

Best Practices Recommendations for Chiropractic Care
for Older Adults: Results of a Consensus ProcessThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Manipulative Physiol Ther 2010 (Jul); 33 (6): 464–473 ~ FULL TEXT
Cheryl Hawk, DC, PhD, Michael Schneider, DC, PhD, Paul Dougherty, DC,
Brian J. Gleberzon, DC, Lisa Z. Killinger, DC
Cleveland Chiropractic College,
Overland Park, KS 66210, USA.
cheryl.hawk@cleveland.edu
These recommendations have been updated by the 2017 article:
Best Practices for Chiropractic Care for Older Adults: A Systematic Review
and Consensus UpdateOBJECTIVE: At this time, the scientific evidence base supporting the effectiveness of chiropractic care for musculoskeletal conditions has not yet definitively addressed its appropriateness for older adults. Expert consensus, as a form of evidence, must be considered when higher levels of evidence are lacking. The purpose of this project was to develop a document with evidence-based recommendations on the best practices for chiropractic care of older adults.
METHODS: A set of 50 seed statements was developed, based on the clinical experience of the multidisciplinary steering committee and the results of an extensive literature review. A formal Delphi process was conducted, following the rigorous RAND-UCLA (University of California, Los Angeles) methodology. The statements were circulated electronically to the Delphi panel until consensus was reached. Consensus was defined as agreement by at least 80% of the panelists. There were 28 panelists from 17 US states and Canada, including 24 doctors of chiropractic, 1 physical therapist, 1 nurse, 1 psychologist, and 1 acupuncturist.
RESULTS: The Delphi process was conducted in January-February 2010; all 28 panelists completed the process. Consensus was reached on all statements in 2 rounds. The resulting best practice document defined the parameters of an appropriate approach to chiropractic care for older adults, and is presented in this article.
CONCLUSION: A multidisciplinary panel of experienced chiropractors was able to reach a high level (80%) of consensus on evidence-informed best practices for the chiropractic approach to evaluation, management, and manual treatment for older adult patients.
From the Full-Text Article:
Introduction
By 2030, nearly 1 in 5 US residents is expected to be 65 years or older. [1] Chiropractors commonly provide care to older adults in the United States, with approximately 14% of chiropractic patients being 65 years or older. [2] With musculoskeletal conditions cited as a leading cause of disability in this population, [3] it is important that the large body of evidence for the effectiveness of chiropractic care be examined for relevance to the geriatric population. This is particularly important given the statements made by the American Geriatric Society (AGS) in their clinical practice guidelines for the management of chronic pain in older adults. The 1998 AGS report made the following recommendation on chiropractic (based on the single study available at that time): [4]“Chiropractic, acupuncture or transcutaneous nerve stimulation may be helpful for some patients, but they are expensive and have not been shown to have greater benefit than placebo controls in the management of chronic pain.”
The most recent AGS clinical practice guideline on the management of persistent pain in older adults, published in 2002, stated: “Unrelieved persistent pain commonly causes patients to seek relief with alternative medicine, including homeopathy, naturopathy, chiropractic, and spiritual healing.” [5] Although a substantial body of research related to chiropractic has accumulated since 2002, most of it addresses conditions of the general adult population, not those of older adults specifically. A 2010 report by Bronfort et al on the effectiveness of spinal manipulation or mobilization therapy (SMT) summarized current evidence from systematic reviews and randomized controlled trials. [6] It found that SMT is effective in adults for low back pain (acute and chronic). Furthermore, the report found that SMT was effective in the treatment of migraines, cervicogenic headaches, cervicogenic dizziness, and painful conditions in some extremity joints. It reported that SMT of the thoracic spine is effective for both acute and subacute neck pain but that the evidence was inconclusive for cervical SMT alone for neck pain or SMT for older adults with pneumonia. The evidence was also found to be inconclusive for thoracic pain, sciatic pain, tension headaches, fibromyalgia, knee osteoarthritis, myofascial pain, and migraines. Spinal manipulation was considered not effective for adults with hypertension.
Concerning the safety of manipulation, in the general population of chiropractic patients, serious adverse events are rare. [6] A 2008 case-control study found that there was no increased risk of vertebrobasilar stroke associated with neck manipulation by chiropractors, in the study population (mean age 63 years) of 3982 (818 cases). [7] In a study of 280 chiropractic patients (13% were over age 60), minor and transient adverse effects such as muscle soreness were common after manipulation, but most resolved within 24 hours and did not affect daily activities. [8] A 2009 systematic review evaluated 46 articles that included data concerning adverse events associated with spinal manipulation. The authors reported that most events are benign and transitory, and the incidence of serious adverse events is rare. [9] It is important to note that these studies investigated the safety of manipulation for adult patients in general, not specifically older adults. At this time, evidence on the effectiveness and safety of chiropractic care specifically for the treatment of older adults is limited, with only 2 randomized controlled trials investigating chiropractic management for back pain in this population. [10, 11] The Bronfort et al report stated that evidence of moderate quality supported the effectiveness of spinal manipulation/mobilization for subacute and chronic low back pain in older adults. [6] The body of evidence investigating various techniques of spinal manipulation is emergent, but suggests that it is important to tailor the manipulative technique to the clinical presentation and preferences of patients. [10–13]
Many chiropractors use technique systems that do not involve high velocity, low amplitude manipulative procedures. Specifically, chiropractors often substitute or preferentially use any of the following technique approaches or systems: instrument-assisted procedures, pelvic blocking, mechanized or non-mechanized table-assisted procedures, and other low-force techniques. [14, 15]
Chiropractic care is not limited to joint manipulation and mobilization techniques. Chiropractors also provide manual soft tissue treatments such as massage, acupressure, manual trigger point therapy, myofascial release and transverse friction massage. They use a wide range of nonmanipulative procedures. The most commonly used nonmanipulative procedure is patient education, used by 95% of chiropractors. Other treatments include exercise (92%), massage (77%), electrical therapy (71%), ultrasound (67%), heat therapy (66%), and acupressure (61%). [2] Concerning massage, the 2010 Bronfort et al report found massage to be effective for chronic low back pain and chronic neck pain in adults. [6]
It is well established that strength training and balance exercises are beneficial for improving physical function and reducing impairment in older adults in both the home and clinic settings. [16–20] Chiropractors often use these and other types of therapeutic exercise as an integral component of their treatment of older adults.
Like other health care providers, chiropractors provide health promotion counseling. There is strong evidence supporting counseling by providers for physical activity and exercise for older adults, for general health, and also for fall prevention. [5, 20–23 ] There is also strong evidence that older adults should be screened for fall risk factors (such as medication use—particularly polypharmacy—blood pressure, balance and gait, heart health, and home safety). [20, 23, 24 ]
Chiropractic training includes required coursework in geriatrics. [2, 25] Standard texts used in chiropractic colleges include chapters on care of the older adult, written by experienced chiropractic clinicians. [12, 26–28] These chapters provide comprehensive information on the physiology and epidemiology of aging, risk factors for poor health outcomes, prevention and health promotion, detailed information on appropriate use of manual procedures including spinal manipulation for frail elderly, and on exercise and adjunctive therapies. [29] Assessments of chiropractic coursework in geriatrics have noted that 15 to 30 course hours are required of chiropractic students, with no required clinical or interdisciplinary experience with older adult patients. [26, 30, 31] One approach proposed in the literature for increasing clinical experience in geriatrics is to develop opportunities for participating with interdisciplinary teams to address the various aspects of patient care. [26] Incorporation of interdisciplinary principles and practice has been found to be well-received by chiropractic students. [31] Currently, there are few geriatric residency programs offered at chiropractic colleges, and no specialty board such as is represented for chiropractic pediatrics or orthopedics. There are also no established postgraduate certification programs in geriatrics for chiropractors.
Clearly, the scientific evidence base has not yet definitively addressed the appropriateness of chiropractic care for older adults, particularly with respect to the safety of spinal manipulation for older adults.
Expert consensus, as a form of evidence, must be considered when higher levels of evidence are lacking. [32] The purpose of this project was to develop evidence-based recommendations on the best practices for chiropractic care of older adults, through a formal consensus process among a multidisciplinary group of experts on geriatrics and chiropractic.
Methods
Overview of Project
The purpose of this project was to develop a consensus document on chiropractic care for adults aged 65 and older, using a best practice rather than guideline approach. Best practice has been described as follows:“Best practice is not a specific practice per se but rather a level of agreement about research-based knowledge and an integrative process of embedding this knowledge into the organization and delivery of health care. Best practice requires a level of agreement about evidence to be integrated into practice. Best practice . . . can bridge the practice-research gap and provide a basis for researchers and clinicians to work together to translate research into meaningful practice.” [33]
The document was not intended to be prescriptive, but to outline the features of chiropractic care which, based on the experts' clinical experience and available evidence, represent the most beneficial approach to chiropractic care for the geriatric population. It is important to recognize that the term “chiropractic care” is not limited to the use of various manual therapies and therapeutic exercise. Many chiropractors utilize adjunctive modalities and physical agents such as ultrasound, diathermy, electrical stimulation, and lasers in their management of older adults. [2] Many chiropractors incorporate diet modification, often including nutritional supplements, as well as counseling on health behavior change into their treatment plan for older adults. This consensus process did not address these components of chiropractic care in depth; it limited its scope to the appropriate application of manual therapies. For the purpose of this project, manual treatment was considered to include spinal and extremity joint manipulation or mobilization, massage and other soft tissue techniques.
Human Subjects Considerations
Before the start of the project, it was approved by the lead institution's institutional review board. Written permission to use their names was obtained from all participants.
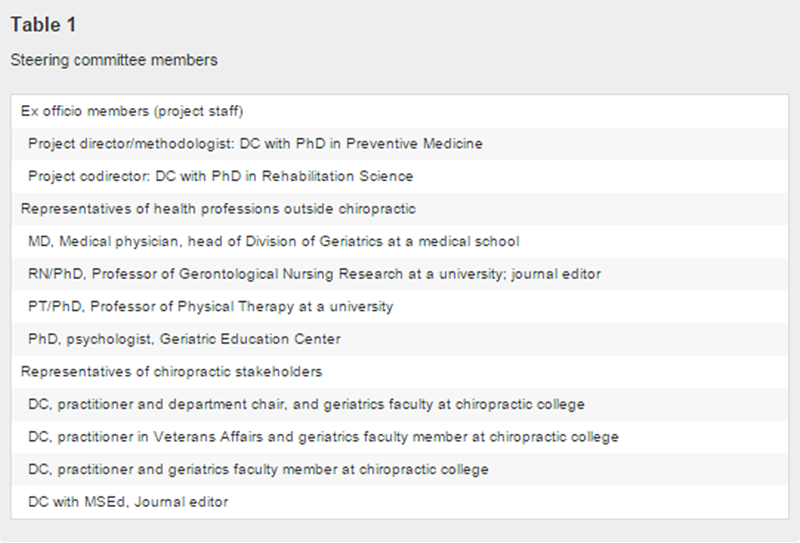
Steering Committee

Table 1 The steering committee (SC) was composed of nationally recognized experts in geriatrics, representing 5 different health professions — chiropractic, medicine, nursing, physical therapy, and psychology. Members were selected to provide project oversight and ensure that all stakeholders' issues and concerns were addressed. Table 1 summarizes the professions and experience represented in this multidisciplinary group.
Literature Review and Seed Documents
A literature review completed by members of the project team in 2005 was updated by an experienced research associate and the results were summarized to provide background information to all participants. The project director and codirector formed a subcommittee composed of 3 members of the SC to assemble the background literature and seed documents, which were then reviewed by the SC for completeness and relevance. The documents provided background on effectiveness and safety, as well as training of chiropractors in caring for older adults. In addition, all participants were provided with a complete list of all citations from the literature review and full text of any article on the list was made available to them.
Development of Seed Statements
The seed statement subcommittee, all chiropractors in academic settings with many years of clinical and research experience, much of it with older adults, developed a set of seed statements, based on the literature and on their experience. The first draft of the document was sent to the SC for review and revision. The final seed statement document consisted of 50 statements addressing all aspects of the clinical encounter. These statements were circulated to the Delphi panel. After they reached consensus, the resulting document was sent to the SC for approval and then returned to the Delphi panel for final approval.
Delphi Consensus Process
The Delphi consensus process was conducted electronically, via e-mail. This method not only reduces costs and time to completion, but also minimizes the possibility of group members influencing one another's opinions, or having one member dominate the group. Panelists were blinded to the identity of other panelists throughout the Delphi process. We followed the rigorous and widely-accepted RAND-UCLA (University of California, Los Angeles) methodology for conducting the Delphi process. [34] We asked panelists to rate the appropriateness of the procedure or practice described in each seed statement. As per the RAND-UCLA methodology, “appropriateness” was used to indicate that the expected health benefit to the patient exceeds the expected negative consequences by a sufficiently wide margin that it is worth doing, exclusive of cost. [34] The rating document provided a scale of 1 to 9 (highly inappropriate to highly appropriate). We instructed the panelists to provide specific reasons for “inappropriate” ratings, providing a citation from the peer-reviewed literature to support it, if such exists.
In analyzing the responses, we scored ratings of 1 to 3 as “inappropriate;” 4 to 6 as “undecided;” and 7 to 9 as “appropriate.” We considered consensus on appropriateness to be present if at least 80% of panelists rated a given statement as 7, 8, or 9 and the median response score to that statement was also between 7 and 9. The Delphi round was to be repeated, including only the statements on which consensus was not reached, after revising those seed statements as per the panelists' comments each time, until consensus was reached or no further change was possible, in which case a minority opinion would be included in the final report. All panelists' comments were provided (with only code numbers identifying them) to all panelists after each round, to assist them in making their rating decisions.
Composition of the Delphi Panel
The SC was asked for nominations for the Delphi panel, and the project team circulated a notice to geriatrics instructors at all US chiropractic colleges, as well as leaders in chiropractic professional organizations and practitioners and faculty involved in geriatrics research and/or practice. Nominees and volunteers completed a form describing their background characteristics and provided their CVs. The SC and project team reviewed these and selected panelists based on their experience and diversity of characteristics, in terms of geography, demographics, and profession. An emphasis was placed on identifying geriatrics experts from outside the chiropractic profession, as well as DCs with dual degrees.
Results
Delphi Panel
Twenty-eight panelists (19 men and 9 women) made up the Delphi panel. Twenty-four were DCs, 1 was a physical therapist (PT); 1, a registered nurse (RN) who specializes in geriatrics; 1, a psychologist (PhD); and 1, a licensed acupuncturist (LAc). Seventeen of the 28 panelists are faculty members at chiropractic colleges, and 3 are faculty members at non-chiropractic institutions. Among the DCs, there were several with dual degrees: one, a DC/MD (medical doctor); 2, DC/MT (massage therapist); and one, a DC/RN. Two panelists had PhDs in addition to their professional degree, one in epidemiology and the other in gerontology. Two had MPH degrees and 2 had MS degrees, one in clinical research and one in biomechanics and exercise physiology. The panelists represented 17 US states and one panelist was from Ontario, Canada. The states were CA, CT, GA, IA, IL, KS, MN, MO,MS, NC, NY, OH, OR, PA, TX, VA, and WA. In terms of advanced training in geriatrics, one panelist had a PhD in gerontology and a postdoctoral fellowship in preventing and managing chronic illness; another had certification as a Geriatric Clinical Specialist. Seventeen of the 24 DC panelists were members of the American Chiropractic Association, and one a member of the International Chiropractors Association. The panelists in active practice had been in practice a median of 20 years (range, 8–40 years); the median estimate for proportion of their patients who are age 65 or older was 25% (range, 12%–90%).
Results of Delphi Rounds: Best Practice Consensus Statements: Chiropractic Care for Older Adults
The Delphi process was conducted in January to February 2010. All 28 panelists participated in the process. Consensus, which we had defined at the start of the project as requiring at least 80% agreement on appropriateness, with a median rating of 7 or higher, was reached on all statements in 2 rounds. The final percentages of agreement on the 50 statements were very high, with 6 statements having 100% agreement; 26 with 90% to 99%, and the rest with 85% to 89%. The following statements are the result of this process.Purpose and Introduction The purpose of this best practice document is to define the parameters of an appropriate approach to chiropractic care for older adults, which is in both the patient's and the public's interest.
The potential benefits of any health care intervention must consider patient preference and should be weighed against the associated risks and the costs in terms of time and money.
In a biopsychosocial approach to health care, it is recognized that there are significant age-related anatomical, physiological, psychological and psychosocial changes which may affect the appropriateness of any given health care intervention.
General Clinical Principles in the Care of Older Adults
The normal age related changes in the neurologic and musculoskeletal systems of older adults create unique findings which may require specific consideration during the physical examination (such as peripheral neuropathy, age-related muscle loss and loss of flexibility).
Physical, psychosocial, and emotional responses to intervention may vary in the older adult.
The Chiropractic Clinical Encounter
Informed consent by the patient or legal representative is required before performing an examination, diagnostic tests, or initiating a management program.
Consent must be fully informed, voluntary, related to the patient's condition, and not be obtained by misrepresentation. The patient must have the capacity to understand the information in order to provide informed consent. If they do not, then a substitute decision maker must be consulted.
Consent is a process and not a one-time, specific event and should be modified as warranted.
Chiropractic Management
Chiropractic management of the older patient should follow the 3 basic principles of evidence based practice, which are to
(1) make clinical judgments based on use of the best available evidence combined with
(2) the clinician's experience, and expertise and
(3) the patient's preferences.The effectiveness of chiropractic care for many geriatric conditions has not yet been definitively established; however, lack of conclusive evidence does not necessarily imply that chiropractic care is not effective.
In the absence of conclusive evidence, a combination of clinician experience and patient preference is considered a reasonable approach for a time-limited, outcome-based therapeutic trial of chiropractic care.
There are 3 basic chiropractic management approaches to the care of the geriatric patient:
(1) sole management by a chiropractic physician,
(2) comanagement with other appropriate health care providers, and
(3) referral to a recognized licensed or certified health care provider/specialist.Comanagement with other appropriate health care providers is common in older adults and may be appropriate under any number of conditions. These include but are not limited to the following:
The patient is not showing clinically significant improvement, or is showing a worsening of symptoms, after a time-limited initial trial of chiropractic care.
The patient requests such a comanagement approach.
There are significant comorbidities that could be outside the scope of chiropractic practice.
If a patient is not responding to the therapeutic intervention it is appropriate to order a consultation with another health care provider, or order additional diagnostic testing.
Older adult patients often have multiple health care conditions being managed by multiple health care providers. The chiropractor, as part of this team, should make every reasonable attempt to obtain copies of all relevant clinical records and files, and to communicate his/her findings to other health care providers.
The chiropractor should, if at all possible, communicate directly with that health care provider, within Health Insurance Portability and Accountability Act (HIPAA) guidelines, in order to provide important clinical information.
Clinical History
Extracting relevant clinical information during the case history of some older adults may require special communication skills and experience, due to changes in their hearing, sight, coordination and cognition. If these impairments are noted, the chiropractor should obtain permission to have the patient's family member or caregiver accompany him or her.
The comprehensive case history at the initial visit should include a review of systems, family history, health care history, concurrent health care and both prescription and nonprescription medication use, including supplements, herbs, and nutriceuticals. Information on health habits, including tobacco use, alcohol use, diet, sleep, physical activity, falls, and other injuries should be included. Activities of daily living (ADLs), which are basic tasks involving bodily issues such as bathing, toileting, eating and walking, and instrumental ADLs, which are a higher level of function than ADLs, such as cooking, writing, and driving, should be reviewed. Prior occurrence of the chief complaint should be recorded, including length of time to recovery, type of treatment, and previous diagnosis.
Additional factors which must be considered during the case history for this age group include atypical presentation of many clinical conditions; underreporting of disease; overestimation of cognitive function; polypharmacy; and ageist attitudes held by patients, caregivers, family, and health care providers.
In many jurisdictions, chiropractors are required to inform appropriate social services if they reasonably suspect an older person is the victim of physical or sexual abuse. Key features on history or physical examination are unexplained injuries in different stages of healing, and a history of abuse. In most cases of senior abuse, the abuser is the person's spouse or child, resulting from a cycle of abuse.
Many states' mandatory reporting laws include issues in addition to sexual or physical abuse, including financial, emotional/psychological abuse, and self- or caregiver neglect. Doctors of chiropractic should be conversant with the particulars of their state laws.
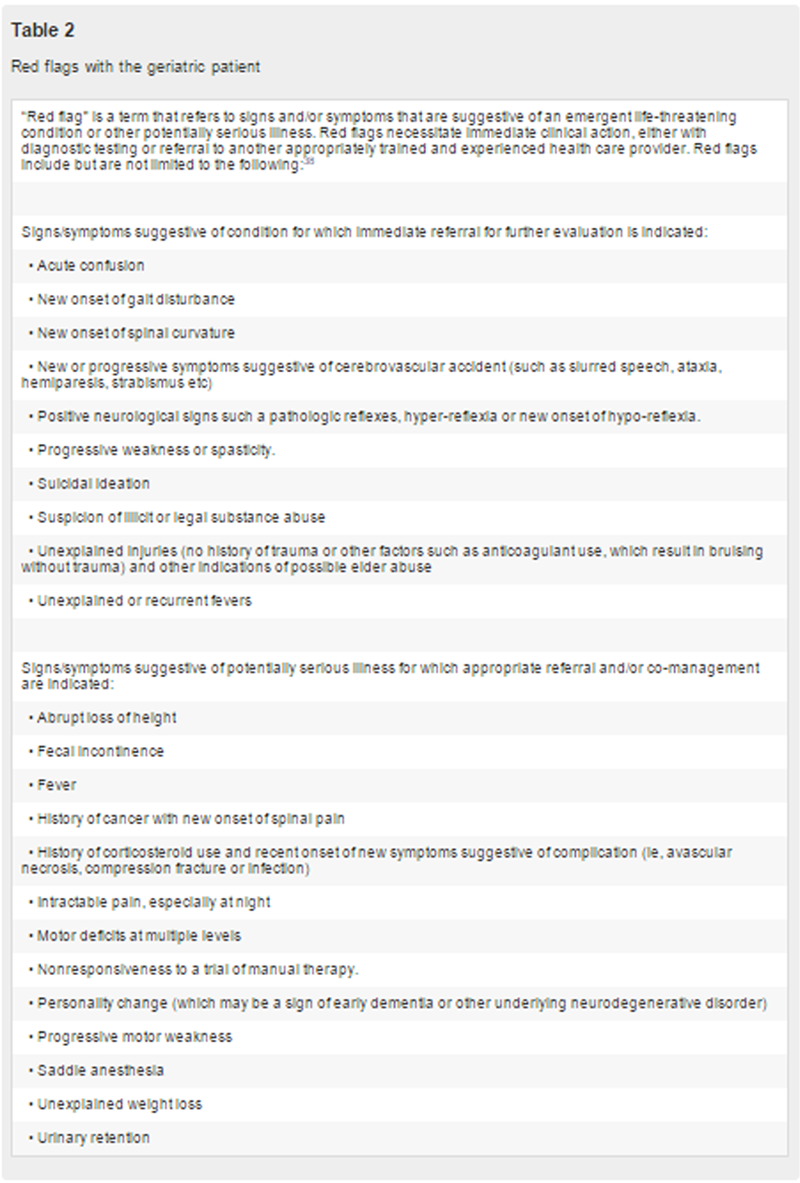
Chiropractors should be alert to signs and symptoms of emotional and mental health issues. Depression with suicidal ideation mandates referral to a mental health provider. Acute confusion (delirium) often requires hospitalization and cognitive impairments resulting from dementia necessitate involvement of a substitute decision maker.
Table 2 Red Flags If the history and/or examination reveal “red flags”—that is, absolute contraindications to care—or if these emerge during the course of care, the patient should be referred to an appropriate provider for further evaluation and/or care. See Table 2 for list of red flags.
Examination
Physical examination should be based on case presentation, to identify potentially serious pathology, and to support management decisions.
Necessary diagnostic or examination procedures outside the practitioner's scope of practice or range of experience should be referred to an appropriately qualified and experienced health professional.
Vital signs should be recorded, including temperature, heart rate, respiratory rate, weight, height, and blood pressure.
Pain is sometimes considered a vital sign, and should always be evaluated.
Comprehensive geriatric assessment, considered a best practice, should include assessment of physical health, functional health, cognitive health, oral/nutritional health, and home-environmental safety.
Diagnostic Imaging—Conventional Radiography
The use of radiography or repeated radiographs is not recommended without clear clinical justification.
The use of conventional radiography and other imaging procedures should be based on current evidence-informed clinical practice guidelines and the clinical judgment of the managing clinician.
Appropriate diagnostic imaging and/or referral for specialty consultation should be considered in patients who fail to respond to an initial brief trial of chiropractic care. In the patient who has failed to respond to this trial of care, the decision to pursue appropriate diagnostic imaging may be required to rule out serious conditions. The decision to pursue these tests should be derived from a thorough history, physical exam, and any previous diagnostic testing that has been performed.
Conventional radiographs may be indicated in cases of clinically suspected trauma-induced injury, such as fracture or dislocation, and also in cases of suspected compression fracture, even in absence of significant trauma, such as in patients with spinal pain that is not related to posture or position.
Conventional radiography is indicated in the presence of red flags for serious disease such as infection, neoplasm, recent fracture, or other bone diseases.
Advanced Diagnostic Imaging
Bone densitometry (not conventional radiography), is indicated for the quantitative measurement of bone mass in patient with suspected metabolic bone disease such as osteoporosis and osteomalacia.
Advanced diagnostic imaging may be required to rule out potentially serious conditions when an older adult patient has not responded adequately to a short trial of chiropractic care, or in the presence of red flags.
Manual Procedures The following considerations apply to treating older adults with manual procedures:
Patient size and frailty: biomechanical force should be modified in proportion to the size and frailty of the patient, as well as taking into consideration any anthropomorphic differences between the doctor and patient.
Contraindications to higher force manual techniques that may put strain on osseous structures may include severe osteoporosis or other bone weakening processes such as but not limited to infection or neoplasia.
Use of soft tissue techniques that may induce bruising should be used with caution or not used at all in patients who are currently on anticoagulation therapy or long-term corticosteroid medication.
Patient preferences: the clinician should adapt manipulation and soft tissue techniques and procedures that support the needs and comfort of the patient.
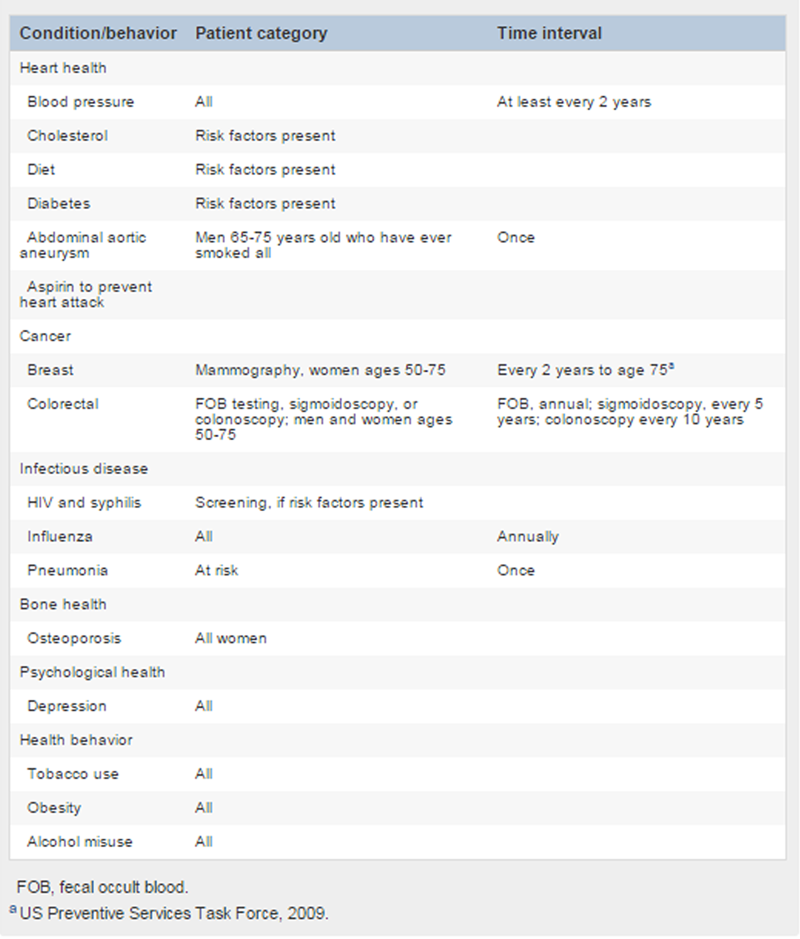
Table 3 Care Planning
Health promotion in older adults is an emerging concept in preventive medicine. This would include advice to stay physically active, maintain a healthy diet, and to engage in social activities. See Table 3 for a list of recommended screening and counseling chiropractors should include in care for the older adult.
Although immunization is a well-established medical approach to disease prevention, older adult patients may ask their chiropractor for information about immunizations. Chiropractors should provide balanced, evidence-based information from credible resources such as the Centers for Disease Control and/or refer the parents to such resources.
Routine manipulation of asymptomatic patients without clinical indicators is not recommended for therapeutic correction when Maximal Medical Improvement has been reached. However, older adults often have significant musculoskeletal degeneration that could benefit from periodic manipulation and therapeutic activities for the purposes of pain relief and/or improvement of function.
Some patients may self-select for manipulative care for the purpose of maintaining or optimizing function.
Care planning should also take into consideration factors such as whether the patient lives alone; his or her competence with activities of daily living, the availability of a competent caregiver, if needed, and the patient's access to transportation, and other necessary resources.
Discussion
Although chiropractic use among older adults is very common, the most appropriate role for chiropractic in the care of this population has yet to be definitively described. Currently, there are ongoing federally funded projects that are systematically evaluating the effectiveness and safety of chiropractic care specifically for the older adult population. [35] These projects, which focus on the integration of chiropractic into a variety of settings, such as nursing homes and Veterans Affairs facilities, will allow for evaluation of the practicality and sustainability of an integrated role for chiropractic in the care of older adults. [36, 37] However, until such projects have been completed, expert opinion is a useful tool to bridge the evidence gap.
The Delphi process conducted in this project serves as a mechanism to achieve consensus on best practices, until higher levels of evidence have been developed. An additional purpose for this document is to serve as a reference for those who are treating older adults to guide treatment principles. This is particularly important since, although there are currently some requirements for chiropractic students to complete coursework in geriatrics, clinical experience in that area is limited and there are few established residencies and/or post-graduate programs to provide the type of specialized training in geriatrics that is available in other professions.
The role of chiropractic in the treatment of older adult must acknowledge the unique needs and complex nature of this population. This document outlines principles that are felt to represent the most appropriate way to treat older adults at this time. As more data are available, it may require a revision of the outlined principles.
An important aspect of the chiropractic management and treatment of older adults is the high prevalence of chronic musculoskeletal conditions for which both surgical and nonsurgical treatment options are available. As people live longer, it is likely that they will increase their utilization of non-surgical treatments such as chiropractic care. This will create an increased amount of responsibility on chiropractors to be able to differentiate between cases which will respond well to nonsurgical care and those that will require surgery, medication, or other more invasive interventions. Chiropractors who treat older adults need to stay current with the evidence regarding these conditions in order to manage cases appropriately.
Many chiropractors will treat chronic musculoskeletal conditions with a combination of manual therapy and rehabilitative exercise. The use of therapeutic exercises in older adults carries with it some special challenges, such as an appreciation for cardiovascular risks with aerobic exercise, risk of falls with balance exercise, and specialized knowledge of postoperative rehabilitation protocols. Chiropractors who manage older adults should consider taking additional post graduate courses in the principles of geriatric rehabilitation, which provide additional training in this specialized area of therapeutic exercise. Furthermore, chiropractic colleges should increase the number of hours dedicated to geriatric education in their curricula. In addition, postgraduate education on the topic of geriatrics should be offered and more heavily promoted at venues used by practicing chiropractors. Postgraduate education on this topic should also include online or web-based materials to increase accessibility to practicing chiropractors. Additional residency opportunities should be developed and offered through chiropractic educational programs.
Limitations of the Study
There are several limitations of this project, chiefly the fact that these statements represent expert opinion, which is a lower level of evidence than that developed through large experimental and observational studies. However, we feel that using a formal Delphi process which included multiple disciplines, both on the Steering Committee and the Delphi panel, helps to limit possible biases which might be created by practice and educational experience or other factors. Another limitation was that it was beyond the scope of this project to address, in depth, exercise, nutrition, lifestyle change, or other modalities and practices that are within the chiropractic scope of practice. We recommend that future projects address the best practice parameters for these topics.
Conclusion
The chiropractic clinician needs to remain aware of the special needs of the older adult patient, particularly with the use of manual therapies. The use of rehabilitative exercise also requires attention to the special needs of the older patient. Additional coursework and clinical experience with older adult patients during chiropractic training, as well as increased emphasis on such training in postgraduate programs, is recommended to further enhance the profession's capacity to serve this population. If chiropractic care is to become integrated into the health care system in caring for the older adult population, there is also a need for more high quality data on its safety and effectiveness for that population.
Practical Applications
The consensus process using a multidisciplinary panel was successful in developing a set of seed statements concerning the key issues related to chiropractic care for older adults.
This document provides a general framework for what constitutes an evidence-based and reasonable approach to the chiropractic management of older adults.
It should not be seen as a final product but, rather, as a work-in-progress that will require refinement as new evidence emerges in the future.
Funding Sources and Potential Conflicts of Interest
This study was funded by a grant from the NCMIC Foundation. All Delphi panelists served without compensation. There are no conflicts of interest reported by the authors.
Acknowledgment
The authors thank Cathy Evans, Project Coordinator, for successfully managing the complex processes of this project. They thank Raheleh Khorsan, MS, for conducting a very thorough and comprehensive literature search. The project could not have been completed without the generous contributions of many experts. These include the Steering Committee, who were, in addition to the authors: Kathleen Buckwalter, RN, PhD; Gail Jensen, PhD, PT; Claire Johnson, DC, MSEd; Paul Katz, MD; and Jurgis Karuza, MA, PhD. The Delphi panelists were also essential in developing this document. They are: Pamela Adams, DC; Jerrilyn A. Cambron, LMT, DC, PhD; Ezra Cohen, DC, CMT; Catherine Cummins, DC; Connie D'Astolfo, DC; Mark D. Dehen, DC; Ronald J. Farabaugh, DC; Kimary L. Farrar, MS, DC; Katherine T. Hoiriis, DC; Paul D. Hooper, DC, MPH, MSc; Victoria A. Hornyak, PT, DPT; Robert Leach, DC, MS; Stacie Salsbury Lyons, PhD, RN; George B. McClelland, DC; Robert D. Mootz, DC, David R. Odiorne, MS, DC; Stephen M. Perle, DC, MS; Paul J. Osterbauer, DC, MPH; Mark T. Pfefer, RN, MS, DC; Julie A. Plezbert, DC; Simone Simaan, MD, DC; Richard G. Strunk, DC, MS; Leonard Suiter, DC; John A. M. Taylor, DC; Rodger Tepe, PhD; Rickard J. Thomas, DC; Sivarama P. Vinjamury, MD (Ayurveda), MAOM, MPH;
References:
U.S. Census Bureau.
An older and more diverse population by mid-century:
Washington, DC: U.S. Census Bureau; 2008. (Available from)
http://www.census.gov/newsroom/releases/archives/population/cb08-123.htmlChristensen, M, Kollasch, M, Ward, R, Webb, K, Day, A, and ZumBrunnen, J.
Job Analysis of Chiropractic 2005
NBCE, Greeley, CO; 2005United States Bone and Joint Decade.
The Burden of Musculoskeletal Diseases in the United States.
American Academy of Orthopaedic Surgeons, Rosemont IL; 2008American Geriatric Society.
The management of chronic pain in older persons:
AGS panel on chronic pain in older persons.
J Am Geriatr Soc. 1998; 46: 635–651American Geriatric Society.
The management of persistent pain in older persons.
J Am Geriatr Soc. 2002; 50: S205–S224Bronfort G, Haas M, Evans R, Leiniger B, Triano J.
Effectiveness of Manual Therapies: The UK Evidence Report
Chiropractic & Osteopathy 2010 (Feb 25); 18 (1): 3Cassidy, JD, Boyle, E, Cote, P et al.
Risk of Vertebrobasilar Stroke and Chiropractic Care:
Results of a Population-based Case-control
and Case-crossover Study
J Manipulative Physiol Ther. 2009 (Feb); 32 (2 Suppl): S201–208Hurwitz, EL, Morgenstern, H, Vassilaki, M, and Chiang, LM.
Frequency and clinical predictors of adverse reactions to chiropractic care
in the UCLA neck pain study.
Spine. 2005; 30: 1477–1484Gouveia, LO, Castanho, P, and Ferreira, JJ.
Safety of chiropractic interventions: a systematic review.
Spine (Phila Pa 1976). 2009; 34: E405–E413Hawk, C, Rupert, R, Colonvega, M, Boyd, J, and Hall, S.
Comparison of Bio-Energetic Synchronization Technique and
customary chiropractic care for older adults
with chronic musculoskeletal pain.
J Manipulative Physiol Ther. 2006; 29: 540–549Hondras MA, Long CR, Cao Y, et al.
A Randomized Controlled Trial Comparing 2 Types of Spinal Manipulation
and Minimal Conservative Medical Care for Adults 55 Years and Older
With Subacute or Chronic Low Back Pain
J Manipulative Physiol Ther. 2009 (Jun); 32 (5): 330–343Bougie, J.
Geriatric practice-specific issues.
in: S Haldeman (Ed.) Principles and Practice of Chiropractic. 3rd ed.
McGraw-Hill, New York; 2005: 1079–1098Triano, J.
The mechanics of spinal manipulation.
in: W Herzog (Ed.) Clinical Biomechanics of Spinal Manipulation.
Churchill-Livingstone, New York; 2000: 92–190Cooperstein, R, Perle, SM, Gatterman, MI, Lantz, C, and Schneider, MJ.
Chiropractic technique procedures for specific low back conditions:
characterizing the literature.
J Manipulative Physiol Ther. 2001; 24: 407–424Cooperstein, R and Gleberzon, B.J.
Diversified technique.
in: R Cooperstein, B.J. Gleberzon (Eds.) Technique Systems in Chiropractic. 1st ed.
Edinburgh, Churchill-Livingstone; 2004: 143–149Forster, A, Lambley, R, Hardy, J et al.
Rehabilitation for older people in long-term care.
Cochrane Database Syst Rev. 2009; : CD004294Howe, TE, Rochester, L, Jackson, A, Banks, PM, and Blair, VA.
Exercise for improving balance in older people.
Cochrane Database Syst Rev. 2007; : CD004963Liu, CJ and Latham, NK.
Progressive resistance strength training for improving physical function in older adults.
Cochrane Database Syst Rev. 2009; : CD002759Robitaille, Y, Laforest, S, Fournier, M et al.
Moving forward in fall prevention: an intervention to improve balance
among older adults in real-world settings.
Am J Public Health. 2005; 95: 2049Lin, MR, Wolf, SL, Hwang, HF, Gong, SY, and Chen, CY.
A randomized, controlled trial of fall prevention programs
and quality of life in older fallers.
J Am Geriatr Soc. 2007; 55: 499–506American Geriatric Society.
Guideline for the prevention of falls in older persons.
J Am Geriatr Soc. 2001; 49: 664–672American Geriatric Society.
Exercise prescription for older adults with osteoarthritis pain:
consensus practice recommendations.
J Am Geriatr Soc. 2001; 49: 808–823Ganz, DA, Alkema, GE, and Wu, S.
It takes a village to prevent falls:
reconceptualizing fall prevention and management for older adults.
Inj Prev. 2008; 14: 266–271AHRQ.
Adult preventive care timeline.
Agency for Healthcare Research and Quality, ; 2006
(AHRQ Publication No. APPIP06-IP001, June 2006.
Agency for Healthcare Research and Quality, Rockville, MD)
http://www.ahrq.gov/ppip/timelinead.htm.Council on Chiropractic Education.
Standards for Doctor of Chiropractic Programs and requirements for institutional status.
Council on Chiropractic Education, ; 2007Borggren, CL, Osterbauer, PJ, and Wiles, MR.
A survey of geriatrics courses in North American chiropractic programs.
J Chiropr Educ. 2009; 23: 28–35Bougie, J and Morgenthal, JP.
The aging: conservative management of common neuromusculoskeletal conditions.
McGraw-Hill, New York; 2001Gleberzon, BJ.
Chiropractic care of the older patient.
Butterworth-Heinemann, Oxford; 2001Killinger, LZ.
Chiropractic and geriatrics: a review of the training, role, and scope
of chiropractic in caring for aging patients.
Clin Geriatr Med. 2004; 20: 223–235Hawk, C, Killinger, Z, Zapotocky, B, and Azad, A.
Chiropractic training in care of the geriatric patient: an assessment.
J Neuromusculoskelet Syst. 1997; 5: 15–25Hawk, C, Byrd, L, and Killinger, LZ.
Evaluation of a geriatrics course emphasizing interdisciplinary issues
for chiropractic students.
J Gerontol Nurs. 2001; 27: 6–12Manchikanti, L, Boswell, MV, and Giordano, J.
Evidence-based interventional pain management:
principles, problems, potential and applications.
Pain Physician. 2007; 10: 329–356Driever, MJ.
Are evidence-based practice and best practice the same?
West J Nurs Res. 2002; 24: 591–597Fitch, K, Bernstein, SJ, Aquilar, MS, Burnand, B,
LaCalle, JR, Lazaro, P, van het Loo, M, McDonnell, J, Vader, J, and Kahan, JP.
The RAND UCLA Appropriateness Method User's Manual.
RAND Corp, Santa Monica, CA; 2003Maiers M, Hartvigsen J, Schulz C, Schulz K, Evans R, Bronfort G.
Chiropractic and Exercise for Seniors With Low Back Pain or Neck Pain:
The Design of Two Randomized Clinical Trials
BMC Musculoskelet Disord. 2007 (Sep 18); 8: 94Dougherty, P and Killlinger, LZ.
The role of chiropractic in long term care.
Long Term Care Interface. 2005; 6: 33–38Centers for Medicare and Medicaid Services.
Medicare program; revisions to payment policies under the physician fee schedule,
and other Part B payment policies for CY 2008.
Federal Register. 2007; : 66221–66578Chou R, Qaseem A, Snow V, Casey D, Cross JT Jr., Shekelle P, Owens DK:
Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline
from the American College of Physicians and the American Pain Society
Annals of Internal Medicine 2007 (Oct 2); 147 (7): 478–491
Return to MEDICARE
Return to SENIOR CARE
Return to BEST PRACTICES
Since 2–28–2016
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |