quality evidence that boys with daytime tiredness are not at higher risk of back pain, but this evidence is inconsistent in girls. [2] Recent reviews have shown that there is a reciprocal relationship between sleep and pain and that sleep impairments are a stronger predictor of pain than pain is of sleep impairments. [9]
In our study, those reporting “any SP” or “substantial SP” reported significantly higher levels of loneliness and lower levels of pupil acceptance than those without SP. When the social variables were both included in an analysis together with SP, associations were still positive, but the estimates were lower and most of them not statistically significant. These findings are similar to a study by Watson et al. where participants reporting high levels of pupil problems had a small but significant OR for reporting LBP compared to those reporting low levels of pupil problems. [31]
When the composite psychological score and social variables were included in the same analysis, all the estimates were reduced. This indicates that loneliness and psychological scores are likely interdependent and thus lower the effect of one another when included in the same model.
There are several strengths in this study including the high participation rate (95%). The sample is also representative of the Danish population, increasing the generalizability of the study. The HBSC questionnaire is subjected to validation and piloting at national and international level [27] and the YSQ was developed and tested for this age group. [21] This study also provides information on two definitions of SP, which allows us to comment on the association between the frequency of psychological and social factors and the severity of reported SP.
However, this study also has some limitations. Due to the cross-sectional nature, neither causation nor direction of association can be determined. The 95% CI for some associations are quite wide, and thus, results should be interpreted with caution. Due to missing SES data, a substantial number of participants were excluded from the adjusted analyses. These participants reported significantly higher frequencies of low mood, nervousness, loneliness, and pupil acceptance. Thus, their exclusion from the adjusted analyses have likely resulted in an underestimation of the reported ORs. Finally, the composite psychological scoring has not undergone a validation process.
There was a high prevalence of psychological and social factors among adolescents in this study cohort. Previous studies have shown that depression, stress, anxiety, sleeping difficulties, and loneliness can all result in negative health-related consequences, including SP. With SP causing such a high level of disability in the population, and SP beginning early in life, it is important to understand the factors associated with the development and perpetuation of SP in adolescents. A better understanding of these factors is likely to lead to better preventative measures as well as more comprehensive intervention strategies in adolescents with SP.
Conclusion
This study indicated that psychological and social factors are associated with SP in adolescents with a higher frequency of these reported factors resulting in higher odds of reporting SP, especially “substantial SP”. Psychological factors appear to be more strongly related to SP than the social variables. Together, this reinforces the importance of understanding psychological and social factors in adolescents reporting SP.
References:
Aartun E, Hartvigsen J, Wedderkopp N, Hestbaek L (2014)
Spinal Pain in Adolescents: Prevalence, Incidence, and Course:
A School-based Two-year Prospective Cohort Study in 1,300 Danes Aged 11-13
BMC Musculoskelet Disord. 2014 (May 29); 15: 187Andreucci MA, Campbell P, Dunn KM (2017)
Are sleep problems a risk factor for the onset of musculoskeletal pain
in children and adolescents? A systematic review.
Sleep 40(7):1–11Cairns K, Yap M, Pilkington P, Jorm A (2014)
Risk and protective factors for depression that adolescents can modify:
a systematic review and meta-analysis of longitudinal studies.
J Affect Disord 169:61–75Calvo-Munoz I, Gomez-Conesa A, Sanchez-Meca J (2013)
Prevalence of Low Back Pain in Children and Adolescents: A Meta-analysis
BMC Pediatr. 2013 (Jan 26); 13: 14Chaiton MO, Cohen JE, O'Loughlin J, Rehm J (2009)
A systematic review of longitudinal studies on the association between depression and smoking in adolescents.
BMC Public Health 9:356Christensen U,Krolner R, Nilsson CJ, Lyngbye PW, Hougaard CO, (2014)
Addressing social inequality in aging by the Danish occupational social class measurement.
J Aging Health 26(1):106–127Diepenmaat AC, van der Wal MF, de Vet HC, Hirasing RA (2006)
Neck/shoulder, low back, and arm pain in relation to computer use, physical activity, stress,
and depression among Dutch adolescents.
Pediatrics 117(2):412–416Dunn KM, Hestbaek L, Cassidy JD (2013)
Low Back Pain Across the Life Course
Best Pract Res Clin Rheumatol 2013 (Oct); 27 (5): 591-600Finan P, Goodin B, Smith M (2013)
The association of sleep and pain: an update and a path forward.
J Pain 14(12):1539–1552Gariepy G,McKinnon B, SentenacM, Elgar FJ (2015)
Validity and reliability of a brief symptom checklist to measure psychological health
in school-aged children.
Child Indic Res 9(2):471–484HarrebyM, Neergaard K, Hesselsoe G, Kjer J (1995)
Are radiological changes in the thoracic spine and lumbar spine of adolescents risk factors
for low back pain in adults? A 25 year prospective cohort of 640 school children.
Spine 20(21):2298–2302Heaps N, DavisM, Smith A, Straker L (2011)
Adolescent drug use, psychosocial functioning and spinal pain.
J Health Psychol 16:688–698Hemingway H, Shipley M, Standfield S, Marmot M (1997)
Sickness absence from back pain, psychosocial work characteristics and
employment grade among office worker.
Scand J Work Environ Healt 23:8Hestbaek L, Leboeuf-Yde C, Kyvik KO, Manniche C:
The Course of Low Back Pain from Adolescence to Adulthood:
Eight-year Follow-up of 9600 Twins
Spine (Phila Pa 1976). 2006 (Feb 15); 31 (4): 468–472Hestbaek L, Leboeuf-Yde C, Kyvik KO (2006)
Are lifestyle-factors in adolescence predictors for adult low back pain?
A cross-sectional and prospective study of young twins.
BMC Musculoskelet Disord 7:27Hicks CL, von Baeyer CL, Spafford PA, von Korlaar I, Goodenough L (2001)
The faces pain scale–revised - toward a common metric in pediatric pain measurement.
Pain 93(2):11Huguet A, Tougas ME, Hayden J, McGrath PJ, Stinson JN, Chambers CT (2016)
Systematic review with meta-analysis of childhood and adolescent risk
and prognostic factors for musculoskeletal pain.
Pain 157(12):2640–2656Jones GT, Watson KD, Silman AJ, Symons DPM, Macfarlane GJ (2003)
Predictors of low back pain in British schoolchildren:
a population-based prospective cohort study.
Pediatrics 111(4):8Jones MA, Stratton G, Reilly T, Unnithan VB (2004)
A schoolbased survey of recurrent non-specific low-back pain prevalence and
consequences in children.
Health Educ Res 19(3):284–289Kjaer P, Wedderkopp N, Korsholm L, Leboeuf-Yde C.
Prevalence and Tracking of Back Pain From Childhood to Adolescence
BMC Musculoskelet Disord. 2011 (May 16); 12: 98Lauridsen HH, Hestbaek L.
Development of the Young Spine Questionnaire
BMC Musculoskelet Disord 2013 (Jun 12); 14: 185Linton SJ (2000)
A review of psychological risk factors in Back and neck pain.
Spine 25(9):9Mikkonen P, Leino-Arjas P, Remes J, Zitting P, Taimela S, Karppinen J (2008)
Is smoking a risk factor for low back pain in adolescents?
A prospective cohort study. Spine 33:527–532Murphy S, Buckle P, Stubbs D (2007)
A cross-sectional study of self-reported back and neck pain among English schoolchildren
and associated physical and psychological risk factors.
Appl Ergon 38(6):797–804Mustard CA, Kalcevich C, Frank JW, Boyle M (2005)
Childhood and early adult predictors of risk of incident back pain:
Ontario child health study 2001 follow-up.
Am J Epidemiol 162(8):779–786Reiss F (2013)
Socioeconomic inequalities and mental health problems in children and adolescents:
a systematic review.
Soc Sci Med 90:24–31Roberts C, Freeman J, Samdal O, Schnohr CW, de Looze ME, Nic Gabhainn S, (2009)
The health behaviour in school-aged children (HBSC) study:
methodological developments and current tensions.
Int J Public Health 54(Suppl 2):140–150Stallknecht SE, Strandberg-Larsen K, Hestbaek L, Andersen AN (2017)
Spinal Pain and Co-occurrence with Stress and General Well-being Among Young Adolescents:
A Study Within the Danish National Birth Cohort
European Journal of Pediatrics 2017 (Jun); 176 (6): 807–814Toftager M, Christiansen LB, Kristensen PL, Troelsen J (2011)
SPACE for physical activity - amulticomponent intervention study:
study design and baseline findings from a cluster randomized controlled trial.
BMC Public Health 11(777):11Vos T, Allen C, Arora M, Barber RM, Bhutta ZA, Brown A, Carter A, et.al (2016)
Global, regional, and national incidence, prevalence, and years lived with disability for
310 diseases and injuries, 1990–2015: a systematic analysis for the
global burden of disease study 2015.
Lancet 388(10053):1545–1602Watson K, Papageorgiou A, Jones G, Taylor S, Symmons D, Silman A, (2003)
Low back pain in schoolchildren - the role of mechanical and psychosocial factors.
Arch Dis Child 88:6
Return to PEDIATRICS
Return to NECK AND BACK PAIN
Return to BIOPSYCHOSOCIAL MODEL
Since 11-28-2018
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |