

Management of Neck Pain and Associated Disorders:
A Clinical Practice Guideline from the Ontario Protocol
for Traffic Injury Management (OPTIMa) CollaborationThis section was compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: European Spine Journal 2016 (Jul); 25 (7): 2000–2022 ~ FULL TEXT
Côté P, Wong JJ, Sutton D, Shearer HM, Mior S, Randhawa K, Ameis A, Carroll LJ, Nordin M,
Yu H, Lindsay GM, Southerst D, Varatharajan S, Jacobs C, Stupar M, Taylor-Vaisey A,
van der Velde G, Gross DP, Brison RJ, Paulden M, Ammendolia C, David Cassidy J, Loisel P,
Marshall S, Bohay RN, Stapleton J, Lacerte M, Krahn M, Salhany R
Canada Research Chair in Disability Prevention and Rehabilitation,
University of Ontario Institute of Technology (UOIT),
2000 Simcoe Street North,
Oshawa, ON, L1H 7L7, Canada.
pierre.cote@uoit.ca
PURPOSE: To develop an evidence-based guideline for the management of grades I-III neck pain and associated disorders (NAD).
METHODS: This guideline is based on recent systematic reviews of high-quality studies. A multidisciplinary expert panel considered the evidence of effectiveness, safety, cost-effectiveness, societal and ethical values, and patient experiences (obtained from qualitative research) when formulating recommendations. Target audience includes clinicians; target population is adults with grades I-III NAD <6 months duration.RECOMMENDATION 1: Clinicians should rule out major structural or other pathologies as the cause of NAD. Once major pathology has been ruled out, clinicians should classify NAD as grade I, II, or III.
RECOMMENDATION 2: Clinicians should assess prognostic factors for delayed recovery from NAD.
RECOMMENDATION 3: Clinicians should educate and reassure patients about the benign and self-limited nature of the typical course of NAD grades I-III and the importance of maintaining activity and movement. Patients with worsening symptoms and those who develop new physical or psychological symptoms should be referred to a physician for further evaluation at any time during their care.
RECOMMENDATION 4: For NAD grades I-II ≤3 months duration, clinicians may consider structured patient education in combination with: range of motion exercise, multimodal care (range of motion exercise with manipulation or mobilization), or muscle relaxants. In view of evidence of no effectiveness, clinicians should not offer structured patient education alone, strain-counterstrain therapy, relaxation massage, cervical collar, electroacupuncture, electrotherapy, or clinic-based heat.
RECOMMENDATION 5: For NAD grades I-II >3 months duration, clinicians may consider structured patient education in combination with: range of motion and strengthening exercises, qigong, yoga, multimodal care (exercise with manipulation or mobilization), clinical massage, low-level laser therapy, or non-steroidal anti-inflammatory drugs. In view of evidence of no effectiveness, clinicians should not offer strengthening exercises alone, strain-counterstrain therapy, relaxation massage, relaxation therapy for pain or disability, electrotherapy, shortwave diathermy, clinic-based heat, electroacupuncture, or botulinum toxin injections.
RECOMMENDATION 6: For NAD grade III ≤3 months duration, clinicians may consider supervised strengthening exercises in addition to structured patient education. In view of evidence of no effectiveness, clinicians should not offer structured patient education alone, cervical collar, low-level laser therapy, or traction.
RECOMMENDATION 7: For NAD grade III >3 months duration, clinicians should not offer a cervical collar. Patients who continue to experience neurological signs and disability more than 3 months after injury should be referred to a physician for investigation and management.
RECOMMENDATION 8: Clinicians should reassess the patient at every visit to determine if additional care is necessary, the condition is worsening, or the patient has recovered. Patients reporting significant recovery should be discharged.Keywords Clinical practice guideline, Neck pain, Treatment, Management, Practice guideline, Therapies, Therapy, Disease management, Whiplash
From the FULL TEXT Article:
Introduction
Background
More than 80 % of individuals experience neck pain and associated disorders (NAD) during their lifetime, with 30–50 % of the general adult population reporting neck pain annually. [1, 2] The course of neck pain is favorable for most people; however, 23 % of individuals who recover from an episode of neck pain will experience a subsequent episode. [3]
For many patients, neck pain is a complex biopsychosocial disorder with problematic physical and psychological symptoms. Neck pain is associated with decreased health-related quality of life, decreased work productivity, daily activity limitations, and increased healthcare utilization. [2, 4–6]
In the United States, approximately 10.2 million visits are made annually to physician offices and hospital outpatient departments for neck pain. [7] In 2010, neck pain ranked fourth among all conditions contributing to years lived with disability. [8] NAD that results from motor vehicle collisions is commonly known as whiplash-associated disorders (WAD). [8] In Canada, 86.2 % of people injured in motor vehicle collisions develop NAD. [6] Recovery from NAD can be prolonged and associated with high health resource use. [10, 11] Costs related to managing this condition are substantial due to medical costs and costs associated with productivity changes. [5, 12]
The clinical management of NAD is often challenging. Recommendations from clinical practice guidelines aim to inform clinical practice. However, the quality of current clinical practice guidelines varies [13], and recommendations that are not evidence-based cannot be relied upon to reduce symptoms or facilitate patient recovery. An up-todate, high quality evidence-based clinical practice guideline is needed to inform the management of NAD grades I–III.
Scope and purpose of the guideline

Table 1 We used the best available evidence to develop a clinical practice guideline for the management of NAD grades I–III (including WAD) of less than 6 months duration (Table 1). NAD includes non-traumatic, traumatic, or work-related neck pain. The target population is adults (18 years of age or older) with recent-onset (0–3 months duration) and persistent (4–6 months duration) NAD grades I–III; it does not cover NAD that persists for more than 6 months. The management of NAD grade IV is beyond the scope of this guideline because it refers to significant pathology that may require invasive/surgical interventions. The target audience for the current guideline includes clinicians (medical doctors, physiotherapists, nurse practitioners, chiropractors, kinesiologists, psychologists, and massage therapists) caring for patients with neck pain in primary, secondary, and tertiary health care settings.
This guideline aims to:(1) accelerate recovery
(2) reduce the intensity of symptoms
(3) promote early restoration of function
(4) prevent chronic pain and disability
(5) improve health related quality of life
(6) reduce recurrences and
(7) promote active participation of patients in their care.Moreover, this guideline aims to promote uniform high quality care for individuals with NAD.
The guideline was developed by the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration, which is a multidisciplinary team of expert clinicians (from medicine, dentistry, physiotherapy, chiropractic, psychology, occupational therapy, and nursing disciplines), academics and scientists (epidemiologists, clinical epidemiologists, library sciences, and health economists), a patient liaison, a consumer representative, a retired judge, and automobile insurance industry experts. The OPTIMa Collaboration was mandated by the Ontario Ministry of Finance and the Financial Services Commission of Ontario to develop an evidence-based clinical practice guideline for neck pain and its associated disorders.
Methods
Systematic reviews
We updated the systematic reviews from the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders (Neck Pain Task Force). [14] This update included eight systematic reviews examining the effectiveness, cost-effectiveness, and safety of non-invasive interventions for the management of NAD grades I–III. [15–22] All systematic reviews were registered with the International Prospective Register of Systematic Reviews (PROSPERO). [23]
The systematic reviews included studies examining the effectiveness of non-invasive interventions for the management of NAD grades I–III (Table 1; Appendix). [15–22] We excluded studies on the management of grade IV NAD (e.g., fractures, dislocations, neoplasms, inflammatory diseases).
Non-invasive interventions included acupuncture, exercise, manual therapy, passive physical modalities, psychological interventions, soft tissue therapy, structured patient education, multimodal care, analgesics, non-steroidal anti-inflammatory drugs (NSAIDs), and muscle relaxants (Appendix I).
Eligible comparators included other interventions, placebo/sham interventions, non-intervention effects associated with wait listing, or no intervention.
Eligible outcomes included selfrated recovery, functional recovery, disability, pain intensity, health-related quality of life, psychological outcomes, or adverse events.
We considered randomized controlled trials (RCTs), cohort studies, and case–control studies published in English. Only full economic evaluations that jointly analyzed costs and health outcomes were eligible for inclusion in the cost-effectiveness review.
We searched MEDLINE, EMBASE, PsycINFO, and Cochrane Central Register of Controlled Trials through Ovid Technologies, Inc., and CINAHL Plus with Full Text through EBSCOhost (Appendix IIA and IIB). We also searched EconLit through ProQuest, Health Technology Assessment (Cochrane), and National Health Service Economic Evaluation Database (Cochrane) for economic evaluations. Our initial searches included publication dates from January 1990 to January 2015 (search dates varied between reviews). In May 2015, we updated all searches in MEDLINE to retrieve recent RCTs, full economic evaluations, or systematic reviews.
Random pairs of independent, trained reviewers screened and critically appraised eligible studies using the Scottish Intercollegiate Guidelines Network (SIGN) criteria. [25] Low risk of bias studies were included in the evidence synthesis. [26] Low risk of bias studies were defined as studies where selection bias, information bias, and confounding were deemed unlikely by two independent reviewers to have threatened the internal validity of the study. Minimal clinically important difference thresholds from the literature were used to determine the clinical importance of the results between groups from low risk of bias studies. [27–30]
Development of recommendations
The principle of patient-centered care was fundamental to the development of this guideline. We developed the evidence-based recommendations according to:
Key decision determinants [overall clinical benefit (effectiveness and safety),
value for money (i.e., costeffectiveness data when available), and consistency
with expected societal and ethical values] based on the Ontario Health Technology
Advisory Committee framework. [31]Best evidence obtained from critical review of scientific literature and
Findings from qualitative research exploring the experiences of persons
treated for traffic injuries in Ontario. [32] These findings on patient
experiences were considered under the key decision determinant
‘expected societal and ethical values.’
Table 2 All systematic reviews were reviewed and approved by a multidisciplinary Guideline Expert Panel that included 21 individuals representing emergency medicine, internal medicine, rehabilitation medicine, orthopedic surgery, dentistry, chiropractic, physical therapy, psychology, nursing, health economics, epidemiology, clinical epidemiology, law, patient liaison, consumer representative, and insurers (non-voting members). The translation of scientific evidence into guideline recommendations followed five steps (Table 2). Recommended interventions were supported by evidence of effectiveness from studies with low risk of bias, and where available, by evidence of benefits outweighing harm to patients. When evidence was sparse (e.g., red flags or pharmacological treatments for neck pain), the Guideline Expert Panel used evidence from the low back pain literature to inform its recommendations.
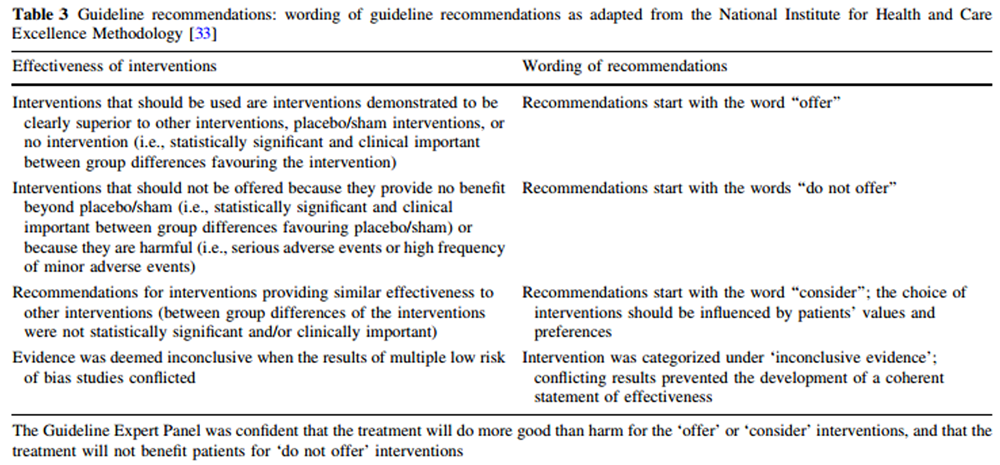
Table 3 This guideline adapted the National Institute for Health and Care Excellence methodology to develop the wording of guideline recommendations (Table 3). [33]
Based on this methodology, recommendations start with the word‘‘offer’’ (for interventions that are of superior effectiveness compared to other interventions,
placebo/sham interventions, or no intervention),
‘‘consider’’ (for interventions providing similar effectiveness to other interventions), or
‘‘do not offer’’ (for interventions providing no benefit beyond placebo/sham or are harmful).An intervention was deemed to have superior effectiveness if evidence of statistically significant and clinically important benefits was identified in at least one RCT with a low risk of bias.
The frequency and duration of interventions was included in the recommendations. This was determined by averaging or by reporting treatment frequencies and durations of care for interventions that were effective. [15, 16] Specifically, for recommended interventions that were supported by one low risk of bias RCT, we used the frequency and duration of treatment that were tested in that RCT. For recommended interventions that were based on more than one low risk of bias study, we computed the mean frequency and duration of care across studies with superior outcomes for a specific intervention.
Each recommendation was integrated into care pathways, which were approved by the Guideline Expert Panel (Figures 1, 2, 3, 4). Interventions for which there is inconclusive evidence of effectiveness were not included in the care pathways (Appendix III).
The applicability (e.g., facilitators, barriers, resource implications, dissemination, implementation) of this guideline is beyond the scope of this project because it was developed for the Government of Ontario. The Government will determine its applicability to the Ontario automobile insurance and healthcare system. It is recommended that this guideline be updated in 5 years so that the guideline is based on current evidence. [34] The update should use methodology similar to the development of this guideline.
External review
This evidence-based clinical practice guideline was developed for the Government of Ontario. The Government invited stakeholders to review and comment on the guideline. Moreover, the government held a series of public consultations on the clinical practice guideline from August 17–21, 2015.
Recommendations
All recommended interventions are supported by evidence of effectiveness, safety, cost-effectiveness (when cost-effectiveness data were available), and are consistent with societal and ethical values. Interventions that are not recommended did not satisfy the criteria of one or more key decision determinants (i.e., evidence of effectiveness, safety, cost-effectiveness, and/or consistency with societal and ethical values).
Recommendation 1: Evaluation of NAD
Clinicians should rule out major structural or other pathologies as the cause of NAD.
Clinicians should classify NAD as grade I, II, or III.
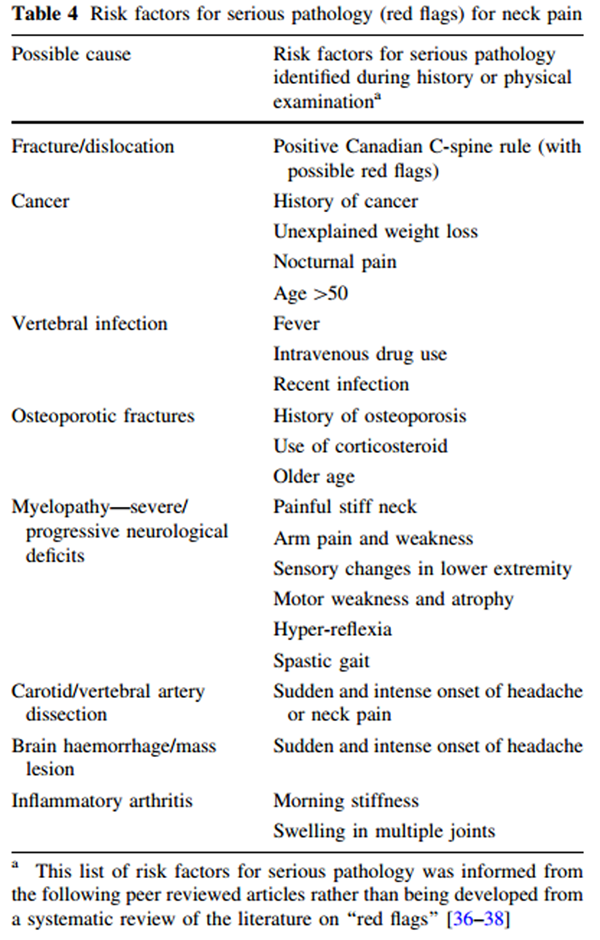
Table 4 Clinicians should conduct a clinical evaluation to rule out major structural or other pathologies (NAD grade IV) as the cause of signs and symptoms. The Canadian C-spine Rule should be used to rule out cervical spine fractures and dislocations associated with acute trauma (Appendix IV). [35] The Canadian C-spine Rule was designed and validated for use in emergency departments, and can be used in acute care settings. The presence of risk factors for serious pathologies (also termed ‘red flags’) identified during the history/examination warrants further investigation and referral to the appropriate healthcare professional ( Table 4 ). [36–38] As there is a paucity of literature on red flags for neck pain, the list of red flags was informed by the low back pain literature. [36–38]
Clinicians should assess for neurological signs
(decreased deep tendon reflexes, muscle weakness, sensory deficits).
NAD III refers to neck pain associated with clear clinical evidence of neurologic signs
(decreased deep tendon reflexes, weakness, or sensory deficits) on physical examination.
Once major pathology has been ruled out, clinicians should classify the grade of NAD as grade I, II, or III; as recent or persistent; and the patient should receive the appropriate evidence-based interventions (Figures 1, 2).
Recommendation 2: Prognostic factors for delayed recovery
Clinicians should assess prognostic factors for delayed recovery from NAD (Appendix V). Most patients will recover. Patients with NAD grade I can be expected to recover more quickly, while those with NAD grade III are expected to recover more slowly. [11, 24, 39–42]
Patients with the following prognostic factors may have a higher risk
for delayed recovery [11, 24, 39–42]:
Demographic factors: older age.
Physical health: prior history of neck pain; high levels of initial pain; and high levels of initial disability.
Psychological factors following a traffic collision: poor expectation of recovery,
symptoms of acute stress disorders (symptoms exhibited within 4 weeks of injury), symptoms of post-traumatic stress disorder (symptoms lasting at least 4 weeks); depressed mood or feelings of depression about pain, anxiety or fear about pain, high levels of frustration or anger about the pain, passive coping, kinesiophobia, avoiding activities due to fear of pain.
Recommendation 3: Management of NAD
Clinicians should educate and reassure patients about the benign and self-limited nature of the typical course of NAD grades I–III and the importance of maintaining activity and movement. Patients with worsening symptoms and those who develop new physical or psychological symptoms should be referred to a physician for further evaluation at any time during their care.
For NAD grades I–III, clinicians should provide care in partnership with the patient and involve the patient in care planning and decision-making. Clinicians should reassure patients that, in the majority of cases, NAD is benign and has a self-limited course. Patients should be educated about the benefits of being actively engaged and participating in their care plan by remaining active and maintaining movement of their neck. Clinicians should emphasize active rather than passive treatments and deliver timelimited care that includes effective interventions. [15–17, 43, 44]
Recommendation 4: Management of recent NAD
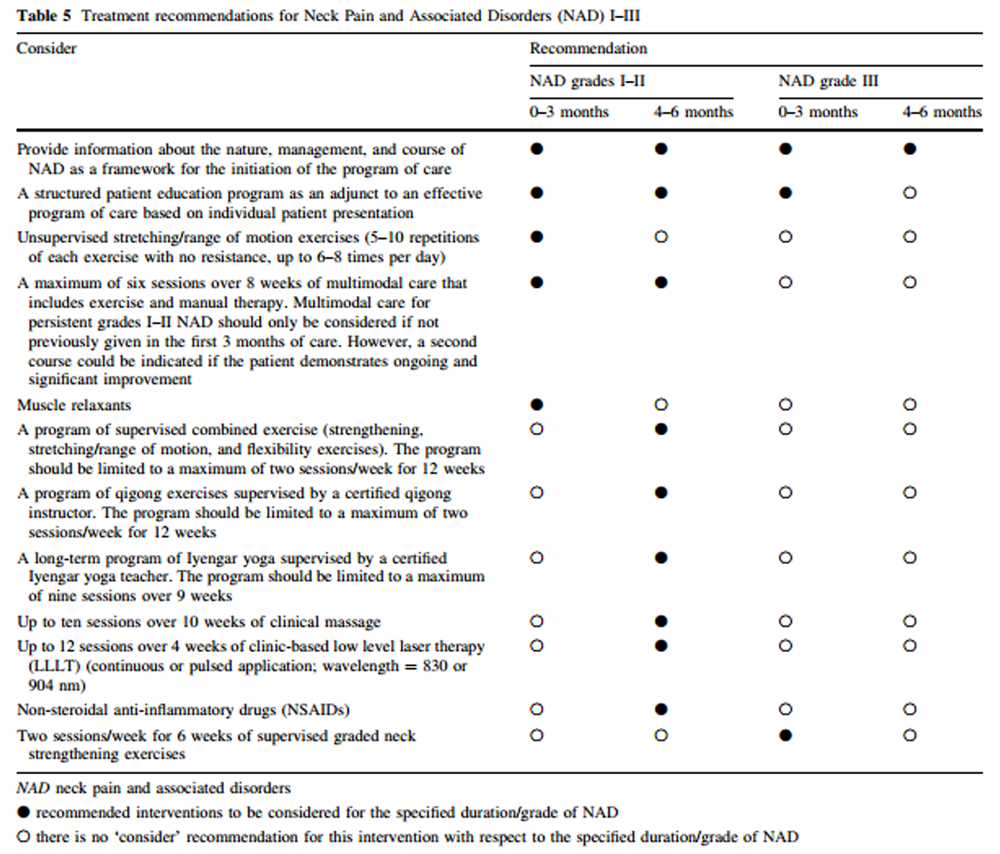
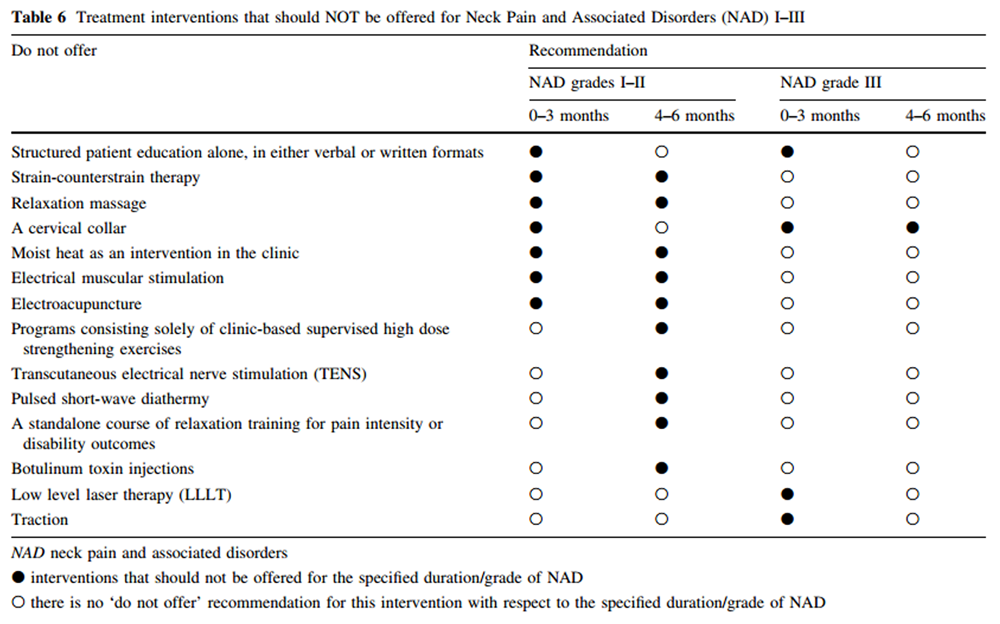
Table 5
Table 6 Grades I–II (Table 5, Table 6; Figures 1, 2) For patients with NAD grades I–II B3 months duration, clinicians may consider structured patient education in combination with: range of motion exercise, multimodal care (range of motion exercise with manipulation or mobilization), or a short course of muscle relaxants (as indicated). In view of evidence of no effectiveness, clinicians should not offer structured patient education alone, strain-counterstrain therapy, relaxation massage, cervical collar, electroacupuncture, electrotherapy, or clinic-based heat.
Structured patient education Clinicians should provide information about the nature, management, and course of NAD as a framework for initiating the program of care. This recommendation is based on universal principles of health professions’ standards of practice wherein patients are informed and educated about their condition, and participate in the decision-making process. [45]
Clinicians should not offer structured patient education alone. [17, 46] This recommendation is based on one low risk of bias RCT suggesting that although structured education was less costly than multimodal care, it was also less effective than multimodal care. [17, 46]
However, clinicians can consider a structured patient education program as an adjunct to an effective program based on individual patient presentation. [17, 46–48] The structured education should focus on providing advice to stay active and reassuring the patient by addressing expectations of recovery. This recommendation is based on three low risk of bias RCTs suggesting that:(1) a course of physiotherapy including self-care advice is more effective than one session
of oral advice in improving the recovery of patients [17, 46]; and
(2) an educational video combined with usual emergency care may be more effective than
usual emergency care alone in reducing neck pain for recent WAD. [17, 47, 48]Exercise Clinicians may consider range of motion exercises (5–10 repetitions with no resistance, up to 6–8 times per day). [15, 49] This involves unsupervised and gentle daily home-based controlled range of motion exercises of neck and shoulder, including neck retraction, extension, flexion, rotation, lateral bending, and scapular retraction. The exercise program should be taught to the patient by a healthcare professional. This recommendation is based on one low risk of bias RCT that found similar outcomes between home exercise and advice, medication, and manual therapy for recent NAD I–II. [49]
Multimodal care Clinicians may consider a maximum of six sessions over 8 weeks of multimodal care that includes range of motion exercise and manual therapy (manipulation or mobilization to the cervical and/or thoracic spine as clinically indicated). [16] This recommendation is based on our systematic review [16] that identified 14 low risk of bias RCTs examining the effectiveness of multimodal care for NAD. [46, 49–64]
This body of evidence suggests that the effective multimodal programs of care included exercise, manual therapy, and education. [16] On average, effective multimodal care was achieved within six visits over 8 weeks. [16] Cost-effectiveness data suggest that exercise and manual therapy is more cost-effective than two other programs of multimodal care (i.e., a program with exercise, traction, soft tissue therapy, and passive physical modalities or a program with advice and analgesics). [65]
Soft tissue therapy Clinicians should not offer straincounterstrain therapy (Glossary—Appendix VI).[21] This recommendation is based on two low risk of bias RCTs suggesting that:(1) ischemic compression and straincounterstrain therapy provided no added benefit
to muscle energy technique for improving neck pain, motion and disability in the short-term
for recent NAD [21, 66] and
(2) strain-counterstrain therapy is not more effective than sham
strain-counterstrain therapy in the short-term.[21, 67]Clinicians should not offer relaxation massage to treat recent onset NAD (Glossary—Appendix VI).[21] This recommendation is based on one low risk of bias RCT suggesting that relaxation massage was less effective than sham laser acupuncture or acupuncture for NAD of variable duration.[21, 68]
Passive physical modalities Clinicians should not offer a cervical collar. [21] This recommendation is based on three low risk of bias RCTs suggesting that collars provide less benefit than advice or active mobilization alone and similar benefit to receiving no care. [21, 69–72]
Similarly, clinicians should not offer electrical muscle stimulation or moist heat as an intervention in the clinic. [21] This recommendation is based on one low risk of bias RCT suggesting that electrical muscle stimulation or moist heat provided no additional benefit to a course of spinal manipulation or mobilization. [21, 73]
Acupuncture Clinicians should not offer electroacupuncture. [21] This recommendation is based on one low risk of bias RCT that found similar outcomes between electroacupuncture and simulated acupuncture for WAD of variable duration. [21, 74] The evidence for needle acupuncture was inconclusive (Appendix III).
Medication The non-opioid first ‘step’ in the World Health Organization analgesic ladder includes non-steroidal anti-inflammatory drugs (NSAIDs), muscle relaxants and acetaminophen. [75] Notwithstanding the prevalence and readily available nature of these over-the-counter (OTC) drugs, there is remarkably little evidence to support a clinical prescription decision for any of these drugs for NAD. This is particularly true for acetaminophen, for which the best available evidence does not indicate that acetaminophen is an effective analgesic for NAD and spinal pain [20, 76, 77]; therefore, acetaminophen should not be recommended or prescribed as a routine intervention.
There was insufficient evidence for any clinical prescription decision concerning NSAIDs for NAD and spinal pain. [18]
Evidence suggests that clinicians may consider a short course of muscle relaxants (cyclobenzaprine). [20] This recommendation is based on one low risk of bias RCT suggesting that use of an oral muscle relaxant may be more effective than placebo. [78] Paradoxically, the evidence suggests that analgesia, rather than muscle relaxation, is the primary therapeutic benefit. Prolonged use is not warranted.
There is evidence that significant adverse effects are associated with use of muscle relaxants; therefore, patient education about the side effects and close monitoring are warranted. [20] There is no evidence of differential effectiveness for the various muscle relaxant drugs. [20] There is no evidence that combining muscle relaxants with other medications provides added benefit. [20]
Recommendation 5: Management of persistent NAD
Grades I–II (Table 5, Table 6; Figures 1, 2) For patients with NAD grades I–II NAD [3 months duration, clinicians may consider structured patient education in combination with: range of motion and strengthening exercises, qigong, yoga, multimodal care (exercise with manipulation or mobilization), clinical massage, low-level laser therapy, or non-steroidal antiinflammatory drugs. In view of evidence of no effectiveness, clinicians should not offer strengthening exercises alone, strain-counterstrain therapy, relaxation massage, relaxation therapy for pain or disability, electrotherapy, shortwave diathermy, clinic-based heat, electroacupuncture, or botulinum toxin injections.
Structured patient education As described above, clinicians should provide information about the nature, management, and course of NAD as a framework for initiating the program of care. This recommendation is based on two low risk of bias studies suggesting that:(1) structured advice alone offers similar outcomes to physiotherapy-based graded exercises
with structured advice [17, 79] and
(2) a self-management program based on an educational booklet may be as effective as
multimodal physical therapy. [17, 56]
Exercise Clinicians may offer a program of supervised combined exercise (range of motion and strengthening exercises) limited to a maximum of two sessions per week for 12 weeks. [15] This recommendation is based on two low risk of bias RCTs in which supervised combined strengthening and range of motion exercises offered greater benefit than being randomized to wait list. [15, 80, 81]
Clinicians may offer a program of qiqong exercises (Glossary—Appendix VI) supervised by a certified qigong instructor, limited to a maximum of two sessions per week for 12 weeks. [15] This recommendation is based on two low risk of bias RCTs in which qigong offered greater benefit than waitlist. [15, 80, 81]
Clinicians may offer a program of Iyengar yoga (Glossary—Appendix VI) supervised by a certified Iyengar yoga teacher, limited to a maximum of nine sessions over 9 weeks. [15] This recommendation is based on one low risk of bias RCT that found Iyengar yoga offered greater benefit than education and a home exercise program. [15, 82]
Clinicians should not offer an exercise program consisting solely of clinic-based supervised high-dose strengthening exercises (Glossary—Appendix VI). [15] The body of evidence suggests that supervised high-dose strengthening exercises do not offer benefit compared to unsupervised strengthening exercises or advice. [15, 83, 84]
Multimodal care Clinicians may consider a maximum of six sessions over 8 weeks of multimodal care that includes range of motion exercises and manual therapy (manipulation or mobilization to the cervical and/or thoracic spine as clinically indicated). [16] Multimodal care may only be considered if not previously provided in the first 3 months of care. However, a second course may be indicated if the patient has demonstrated ongoing and significant improvement. As described above, this recommendation is informed by two systematic reviews. [16, 22]
Soft tissue therapy Clinicians may consider up to ten sessions over 10 weeks of clinical massage (Glossary— Appendix VI). [21] Clinical massage is expected to provide short-term benefits only. The body of evidence suggests that clinical massage with self-care offers benefit compared to self-care advice alone. [21, 68, 85]
However, clinicians should not offer relaxation massage (Glossary—Appendix VI). [21]
This recommendation is based on one low risk of bias RCT suggesting that relaxation massage (e.g., Swedish massage) was less effective than sham laser acupuncture or acupuncture for NAD of variable duration. [21, 68]
Clinicians should not offer strain-counterstrain therapy (Glossary—Appendix VI). [21]
This recommendation is based on two low risk of bias RCTs suggesting that:(1) ischemic compression and strain-counterstrain therapy provided no added benefit
to muscle energy technique for improving neck pain intensity, disability and motion
in the short-term for recent NAD [21, 66]
(2) strain-counterstrain therapy is not more effective than sham strain-counterstrain
therapy in the short-term. [21, 67]Passive physical modalities Clinicians may consider up to 12 sessions over 4 weeks of clinic-based low level laser therapy (LLLT). [21] LLLT may be offered in a continuous or pulsed application (wavelength = 830 or 904 nm). This recommendation is based on six RCTs in which the preponderance of evidence suggests that clinic-based LLLT offers greater benefit than placebo. [21, 86–91]
Clinicians should not offer transcutaneous electrical nerve stimulation (TENS). [21] This recommendation is based on two low risk of bias RCTs suggesting that:(1) TENS is no more effective than placebo [21, 92]
(2) TENS provides similar outcomes to multimodal programs of care
that include ineffective interventions (i.e., Jones technique). [21, 51]Clinicians should not offer pulsed short-wave diathermy. [21] This recommendation is based on one RCT suggesting that adding short-wave diathermy to advice and exercise provides no benefit. [21, 93] Cost-effectiveness data suggest that short-wave diathermy appears less cost-effective than advice and exercise. [94]
Clinicians should not offer electrical muscle stimulation or moist heat as an intervention in the clinic. [21] This recommendation is based on one low risk of bias RCT suggesting that electrical muscle stimulation or moist heat provided no additional benefit to a course of spinal manipulation or mobilization. [21, 73]
Psychological intervention Clinicians should not offer a stand-alone course of relaxation training for pain intensity or disability outcomes. [19] This recommendation is based on two low risk of bias RCTs. [52, 53, 95] The first RCT found that group-based pain and stress self-management (focused on relaxation training) by physiotherapists leads to similar pain and disability outcomes to multimodal physiotherapy. [52, 53] However, the second RCT found that relaxation training is no more effective than the advice to act as usual for pain and disability. [95] Therefore, evidence suggests that muscle relaxation training is not effective for improving pain or disability outcomes in patients with persistent NAD grades I–II. This should not, however, be taken as ruling out the use of psychological interventions where these are indicated for treatment of psychological distress, as opposed to pain or disability management alone.
Acupuncture Clinicians should not offer electroacupuncture. [21] This recommendation is based on one low risk of bias RCT that found similar outcomes between electroacupuncture and simulated acupuncture for WAD of variable duration. [21, 74]
Medication The non-opioid first ‘step’ in the World Health Organization analgesic ladder includes NSAIDs, muscle relaxants and acetaminophen. [75] However, the best available evidence does not indicate that acetaminophen is an effective analgesic for persistent NAD and spinal pain [20, 76]; therefore, acetaminophen should not be recommended or prescribed as a routine intervention.
Moreover, there was insufficient evidence to support prescriptions of muscle relaxants for persistent NAD and spinal pain. [20]
However, the evidence suggests that clinicians may consider NSAIDs for this population. [18] This recommendation is based on two low risk of bias RCTs from one low risk of bias systematic review suggesting that NSAIDs may be more effective than placebo. [14] Prolonged use is not warranted and the potential adverse effects associated with NSAIDs should be discussed with the patient. [18] Finally, there is no evidence of differential effectiveness across various drugs within the NSAID class [18] and there is also no evidence that combining NSAIDs with other medications provides added benefit. [18]
With respect to off-label usage of botulinum toxin injections for NAD and spinal pain, on the basis of a purported analgesic or muscle relaxant effect, clinicians should not offer botulinum toxin injections. [20] This recommendation is based on six low risk of bias RCTs in two low risk of bias systematic reviews [96] suggesting that there were no differences between botulinum toxin injections and placebo. [96, 97]
Recommendation 6: Management of recent NAD
For patients with NAD grade III B3 months duration, clinicians may consider supervised strengthening exercise in addition to structured patient education. In view of evidence of no effectiveness, clinicians should not offer structured patient education alone, cervical collar, lowlevel laser therapy, or traction.
Structured patient education As described above, clinicians should provide information about the nature, management, and course of NAD III as a framework for initiating the program of care. The structured education program should focus on providing advice to stay active and reassuring the patient by addressing expectations of recovery. [17, 46]
Clinicians should not offer structured patient education alone. [17]
This recommendation is based on six low risk of bias RCTs suggesting that:(1) structured patient education alone provides no benefits compared to
other conservative treatments (i.e., physiotherapy, supervised exercises,
massage) or unstructured advice in improving the recovery of patients
with NAD [17, 46, 56, 79, 85, 98];
(2) one method of delivering an education intervention is not superior to another. [17, 99]Exercise Clinicians may consider two sessions per week for 6 weeks of supervised graduated neck strengthening exercises [15] (Appendix VII). This can be supplemented with a home exercise program that includes daily stretching, strengthening, and relaxation exercises and may be supplemented by acetaminophen or NSAIDs. This recommendation is based on one low risk of bias RCT suggesting that strengthening exercises are more beneficial than advice but provide similar benefits as a semi-hard cervical collar and rest for recent-onset cervical radiculopathy. [15, 100] However, a cervical collar is not recommended due to its potential risk of harm (e.g., iatrogenic disability, inactivity, deconditioning, lack of self-efficacy) that exceeds the potential for benefit. [101]
Traction Clinicians should not offer traction. [21] This recommendation is based on one low risk of bias RCT suggesting that traction provides no added benefit to multimodal care for cervical radiculopathy. [21, 102]
Passive physical modalities Clinicians should not offer a cervical collar. [21] Despite similar outcomes for the use of a semi-rigid cervical collar and graded neck strengthening exercises [21, 100], we do not recommend using cervical collars for NAD III based on:(1) the need to monitor the use and prescription of a cervical collar
as outlined in the trial protocol would be impractical;
(2) the widely recognized ethical concerns that the potential risk of harm
(e.g., iatrogenic disability, inactivity, deconditioning, lack of self-efficacy)
exceed the potential for benefit. [101]Clinicians should not offer LLLT. [21] This recommendation is based on one low risk of bias RCT suggesting that LLLT was equal to placebo LLLT for recent-onset cervical radiculopathy. [21, 103]
Recommendation 7: Management of persistent NAD
Grade III (Table 5, Table 6; Figures 3, 4) Clinicians should not offer a cervical collar. Patients who continue to experience neurological signs and disability more than 3 months after injury should be referred to a physician or for investigation and management. This recommendation is based on one low risk of bias RCT suggesting that use of a cervical collar provides outcome similar to an individualized multimodal program of care in the medium and long term. [21, 69] However, we do not recommend the use of cervical collars given the ethical concerns that the potential risk of harm exceeds the potential for benefit. [101]
Recommendation 8: Reevaluation and discharge
Clinicians should reassess the patient at every visit to determine if:(1) additional care is necessary;
(2) the condition is worsening; or
(3) the patient has recovered.
Patients should be discharged as soon as they report significant recovery.
Health care professionals should use the self-rated recovery question to measure recovery:
‘‘How well do you feel you are recovering from your injuries?’’. [104–108]
The response options include:(1) completely better
(2) much improved
(3) slightly improved
(4) no change
(5) slightly worse
(6) much worse
(7) worse than ever.Patients reporting to be ‘completely better’ or ‘much improved’ should be considered recovered.
The self-rated recovery question is a valid and reliable global measure of recovery in patients with neck pain. [104–108]
Patients who have not recovered should follow the care pathway outlined in the guideline (Figures 1, 2, 3, 4).
Discussion
We developed an evidence-based clinical practice guideline to help clinicians deliver effective interventions for the management of NAD (which includes WAD) and promote uniform high quality care for patients with neck pain. The recommendations are based on recent systematic reviews of the literature and synthesis of best available evidence. Implementing evidence-based recommendations for a common condition, such as neck pain, will likely improve patient outcomes, reduce regional variations, and improve the efficiency of the healthcare system. [109, 110]
The guideline identifies clinical interventions that should not be prescribed because they are ineffective or because their effectiveness is not clearly established. For example, we found inconclusive evidence for the effectiveness of needle acupuncture, cognitive behavioral therapy, and biofeedback for the management of persistent NAD grades I–II. [19, 21] The evidence on the effectiveness of these interventions is inconclusive because the results of multiple high-quality RCTs conflicted with each other. Finally, the guideline does not recommend interventions that have not been evaluated in high-quality studies.
Summary of recommendations
Clinicians should rule out major structural or other pathologies as the cause of NAD. In the absence of major structural or other pathologies, clinicians should classify NAD as grades I, II, or III and determine the presence of prognostic factors for delayed recovery. The management of all patients should include education, advice, encouragement to stay active (including return to work where appropriate), and reassurance that NAD is typically of a time-limited nature. In the context of shared decision-making, clinicians should discuss with the patient the range of effective interventions available for the management of NAD. Supplementing self-management strategies with clinical care may be indicated provided the intervention is likely to enable recovery through symptom relief and improvement in function. For such interventions, there is no evidence that effectiveness can be increased through more frequent attendance or prolonged course of treatment. [43, 44]
The following clinical interventions can be considered for recent onset NAD grades I and II (B3 months): range of motion exercises with or without manipulation or mobilization, or muscle relaxants. For persistent NAD grades I– II ([3 months), clinicians can consider supervised range of motion and strengthening exercises, qigong, yoga, multimodal care (exercise with manipulation or mobilization), clinical massage, LLLT, or NSAIDs. It is important to note that all recommended interventions provide small benefits at best.
Patients with recent NAD grade III (B3 months) should be treated with supervised strengthening exercise. Patients with NAD grade III who still experience neurological signs and disability 3 months after injury should be referred to a physician for further investigation of neurological deficits.
Comparison to previous guidelines
Overall, our recommendations agree with those of previous clinical practice guidelines. [9, 13, 111–116]Our recent systematic review of guidelines for the management of WAD suggests that treatment options include: advice, education, reassurance, exercise, return-to-activity, mobilization/manipulation, and analgesics. [13] All guidelines agree that collars are contraindicated for WAD. [13] Moreover, the 2008 clinical practice guideline from the American Physical Therapy Association recommends that the management of neck pain include: education, cervical and thoracic mobilization/manipulation, exercises, and traction; and that neck-related arm pain should be managed with thoracic mobilization/manipulation and exercises. [115]
There are a few important differences between previous guidelines and ours. Specifically, we do not recommend analgesics or traction for the management of neck pain. This difference is likely because most of the previous guidelines are dated. [34] The Neck Pain Task Force identified one study that found no differences between an analgesic (benorylate) and placebo for reducing pain. [14, 117] Our recent systematic review did not find any eligible studies that evaluated the effectiveness of analgesics for neck pain. For traction, the Neck Pain Task Force did not find enough evidence to determine the effectiveness of traction. [14, 118] Our recent systematic review identified one study that found traction does not provide added benefit to a multimodal program for NAD grade III [21, 102]. Moreover, our guideline specifies the interventions that should not be used because the evidence suggests that they are ineffective. [14, 102, 117, 118]
The evidence published since the release of previous clinical practice guidelines has improved our ability to effectively manage patients with neck pain. Prior to the OPTIMa guideline, the most recent guidelines were published in 2008. [111, 115] Since then, high quality RCTs suggest that multimodal care (i.e., exercises and manipulation/mobilization) is effective for the management of recent-onset neck pain and that Iyengar yoga, qigong, and clinical massage may benefit patients with persistent neck pain. [16, 80–82, 85] Moreover, the evidence indicates that strain-counterstrain, relaxation massage, and electroacupuncture should not be used to manage patients with recent-onset and persistent neck pain. [67, 68, 74, 85] For recent NAD grade III, recent evidence suggests that graded neck strengthening exercises should be used, while LLLT and traction should not be used. [100, 102, 103] Finally, the OPTIMa guideline provides parameters on the dosage of interventions that are informed by high quality RCTs. Therefore, recent literature provides clinicians with current best evidence that informs the management of their patients.
We conducted eight systematic reviews to update the work of the Bone and Joint Decade Task Force on Neck Pain and Its Associated Disorders and inform these recommendations. [15–22] Despite recent improvement in the quality of the literature on the management of neck pain, there are still important gaps. Specifically, the evidence is still inconclusive on the effectiveness of acupuncture, cognitive behavioral therapy and biofeedback. [19, 21] Therefore, efforts should be dedicated to determine the effectiveness of these interventions. In addition, research should also consider identifying the most effective dosage to optimize treatment response for all interventions.
Dissemination and implementation of this guideline
It is important to consider factors related to dissemination and implementation of this guideline. Few of the previous high quality guidelines in this area assessed the resource implications and implementation issues related to their adoption by clinicians and policy makers. [13] In Canada, the Government of Ontario is considering the applicability of this guideline to the Ontario health care system and automobile insurance system.
The guideline could be adapted for local use in other jurisdictions. We recommend that clinicians, insurers and policy-makers use the ADAPTE framework to adapt this guideline to their needs and environment. [119]
Strengths and limitations
This clinical practice guideline was informed by comprehensive literature searches and its recommendations were based on high-quality evidence. When developing clinical recommendations, the Guideline Expert Panel considered effectiveness, safety, cost-effectiveness, consistency with societal and ethical values, and patient preferences and experiences. Moreover, the recommendations include consideration of effect sizes and minimal clinically important differences to assess the magnitude of benefit of an intervention on patient outcomes. Finally, the Guideline Expert Panel disclosed any conflicts of interest and maintained editorial independence. [120]
We conducted a supplementary search of MEDLINE extending to May 2015 to identify any recently published RCTs and systematic reviews relevant to the guideline. This search (extending from January 1, 2013 and May 29, 2015) yielded 592 articles, of which 20 were relevant and 15 RCTs were of high quality [121–135] (five studies were low quality [134, 136–139]).
The low risk of bias studies from the updated search investigated the following interventions:(1) acupuncture [121, 122, 133]
(2) exercise [123–126, 134]
(3) manual therapy [127, 128]
(4) passive physical modalities [129]
(5) soft tissue therapy [122, 130]
(6) multimodal care [125, 126, 131, 132, 135] and
(7) psychological interventions [123].None of these trials presented information that conflicted with the recommendations of this guideline.
Our recommendations were limited by the amount, nature, and quality of evidence published in the literature. [15–22] For example, very few studies have investigated the effectiveness of medication for the management of patients with NAD. [18, 20] Moreover, most RCTs studied the relative effectiveness of commonly-used interventions, but little evidence is available to determine whether popular interventions are more effective than placebo/sham treatments. Inconclusive evidence on the effectiveness of commonly-used interventions (e.g., needle acupuncture) prevents the development of clinical recommendations. There is a need for research to address these limitations in the literature. Finally, our supplemental search extending to May 2015 was conducted in MEDLINE only; however, MEDLINE is one of the main biomedical databases to search healthcare literature. [140]
Acknowledgments
The authors would like to acknowledge the invaluable contributions to this guideline from: Lynn Anderson, Poonam Cardoso, Brenda Gamble, Willie Handler, Vivii Riis, Paula Stern, Thepikaa Varatharajan, Angela Verven, and Leslie Verville.
Compliance with ethical standards
Funding The development of this clinical practice guideline was funded by the Ministry of Finance and the Financial Services Commission of Ontario (OSS_00267175). The Ministry of Finance and Financial Services Commission of Ontario were not involved in the design, conduct, or interpretation of the research that informed the development of the care pathways included in this report. The development of the guideline by the Guideline Expert Panel was not influenced by the Ministry of Finance or Financial Services Commission of Ontario; the views and interests of the funding body did not influence the final recommendations. All individuals involved in the project declared any competing interests. This research was undertaken, in part, thanks to funding from the Canada Research Chairs program to Dr. Pierre Coˆte´, Canada Research Chair in Disability Prevention and Rehabilitation at the University of Ontario Institute of Technology, and funding from Alberta Innovates—Health Solutions to Dr. Linda Carroll, Health Senior Scholar.
Conflict of interest Dr. Brison reports no commercial interest; a university role that incorporates research activities related to guideline development.
Dr. Lacerte reports an active clinical practice and conducting medicolegal assessments or reports for plaintiff lawyers and occasionally independent medical examinations for lawyers and insurers;
Consultancies: Drs. Ameis and Lacerte reports non-paid consultancy for the Catastrophic Impairment Expert Panel;
Honoraria: Drs. Gross and Bohay report honoraria during the conduct of this study;
Grants: Dr. Coˆte´ reports grants from Ontario Ministry of Finance and Financial Services Commission of Ontario during the conduct of this study; grants from Aviva Canada outside the submitted work.
Dr. Gross reports grants from Workers’ Compensation Board of Alberta, grants from Workers’ Compensation Board of Manitoba, outside the submitted work;
Other: Drs. Brison and Marshall report participation in guideline development.
Dr. Coˆte´ reports funding from Canada Research Chair Program – Canadian Institutes of Health Research during the conduct of this study; personal fees from National Judicial Institute, Socie´te´ des experts en e´valuation me´dico-le´gale du Que´bec, and European Spine Society, outside the submitted work.
Dr. Ameis reports his past role as medical director and current consultant to Granite Health Service. For the remaining authors, no conflicts were declared.
Appendix 1–7:
Appendix 1–7.
References and Figures:
Please refer to the Full Text article.

Return to CHRONIC NECK PAIN
Return to GUIDELINES Articles
Return to NECK DISORDER GUIDELINES
Since 3-18-2016


| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |