

The Infant with Dysfunctional Feeding Patterns û
The Chiropractic AssessmentThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Clinical Chiropractic Pediatrics 2016 (May); 15 (2): 1230 ~ FULL TEXT
OPEN ACCESS Sharon Vallone, DC, FICCP and Faraneh Carnegie-Hargreaves, DC
Private practice,
South Windsor,
Connecticut, USAThe World Health Organization recommends exclusive breastfeeding for the first 6 months of an infantÆs life, followed by the introduction of complementary foods while breastfeeding for 2 years and beyond. Early and consistent breastfeeding support can often make the difference in a dyadÆs ability to establish a functional breastfeeding relationship. While challenged dyads can sometimes accomplish competent breastfeeding given appropriate support, necessary interventions, and an opportunity to learn; timing is critical when a neonate has not been transferring adequate milk volume or is managing feeding in a passive or compensatory manner. Chiropractors should be most familiar with the diagnosis and treatment of musculoskeletal dysfunctions that could result in an inability to feed. They should also recognize and treat the compensatory changes that will develop in a healthy, neurotypical neonate who is challenged by an inability to feed efficiently in order to prevent the evolution of long term physiologic and postural ramifications.
Key words: breastfeeding, dysfunctional feeding, chiropractic, International Board Certified Lactation Consultant, tethered oral tissue, tongue tie, lip tie, neonate, pediatric.
From the FULL TEXT Article:
Introduction
The World Health Organization recommends exclusive breastfeeding for the first 6 months of an infantÆs life, followed by the introduction of complementary foods while breastfeeding for 2 years and beyond.1
According to the 2014 breastfeeding report card produced by the CDC, breastfeeding rates continue to rise in the United States. In 2011, 79% of newborn infants started to breastfeed, 49% were breastfeeding at 6 months, and 27% at 12 months. (However, it is important to note that this does not represent exclusivity, as another CDC report states that exclusivity rates did not rise between 2002 and 2012). [2] Additionally, the number of IBCLCs (International Board Certified Lactation Consultants), and others trained to support breastfeeding in various clinical and community settings has also increased. [3, 4] Short-term risks of artificial-feeding have been well-documented across the literature and include increased obesity and incidence of infection ù including acute otitis media, respiratory tract and gastrointestinal infection. In the long term, failure to breastfeed is likely a factor in the development of inflammatory bowel disease, celiac disease, and diabetes. Artificial-feeding has also been associated with increased blood pressure and cholesterol levels in adulthood. [5]
Early and consistent breastfeeding support can often make the difference in a dyadÆs ability to establish a functional breastfeeding relationship. [6] Despite the fact that challenged dyads can still accomplish successful breastfeeding given time-appropriate support and interventions, timing is critical when a neonate has not been transferring milk. If released from the hospital without appropriate assessment of latch and transfer, symptoms may not appear until the dyad has gone home and the neonateÆs status can rapidly decline. Neifert (2001) makes a compelling argument for the importance of recognizing and resolving breastfeeding dysfunction as it affects neonatal health: ôClinicians must overcome the tendency to view the complications of mismanaged breastfeeding as an indictment of the ôprocessö. Instead, pediatric practitioners are obligated to confront the reality of breastfeeding failure, identify associated risk factors and implement intervention strategies to prevent infant morbidity.ö [7]
Once at home, an infant who cannot transfer milk may quickly become a lethargic infant but may be perceived as a well-behaved baby. Even if parents express concern, they are often advised not to wake a sleeping baby by well-intentioned but ill-informed family, friends, or healthcare providers. Without daily weights to observe weight loss (or gain), or taking note of the requisite number of wet diapers or stools produced, this failure to feed may go unnoticed until the situation has become tenuous, or worse, untenable. When the infant is unable to transfer a sufficient amount of milk to sustain normal activity, they will often fall asleep at the breast waking shortly afterward and crying inconsolably until put to breast again. Other signs of inadequate milk transfer include feeding for short intervals very frequently or the infant who never gets off the breast yet fails to gain weight and meet developmental milestones. [8] Alternatively, these babies may gain adequately in the shortterm if the mother has a robust milk supply and is willing to nurse very frequently, however milk supply is dependent upon milk removal, not only time at breast. [9]
New parents often receive input from a variety of sources including family members, friends, and daycare providers as well as parent support groups and local service organizations like La Leche League [10] or Breastfeeding USA. [11]
But with all these different sources of information, there is risk of parents being overwhelmed by confusing or conflicting information, as well as myth and bias. Parents need educated support to help them evaluate the available information and resources so they can make informed decisions. Tow and Vallone (2009) assert that this role should ideally fall to the appropriately trained healthcare provider, the International Board Certified Lactation Consultant or IBCLC.
Despite the IBCLC being the most suitable portal of entry for breastfeeding education and support, a mother can potentially receive guidance at a variety of junctures: while still in the hospital by nursing or lactation support staff, incidentally at a routine well-baby follow up with nursing staff, well baby clinic or pediatrician check up due to failure to gain weight, in consultation with another provider because of past experience with a sibling or based on their reputation (taking their newborn to a chiropractor for breastfeeding difficulty), or due to an emergent condition requiring a trip to urgent care (a somnolent infant who cannot be roused). Although some of these professional interactions are with healthcare providers who have sought additional education or have experience in this arena, these interactions are often fraught with conflicting or misinformation which can lead to frustration and failure without seeking the support of an IBCLC.
Chiropractors should be most familiar with the diagnosis and treatment of musculoskeletal dysfunctions that could result in an inability to feed. The delicate balance required to nurse and transfer breast milk successfully is influenced by the functionality of the associated joints, soft tissue, and nerves of the cranium and cervical spine. Full, normal function may be negatively influenced by the neonateÆs innate ability to compensate for any ôroadblocksö it might encounter (ranging from neurologic and musculoskeletal implications of birth trauma to the presence of a tongue or lip tie). The chiropractor also needs to recognize and treat the compensatory changes that will develop in a healthy, neurotypical neonate when challenged by an inability to feed efficiently to prevent the evolution of long term physiologic and postural ramifications. [12-14]
A chiropractor may not be the first individual who will be positioned to support the breastfeeding dyad when challenges arise. Frequently, our role will be collaborative. Yet, with the increasing number of parents seeking early assessment by a chiropractor for their newborns [15-18] it behooves us to educate ourselves as to the differential diagnoses related to breastfeeding. This means the ability to identify the infant who cannot feed efficiently (or at all), is failing to thrive, or feeding in a compensatory pattern; and make referrals as appropriate. [19]
Other healthcare providers the chiropractor can expect to collaborate with when working with an infant who cannot feed include: IBCLCs, midwives, naturopaths, nurses, pediatricians, dentists, oral surgeons, pediatric surgeons, ear/nose/throat (ENT) surgeons or otolaryngologists, speech and language pathologists (SLP), occupational therapists (OT), oromyofunctional therapists (OMT), or other feeding or airway specialists who may play various roles in the care of the infant. Unfortunately, the parents may also be receiving conflicting information from these providers. When this happens, they are in even greater need for an advocate to help them create a plan of care for their infant to reduce the risk of premature cessation of breastfeeding.
When any one of these healthcare providers recognizes that the dyad is having breastfeeding challenges, an assessment should be performed including a system survey. The musculoskeletal examination (at which the chiropractor should be proficient) may reveal biomechanical dysfunction. For example, decreased range of motion of the joints of the cranium (like the temporomandibular joint) can interfere with a neonateÆs ability to gape comfortably and competently latch and transfer milk. Restricted cervical range of motion can result in discomfort or inability to latch with resultant behaviors like arching at the breast, crying in frustration, or pulling off the breast repeatedly. [20-29]
The collaborative protocol might include components of natural alternatives and/or holistic interventions based on the presenting diagnosis. Interventions may be straightforward and limited to chiropractic adjustments to restore normal joint function and neurologic competency or may be fraught with comorbidities and expand to include surgery (most often to release tethered oral tissues), [30, 31] supplementation to provide calories, rehabilitative exercises, pharmaceuticals, homeopathy and nutritional supplements to support gastrointestinal health and wound healing under the instruction of the IBCLC or other healthcare providers.
It would be helpful for the chiropractor to familiarize themselves with the prescribed interventions as well as the supportive measures to treat many of the comorbid conditions. Part of the chiropractorÆs role may be to help support the parents who have trepidation about recommended procedures. The chiropractor may also offer encouragement for parents having difficulty being compliant with protocols that may be required to help their infant attain competent feeding, ranging from a frequent pumping schedule to wound care and stretching after the revision of oral tethered tissues (lip, tongue, or buccal ties). The recognition that many of these interventions serve to prevent early cessation of breastfeeding [32] is critical but the chiropractor is ideally suited to evaluate and explain the implications of musculoskeletal dysfunction as it relates to current dysfunction as well as potential problems that could arise in the future if left unaddressed.
To underscore the importance of correcting altered oral motor function (whether structural, neurological, or mechanical), there has been an association with a wide variety of developmental issues. Some that have been (or are currently) under multidisciplinary exploration include failure to thrive, [33] airway dysfunction, SIDS, aerophagia (resulting in colic and reflux), [34] dental caries, [35] oral motor dysfunction, malocclusion, [36, 37] decreased patency of the sinuses, narrowed palatal architecture, snoring, sleep apnea and sleep disordered breathing, [38-40] disrupted immune function (including tonsillar hypertrophy), gastrointestinal dysfunction, and challenges in speech and articulation. [41, 42]
Physiologic function
There are far reaching effects because of the intimate relationship between the musculoskeletal and the nervous systems. Structure affects function and vice versa. Mechanical dysfunction can result in a lack of peripheral mechanoreceptor input to the central nervous system (CNS) which can influence a range of functions from the level of alertness to the modulation of visceral (mastication, swallowing, vomiting, peristalsis, glandular secretion, bladder control) and somatic (posture and general muscle tone) activities.
Local and global lack of mobility of the connective tissue (fascia) and articulations of the cranium, spine and extremities (due to injury, edema, adhesions, and compensations) can result in traction of the fascia which can also cause a mechanical barrier or alter afferent input to the CNS. [43]
Breathing and eating are the neonateÆs primary driving physiologic functions. The neurologically competent neonate will draw his or her first breath and seek the breast immediately when there is no interference. [44] If anything impedes the accomplishment of these initial goals, compensations will be developed as rapid plastic connections are made in the neonatal brain. This neuroplasticity assures survival under adverse conditions even at the expense of structural changes to achieve physiologic homeostasis. Even the neonate impaired by genetics, pharmaceutical intervention, or birth injury will frequently demonstrate this amazing ability to create compensatory neuronal pathways to accomplish these functions so basic to survival.
Structural interference impeding breathing may take other forms. For example, the use of the infant car restraint system, the ôbaby bucket,ö results in an infant positioned in a flexed posture who may not be able to inspire with sufficient capacity to supply the required oxygen to maintain sustainable pO2. Premature or impaired infants like those with posterior tongue ties may be at even higher risk. [45]

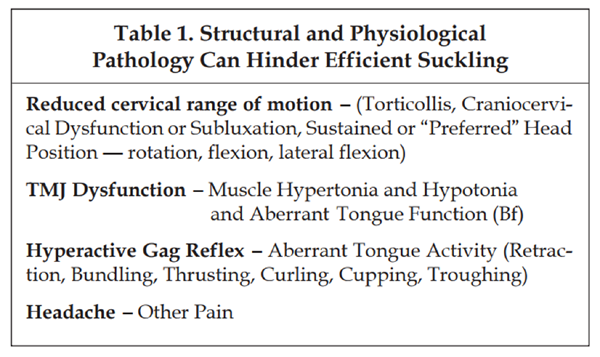
Table 1 The neonate uses six cranial nerves, 22 bones connecting at 34 sutures, and 60 voluntary and involuntary muscles in order to accomplish a smooth suck, swallow, breath sequence. [46] When the movement at any of these articulations is decreased or impeded, there is an associated cascade of movements that are influenced by the original mechanical dysfunction. Mechanical dysfunction (Table 1) can result in an immediate challenge to the neonateÆs ability to breathe and feed. Mechanical dysfunction that interferes with critical life sustaining activities (such as breathing and eating) also results in an engagement of the sympathetic nervous system. The sympathetic nervous system responds to low pO2 and the question, ôWhereÆs my next meal coming from?ö Accordingly, the brain rapidly creates new plastic circuits in an effort to urgently resolve the problem. Compensations ensue that may be functional or dysfunctional. In the short term, the impact of these compensations on respiratory function, milk transfer, the infantÆs sleep patterns, and maternal stress level may be significant. Compensatory patterns may have long term effects as previously outlined.
Mechanical dysfunction also prompts nociceptive input to the central nervous system. Nociception (pain) via the spinoreticular tract can result in activation of the sympathetic nervous system (via the amygdala and the thalamus) with an associated exaggeration of infantile reflexes; altered respiration and infant sleep patterns; increased difficulty integrating sensory input; decreased digestion; and increased irritability û all manifestations of autonomic dysregulation.
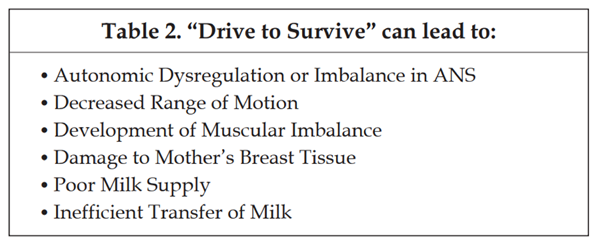
Table 2 An unmedicated neurotypical neonate will seek his motherÆs breast for nourishment if left to his own devices. In utero constraint, a difficult labor and delivery, and interventions û both non emergent and emergent û employed during a home birth or in a hospital setting may thwart the neonateÆs ability to nurse by altering normal biomechanical function and perhaps development (Table 2). The most direct way to effect immediate change for the neonate is to address any neuromusculoskeletal problems impeding normal function. The level of intervention will depend on the level of complexity of the dysfunction. The earlier the intervention, the greater the chance of attaining competency.
The History
A thorough history and evaluation will facilitate management (including appropriate referrals) for your patient. From learning the details of the birth to recognizing key posturing or head position, a detail-oriented approach is critical. Specific questions are designed to elicit specific information about the breastfeeding relationship.
Table 3
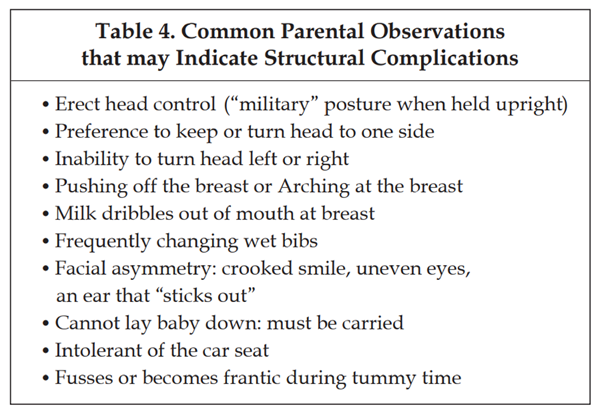
Table 4 To determine appropriate management, every practitioner who interfaces with the dyad needs to look at form and function through a discerning lens and differentiate neuromusculoskeletal from other issues (Table 3). Chiropractors need to take into account the observations of the parents and caregivers who will often describe alterations in function in minute detail (Table 4).
The Exam
Examine the infant layer by layer. Indulge in observation and know that books exist to name things. A full assessment of all systems should be routinely performed with special attention given to neuromusculoskeletal integrity. Neurologic responsiveness, reflexes, and muscle tone should be assessed as well as the soft tissue structures (including skin turgor, color and temperature, fascial tension, and development of muscle mass); osseous structures to rule out fracture or displacement; and articulations to rule out hyper or hypomobility of the joints, capsular swelling, and muscle symmetry surrounding the joint.
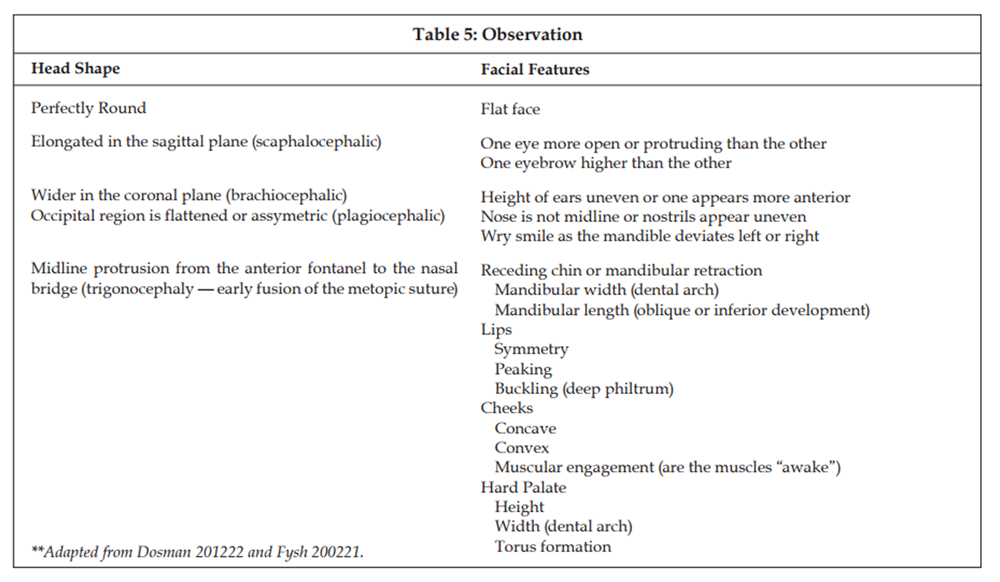
Table 5 Visual assessment (Table 4) as well as passive palpation can reveal many clues to the cause of the breastfeeding dysfunction. For example, reflexes like rooting and suckling can be stimulated digitally or, in a homebirth, simply observed while the neonate is lying prone across the motherÆs chest and abdomen. A neurotypical neonate will spontaneously commando crawl (stepping reflex), root, latch, and suckle while palming the breast (Babkin) without assistance. Even the initial assessment of the suck, swallow, breath synchrony47 can be performed by observing and listening, If the neonate is unable to do this unassisted, a chiropractic examination may reveal the cause (Table 5).
Conclusion
When evaluating an infant with breastfeeding dysfunction a ôwhole childö approach needs to be adopted as there are many factors that could interfere with successful latch and transfer including injured muscles, fractured clavicle, hip dysplasia, neurologic interference from an anoxic event, or an extended half-life of an administered medication. Although supplementation by bottle may be possible (whether with breastmilk or an artificial milk replacement), it may prove to be just as challenging for the impaired neonate and ultimately more serious interventions like a nasogastric tube could be necessary.
Diligent evaluation and differential diagnosis are critical in the neonate who is having difficulty feeding. A collaborative effort between chiropractors and other health care providers while utilizing an IBCLC for primary breastfeeding evaluation and support is often the most efficacious means to restoring competency for the breastfeeding dyad.
References:
The World Health OrganizationÆs infant feeding recommendation.
Accessed 2015 September. Retrieved from:
www.who.int/nutrition/topics/infantfeeding_recommendation/en/.Breastfeeding among U.S. Children Born 2002û2012,
CDC National Immunization Surveys.
Accessed 2016 February. Retrieved from:
http://www.cdc.gov/breastfeeding/data/NIS_data/.Breastfeeding Report Card Progressing Toward National Breastfeeding Goals United States, 2016
Patel S and Patel S.
The Effectiveness of Lactation Consultants and Lactation Counselors on Breastfeeding Outcomes.
J Hum Lact. 2015 Dec 7. pii: 0890334415618668. [Epub ahead of print].Horta BL and Victoria CG.
Long-term effects of breastfeeding: a systematic review.
World Health Organization 2013. Retrieved from:
http://apps.who.int/iris/bitstream/10665/79198/1/9789241505307_eng.pdfChiurco A et al.
An IBCLC in the Maternity Ward of a Mother and Child Hospital: A Pre- and Post-Intervention Study.
Int J Environ Res Public Health 2015 Aug; 12(8): 9938û9951.sss.Neifert MR.
Prevention of breastfeeding tragedies
Pediatr Clin North Am 2001 April; 48(2):273-297.Krugman SD and Dubowitz H.
Failure to thrive
Am Fam Physician 2003 Sep ;68(5):879-884.Kent JC1 , Prime DK, Garbin CP.
Principles for maintaining or increasing breast milk production.
J Obstet Gynecol Neonatal Nurs 2012 JanFeb;41(1):114-21.La Leche League International.
Accessed 2015 December. Retrieved from:
http://www.llli.org/Breastfeeding USA.
Accessed on 2015 December. Retrieved from:
https://breastfeedingusa.org/Tow J and Vallone SA.
Development of and integrative relationship in the care of the breastfeeding newborn: Lactation consultant and chiropractor.
J Clin Chiropr Pediatr 2009 June; 10(1).626-632.Lavigne, V.
A narrative review and case report: frenotomy procedure in neonate with tongue-tie.
J Clin Chiropr Pediatr 2012 Dec; 13(2).1025-1031.Fry LM.
Chiropractic and Breastfeeding Dysfunction: A Literature Review
Journal of Clinical Chiropractic Pediatrics 2014 (Mar); 14 (2): 1151-1155Gleberzon, BJ, Arts, J, Mei, A, and McManus, EL.
The Use of Spinal Manipulative Therapy For Pediatric Health Conditions:
A Systematic Review of the Literature
J Can Chiropr Assoc. 2012 (Jun); 56 (2): 128û141Miller J.
Demographic Survey of Pediatric Patients Presenting to
a Chiropractic Teaching Clinic
Chiropractic & Osteopathy 2010 (Dec 15); 18: 33Miller J.
Cry babies: a framework for chiropractic care.
Clin Chiropr 2007; 10:139-146.Black, LI, Clarke, TC, Barnes, PM, Stussman, BJ, and Nahin, RL.
Use of Complementary Health Approaches Among Children Aged
4û17 Years in the United States: National Health
Interview Survey, 2007û2012
National Health Statistics Report 2015 (Feb 10); (78): 1û19Watson Genna, C.
Supporting Sucking Skills in Breastfeeding Infants.
Boston: Jones and Bartlett Publishers; 2008.Holleman, A. C., Nee, J., & Knaap, S. F.
Chiropractic Management of Breast-feeding Difficulties: A Case Report
Journal of Chiropractic Medicine 2011 (Sep); 10 (3): 199û203Vallone S.
Chiropractic Evaluation and Treatment of Musculoskeletal Dysfunction
in Infants Demonstrating Difficulty Breastfeeding
J Clinical Chiropractic Pediatrics 2004 (Dec); 6 (1): 349û366Alcantara J and Anderson R.
Chiropractic care of a pediatric patient with symptoms associated with gastroesophageal reflux disease, fusscry-irritability with sleep disorder syndrome and irritable infant syndrome of musculoskeletal origin.
J Can Chiropr Assoc 2008 Dec; 52(4), 248-255.Hewitt E.
Chiropractic care for infants with dysfunctional nursing: a case series.
J Clin Chiropr Pediatr 1999;4(1):241û244.Holleman A et al.
Chiropractic management of breast-feeding difficulties: a case report.
J Chiropr Med 2011 Sep;10(3), 199-203.Holtrop D.
Resolution of suckling intolerance in a 6-month-old chiropractic patient.
J Manipulative Physiol Ther 2000 Nov-Dec; 23(9), 615-618.Miller, J. E., Miller, L., Sulesund, A. K., & Yevtushenko, A.
Contribution of Chiropractic Therapy to Resolving Suboptimal Breastfeeding:
A Case Series of 114 Infants
J Manipulative Physiol Ther 2009 (Oct); 32 (8): 670û674Miller J, Newell D, Bolton J.
Efficacy of Chiropractic Manual Therapy on Infant Colic:
A Pragmatic Single-Blind, Randomized Controlled Trial
J Manipulative Physiol Ther. 2012 (Oct); 35 (8): 600û607Holleman AC et al.
Chiropractic management of breast-feeding difficulties: A case report.
J Chiropr Med 2011 Sep; 10(3):199-203.Drobbin D and Stallman J.
Resolution of breastfeeding and latching difficulty following subluxation based chiropractic care: case report and review of the literature.
J Pediatr Matern & Fam Health - Chiropr 2015(3),02-108.Coryllos E et al. (2004).
Congenital tongue-tie and its impact on breastfeeding.
American Academy of Pediatrics Newsletter.(Summer), 1-5.Kotlow, L. (2011).
Diagnosis and treatment of ankyloglossia and tied maxillary fraenum in infants using Er:YAG and 1064 diode lasers.
Eur Arch Paediatr Dent 2011 Apr;12(2):106-12.OÆCallahan C et al.
The effects of office-based frenotomy for anterior and posterior ankyloglossia on breastfeeding.
Int J Pediatr Otorhinolaryngol 2013 May; 77(5):827-32.Forlenza GP et al.(2010).
Ankyloglossia, Exclusive Breastfeeding, and Failure to Thrive.
Pediatrics 2010 Jun;125(6):e1500-4.Kotlow L
Infant reflux and aerophagia associated with the maxillary lip-tie and ankyloglossia (tongue-tie).
Clinical Lactation, (2011), Vol. 2-4, 25-29.Kotlow LA.
The influence of the maxillary frenum on the development and pattern of dental caries on anterior teeth in breastfeeding infants: prevention, diagnosis, and treatment.
J Hum Lact 2010 Aug; 26(3), 304-308.Saccomanno S et al.
Causal relationship between malocclusion and oral muscles dysfunction: a model of approach.
Eur J Paediatr Dent 2012 Dec;13(4):321-323.Mukai S and Nitta N.
Correction of the Glosso-larynx and Resultant Positional Changes of the Hyoid Bone and Cranium.
Acta Otolaryngol 2002 Sep;122(6):644-50.Palmer B.
Breastfeeding: Reducing the Risk for Obstructive Sleep Apnea.
Breastfeeding Abstracts (LLLI), February 1999; 18(3):19-20.
Accessed 2015 December. Retrieved from:
http://www.llli.org/ba/feb99.html .Levrini L et al.
Model of oronasal rehabilitation in children with obstructive sleep apnea syndrome undergoing rapid maxillary expansion: Research review.
J Sl Sci 2014; (7)225-233.Ruoff C and Guilleminault C.
Orthodontics and sleep-disordered breathing. Editorial.
Sleep Breath, 2012 16 (2). 271-273.Dollberg, S., Manor, Y., Makai, E., & Botzer, E. (2011).
Evaluation of speech intelligibility in children with tongue-tie.
Acta Paediatr 2011 Sep;100(9), 125-7.Ito Y et al. (2015).
Effectiveness of tongue-tie division for speech disorder in children.
Pediatr Int 2015 Apr; 57(2), 222-226. doi: 10.1111/ped.12474.Schleip R.
Fascial plasticity û a new neurobiological explanation.
J Bodyw Mov Ther 2003 Jan; 7(1):11-19 and 7(2):104-116.Watson Genna, C.
Supporting Sucking Skills in Breastfeeding Infants.
Boston: Jones and Bartlett Publishers; 2008.Bull M and Engle W.
Safe Transportation of Preterm and Low Birth Weight Infants at Hospital Discharge.
Pediatrics 2009 May. 123; 1424-1429.Smith, LJ.
Impact of birthing practices on the breastfeeding dyad.
J Midwifery Womens Health 2007 Nov-Dec;52(6):621-30.Sakalidis V. and Geddes D.
Suck-Swallow-Breathe Dynamics in Breastfed Infants.
J Hum Lact. 2015 Aug 28. pii: 0890334415601093. [Epub ahead of print].
Return to PEDIATRICS
Since 11-21-2017

| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |