

Prevalence of Musculoskeletal Dysfunction in Infants
Presenting for Chiropractic Care in Norway:
A Cross-sectional StudyThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Clinical Chiropractic Pediatrics 2017 (Sep); 16 (1): 1355–1361 ~ FULL TEXT
OPEN ACCESS Catherin Alvestad Slettebo, DC, MSc, Joyce E. Miller, DC, PhD
AECC University,
Bournemouth, UKBackground: Musculoskeletal (MSK) injuries are common though considered under-recognized at birth. There are no gold standard routines for examination of the musculoskeletal system in infants, and very little research that investigates clinical examination and MSK findings in infants under the age of six months.
Objectives: The objectives were to determine the prevalence of neck dysfunction, postural spine problems, and their possible association with parent reported behavioral problems such as suboptimal breastfeeding and supine sleeping in infants younger than six months of age. The aim of this study was to observe any associations between MSK problems of infancy and common behavioral and public health issues. Methods: This is a cross sectional questionnaire based observational study in a clinical population. Mothers of infants presented to chiropractic clinics in Norway filled in a questionnaire on the first visit, and this was followed by a clinical examination and questionnaire completed by the Doctors of Chiropractic on the same day.
Results: In total, 90 infants enrolled in the study. A total of 56 infants (66%) had postural problems. Favorite side of cervical rotation (N=41; 75%) was the most common dysfunction in supine lying. Neck hyperextension was present in 21 infants (38%). The inability to rotate their head equally side to side was present in 49 children (54%). In total 22 (24%) of the infants did not have the ability to sleep or lie comfortably supine. Suboptimal breastfeeding was reported by 22 (25%) parents, and 10 (12%) of the mothers reported pain during feeding. TMJ imbalance was identified in 16 infants (19%). There were statistically significant associations between suboptimal breastfeeding and TMJ imbalance, suboptimal rooting/sucking reflexes, inability to turn head and neck equally and painful breastfeeding, respectively.
Conclusion: Parents reported several MSK problems in infants along with suboptimal breastfeeding and other ADLs, which were corroborated and specified by the clinical examination. More study is needed to determine a gold standard reference for infant musculoskeletal examinations along with the importance in improving activities of daily living and public health through balance of the MSK system.
Keywords: cervical spine dysfunction, musculoskeletal injuries, musculoskeletal problems, musculoskeletal examination, breastfeeding problems, supine sleep, infants, pediatrics, chiropractic.
From the FULL TEXT Article:
Introduction
Mild to moderate musculoskeletal injuries are common at birth, but frequently missed. [1] Although these injuries are common, their association with quality of life conditions like sleeping, feeding or excessive crying may not always be understood in professional practice. However, birth injuries are implicated in infant complaints. For example, a difficult birth has the highest association with infant colic (now known as excessive crying) than any other factor. [2]
Further, birth injury is implicated in suboptimal breastfeeding. [3–6] Breastfeeding is one of the key factors in improved health for the infant and mother, [7, 8] and although Initiation might be high, early discontinuation is a trend if the mothers experience problems, discomfort or pain with feeding. [9] A recent study in England on dyads with feeding problems showed that cessation of breastfeeding occurs early within three weeks of age. [10] It is suggested that the infant is the cause in 59% of feeding problems. [11] However, this has been disputed as being much higher (85%) in more current research. [12] It is therefore essential to assess biomechanical problems early in infants to detect any musculoskeletal problems that might influence breastfeeding. In addition to good sucking, rooting and swallowing reflexes, the infant needs appropriate and supportive posture and adequate cervical spine range of motion to establish sufficient breastfeeding. The newborn uses six cranial nerves, 22 bones connecting to 34 sutures, and 60 voluntary and involuntary muscles in order to suck swallow and breathe. [6] Doctors of chiropractic may contribute to this important task in light of the anatomy and biomechanical problems involved. [4, 13–22]
There is a need for more precise and early assessment of the newborn infant, with a full clinical examination including biomechanical features like examination of the infant’s neck and spine, cranium, and TMJ in addition to postural assessment, primitive reflexes (for example suck and rooting reflexes) and appropriate neurological examinations. These examinations are routine in chiropractic practice but the findings have not previously been documented in the research literature. This is key to further understanding of any association of observational findings with parent reports of behaviors.
This study was designed to specifically look at the prevalence of neck dysfunction, and other biomechanical problems in the infant that may be associated with suboptimal breastfeeding and other key ADLs. The chief goal of this study was to track routine clinical practice of infant care in chiropractic practices in Norway, by documenting and comparing parent report of infant problems and doctor of chiropractor’s clinical findings.
Methods
The study was an observational cross-sectional study of infants routinely presented to a chiropractic clinic. Inclusion criteria were infants who were presented by their parents with a clinical complaint and who consented. Exclusion criteria were parents who did not wish their child to be included. The study was completely anonymous and no identifying data was kept except in the routine legal way as it is always kept in each clinic. Doctors of chiropractors collected the study data in multidisciplinary clinics in Norway. The chiropractic providers had a certificate in pediatric treatment, or were undertaking a professional program like MSc Advanced Professional Practice in Pediatrics.
The study included a parent questionnaire and an examination by a doctor of chiropractic. The chiropractic examination in this study was divided into five parts:Neck dysfunction,
postural problems,
suck and rooting dysfunctions,
TMJ dysfunction and
other dysfunction present (but not assessed in detail in the study).The chiropractic examination evaluated neck function based on passive cervical rotational motion, occipital glide test and neck flexion rotation test, as well as palpation for tender spots in upper and lower cervical spine. A detailed list of clinical examinations and instructions were given to each doctor of chiropractic.
The study did not differ from routine clinical practice. There were no interventions and there were no measurements before or after treatment, as part of the study. The data was collected in infants aged 0–6 months, on their first consultation at chiropractic offices in Norway. All data collection material was either sent to the participating chiropractors electronically ready to print, or by post already printed. The data was collected from end of January 2016 until end of April 2016. The study was registered with REK (Regionale komiteer for medisinsk helsefaglig forskningsteknikk), a regional study ethics committee in Norway. No further ethical oversight was required.
All infants were examined and measured once in this study. The data were first entered into an Excel spreadsheet and then exported to SPSS where appropriate statistical analysis could be undertaken. Each row in the spreadsheet contained the answer set from a given respondent, and each column would represent a question in the questionnaire (variables). Blank cells were questions that respondents did not answer. To determine if there was an association between dysfunctions and breastfeeding in infants less than four months of age, we used Pearson Chi-Square test.
Selective answers to questions are always a limitation in this type of study; six mothers did not answer the questions regarding breastfeeding issues. The reason for this can be is that they already had terminated the breastfeeding. The mothers could therefore have problems answering these questions. The questionnaire should have included a question to identify if the mother had stopped breastfeeding due to conditions related to fuss, or difficulties in the breastfeeding situation. One doctor of chiropractic did report a few missing questionnaires and a few practitioners did leave a blank cell on the examination section. Otherwise there were no further problems filling in the questionnaires.
Results
Population: Gender, age and type of birth
In total, 90 infants enrolled in the study. A total of 56 (66%) infants had postural problems. Forty-two (47%) of the participants were male and 47 (53%) were female. The mean age was 8.2 weeks. The most common age at presentation was two weeks. Out of 90 infants 46 (51%) had a normal vaginal birth, and 44 (49%) of the infants had an assisted birth.
Presenting chief complaints
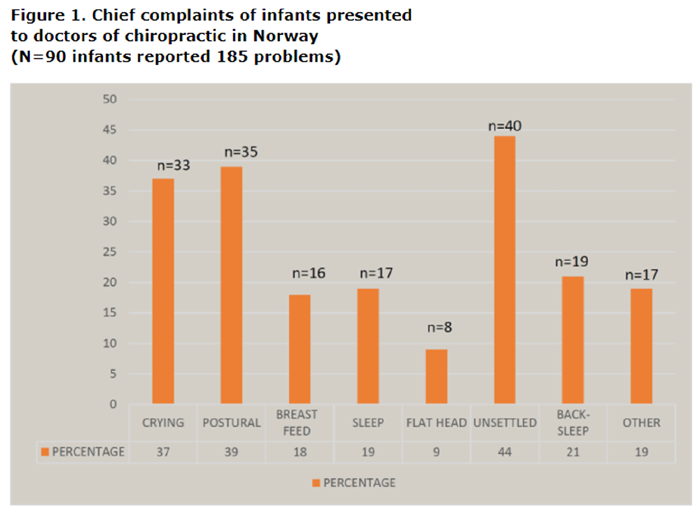
Figure 1
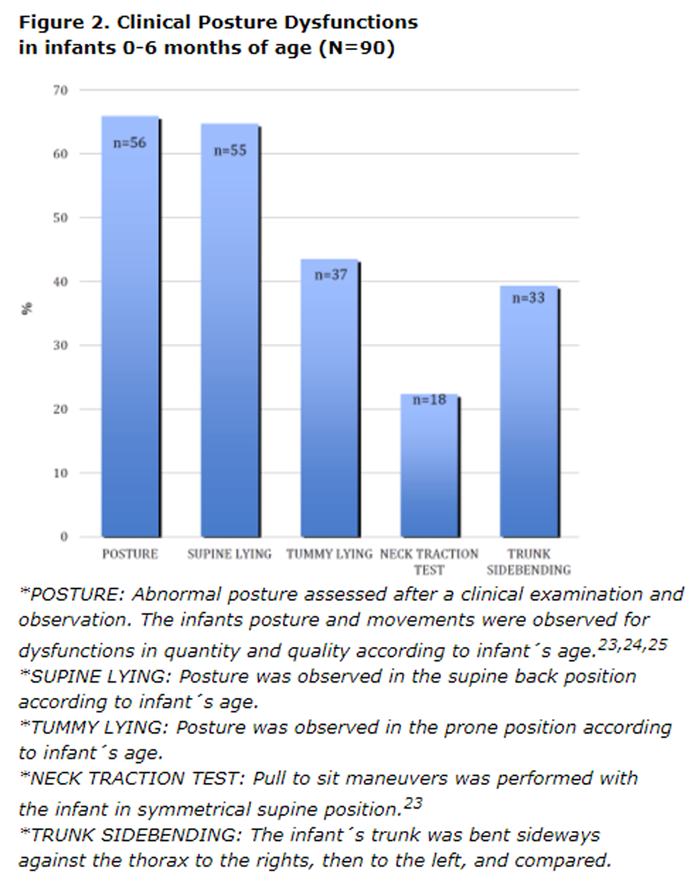
Figure 2
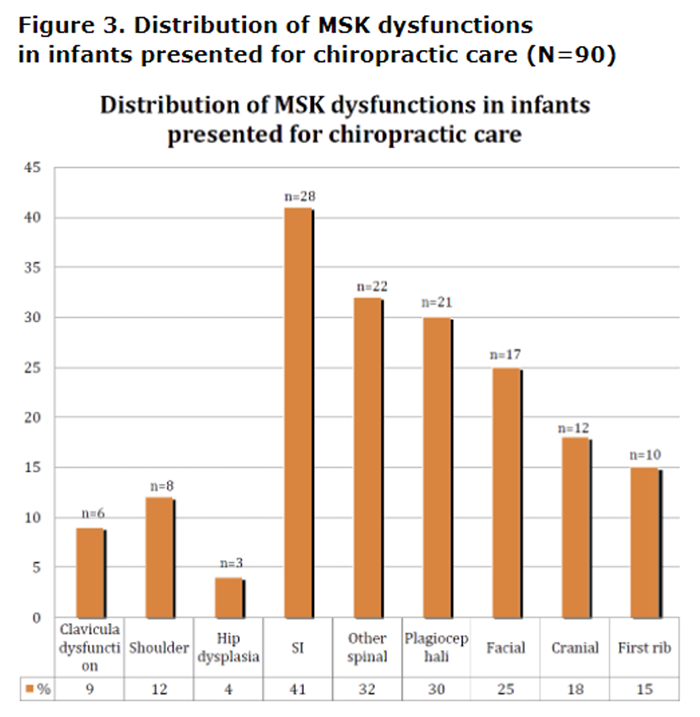
Figure 3

Table 1 Parents could report as many problems as the child had. Therefore, there were sometimes multiple complaints for each infant. The most common complaint and reason for seeking chiropractic was unsettled baby (n=40, 44%), followed by postural problem (n=35, 39%) and crying (n=33, 37%). Breastfeeding problems were reported in 16 (18%) infants as the presenting complaint (Figure 1).
Parent reported behaviors
Twenty-two of the mothers (25%) reported breastfeeding problems, and another 10 (12%) mothers reported pain during feeding. Thirty (36%) of the infants had a favorite side during feeding. There were 49 (54%) parents who reported that their child could not turn their head and neck equally to both sides. Uncomfortable supine sleep was reported in 22 (24%) infants. Another 37 (42%) infants had a problem with tummy time. Regarding breastfeeding, 59 of the infants were “100% breastfed,” 13(14%) were “75% breastfed” and 18 (20%) were receiving “50%” or less feeding from the breast.
Postural clinical examination findings
After a clinical assessment, abnormal postural findings [23–25] were present in 56 (66%) infants. Neck dysfunctions found by clinical chiropractic examinations were present in 74 (87%) out of 90 infants. Also 55 (65%) infants did not have normal supine posture for his/her age. Favorite side of the neck and head (n=41; 73%) was the most common finding, second was neck hyperextension (n=21; 38%), third was trunk hyperextension (n=11; 20%), followed by hip asymmetry (n=5; 9%) and multiple malpositions (n=6; 11 %) when assessing posture dysfunctions in supine lying. Postural problems are depicted in Figure 2.
Dysfunctional suck reflex, rooting reflex and TMJ imbalance
Dysfunctional suck reflex was identified in 17 (19%) infants under the age of 4 months. Abnormal rooting reflex was present in 12 (14%) subjects. The clinicians found 16 (19%) patients with TMJ imbalance. There were many other MSK dysfunctions identified in this study (Figure 3).
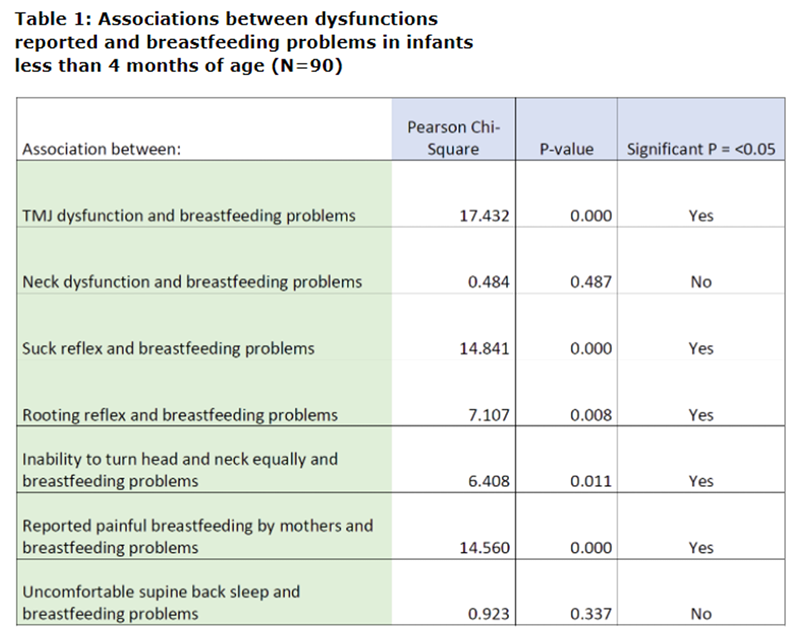
An analysis of the association between the infant's inability to turn equally his/her neck to both sides and breastfeeding was significant, with Pearson Chi-Square value of 6.408 and p-value of 0.011. Also, there were statistically significant associations between suboptimal breastfeeding and TMJ imbalance, suboptimal rooting/sucking reflexes, and painful breastfeeding, respectively (Table 1).
Discussion
This is the first study to investigate musculoskeletal (MSK) presentation, examination and findings that describe common chiropractic pediatric practice. Since transitioning to certain postures at specific ages are important for reaching milestones and methodical development in children, 25 postural assessments were considered important in this examination. It is key to identify the infant’s quantity and quality of movements and postures when assessing infants under the age of six months. Mothers had excellent ability to identify postural problems in their own infant. Postural problems were the second most common reason for seeking chiropractic help for their child in this study, comprising just under half of the complaints. Furthermore, mothers noticed postural problems early with the most common age of presentation at two weeks.
As such, there were several MSK problems identified by mothers, all of which could and did affect important infant activities of daily living (ADLs) such as breastfeeding, supine sleep and full and equal cervical spine rotation. Since sleep and feeding are the major occupations for a newborn, these are key ADLs for optimal development and as such, are important public health issues; the same could be argued for cervical spine rotation as inability may result in positional plagiocephaly, a risk for developmental delay. [26–28]
Unsettled baby was a main complaint registered by nearly half of the parents in the study. Slightly fewer parents reported crying as a chief complaint. Often parents reported that these problems go hand in hand. These also coincided with postural problems. It is logical that there is a link to postural problems as a baby who cannot get into a comfortable position is likely to be characterized as unsettled by the parents. With a mean age for this population of eight weeks, this is considered a time when parents have noticed excessive crying and/or unsettled behavior and/or postural preferences, have found no remedy and thus, present to a chiropractor. This correlates with other research literature, [29] which suggest that chiropractic care may be the last port of call for infant complaints. This population further corroborates the research literature as half of the births had been assisted, and does suggest a high rate of complicated births among patients seeking chiropractic care. Babies with assisted births are more likely to have postural problems and excessive crying. [1, 2, 12] Another study that looked at maternal report of feeding practice, [10] found that more than half of infants who stopped breastfeeding reported an assisted birth.
A focus of this study was the prevalence of infant problems, which are public health concerns for the short and long-term health of the baby. Three of these are breastfeeding, ability to sleep supine, and head shape. Together these comprised a third of the study population. This is a place where chiropractic care can help to shoulder the major burden of public health problems for infants and restore these children to full function to prevent long-term problems. Chiropractic care has been shown to assist mothers to continue breastfeeding, [4, 10, 12, 30–32] supine sleep [33, 34] and head shape. [13, 35] Even though the complaints of positional head deformation were low (under 10%), more than half of the babies had difficulties rotating their head equally to both sides. If this condition is not corrected, then the head shape problems are likely to develop. [28, 36] Further, there is evidence that developing plagiocephaly can result in breastfeeding problems and is associated with long-term developmental problems. [37, 38] It was interesting that only two-thirds of the mothers totally breastfed their baby in this study. Considering this study was in Norway, a country known for one of the highest rates of total breastfeeding in the world, and one-third of the mothers were unable to totally breastfeed their newborn indicates a big problem for the dyad and society which has not been widely reported previously.
A study like this has several limitations. One weakness of the study is that there were many examiners performing tests, and inter-examiner reliability can be questioned. However, this could be a strength as well and it did reflect routine practice. Many of the examinations in the study allowed for subjective judgments, although the prescriptive description has taken as much personal judgment as possible out of the equation. Another limitation is that examination signs such as decreased active and passive range of motion are proven to indicate upper neck dysfunction in adults, but not studied in children. [39–41] It is suggested that these tests can be valid in children too, although with different normal values. [42, 43]
Studies have shown that an infant needs to achieve skills typical for a three-month-old baby for proper development. [23–25] It is of value to assess abnormal postures in early life, especially with focus on infants below three months of age. It is therefore of interest that nearly two-thirds of the children in this study had abnormal supine posture, and that almost 40% of the parents did identify postural problem as a main complaint. If postural impediments can be removed early, it is likely that normal development can ensue with re-building of any aberrant neurological pathways. [25, 44] Also, uncomfortable postures can reduce quality of sleeping. [45] Of course, supine position is required to reduce the risk of SIDS and supine sleep is seven times safer than any other position. [46] Parents are aware of the problem and reported uncomfortable supine sleep in one-quarter of the children. This is a major area for chiropractors to positively impact the public health.
The neck has an important role in the natural postural development and milestone achievements. [25] This group of patients did have a very high frequency of cervical spine dysfunction (87%). This could be viewed as over-identification. However, some prior studies have also found the same trend in patients seeking chiropractic care. [3, 4, 21, 30, 32, 47] The parents in this study identified several MSK problems, including the inability to turn the head and neck equally to both sides. Parents are keen observers of their infant and they recognize these postural problems early. [33]
One key finding in this study was a significant association between the infant´s ability to equally turn his/her neck to both sides with breastfeeding problems. This has not been previously documented. Another interesting finding was that more than one-third of the mothers reported that their infants had a favorite breast during breastfeeding. Evidence has suggested a clinical rationale for addressing the cervical spine and chiropractic assessment in infants with suboptimal breastfeeding. [3, 4, 30–32, 47] Neck dysfunction was found in most of the infants, as were palpation findings in the neck. These findings were further identified by orthopedic tests (cervical flexion rotation test [49–53] and occipital glide test [54]). There is no definite theory for the cause of reduced neck rotation. The ability to turn the head equally is not the same as torticollis, generally caused by muscle involvement whereas the former is often caused by dysfunctional cervical joint motion, something, which can be easily corrected with skilled chiropractic techniques.
Future research should focus on which clinical examinations have the highest sensitivity and specificity to detect infant MSK problems that most commonly lead to disruption in normal ADLs. Reliability of different clinical examinations like neck flexion rotation test, occipital glide test, and trunk flexion test in infants requires further study. Researches into orthopedic tests are important because there is a demand for reproducible tests when assessing infants. Reliable and valid examination procedures are required to create a gold standard musculoskeletal examination for the infant patient.
Conclusion
Parents were able to identify and report musculoskeletal problems in infants along with irritability, crying, suboptimal breastfeeding and other ADLs, which were corroborated and specified by the clinical examination. More study is needed to determine a gold standard reference for infant musculoskeletal examinations along with their implications in improving activities of daily living and public health.
References:
Stellwagen I, Hubbard E, Chambers C, Jones.
Torticollis, facial asymmetry and plagiocephaly in normal newborns.
Archives of Disease in Childhood 2008; 93, (10): 827-31.Zwart P,Vellema-Goud M, Brand, LP.
Characteristics of infants admitted to hospital for persistent colic, and comparison with healthy infants.
Acta Paediatrica 2007; 96:401-405. DOI:10.1111/j.1651-2227.2007.00090.Vallone S.
Evaluation and Treatment of Breastfeeding Difficulties Associated with
Cervicocranial Dysfunction: A Chiropractic Perspective
Journal of Clinical Chiropractic Pediatrics 2016 (Dec); 15 (3): 1301–1306Alcantara J, Alcantara JD, Alcantara, JU.
The Chiropractic Care of Infants with Breastfeeding Difficulties
Explore (NY) (Nov) 2015; 11 (6): 468–474Holtrop DP.
Resolution of Suckling Intolerance in a 6-month-old Chiropractic Patient
J Manipulative Physiol Ther 2000 (Nov); 23 (9): 615–618Smith LJ.
Impact of birthing practices on the breastfeeding Dyad.
J of Midwifery and Women´s Health 2007; 52,(6): 621-30.Jackson KM, Nazar AM.
Breastfeeding, the immune response, and long- term health
Am Osteopath Assoc. 2006; 106.203-7.Rollins NC, Bhandari N, Hajeebhoy, et al.
Why invest, and what it will take to improve breastfeeding practices?
The Lancet 2016; 387:491–504.Miller J, Miller L, Sulesund, A-K, Yevtushenko A.
Contribution of Chiropractic Therapy to Resolving Suboptimal Breastfeeding:
A Case Series of 114 Infants
J Manipulative Physiol Ther 2009 (Oct); 32 (8): 670–674Homdrum AKS, Miller J.
Maternal rapport of feeding practise: a cross-sectional survey of 1753 mothers presenting infants to a chiropractic-teaching clinic.
Journal of Clinical Chiropractic Pediatrics 2015; vol.15: 1Lawrence R.
Breastfeeding: a guide for medical profession.
Chicago: Mosby. 1994.Miller J, Beharie MC, Taylor AM, Simmenes EB, Way S.
Parent Reports of Exclusive Breastfeeding After Attending a Combined Midwifery and
Chiropractic Feeding Clinic in the United Kingdom: A Cross-Sectional Service Evaluation
J Evid Based Complementary Altern Med. 2016 (Apr); 21 (2): 85–91Collins K, Alcantara J, Holt K.
Resolution of Breastfeeding and Gastrointestinal Complaints in Infants Twins with Plagiocephaly & Scaphocephaly Following Birth Trauma; A Case series.
J. Pediatric, Maternal & Family Health 2015; February 10: 34-41.Drobbin D, Stallman J.
Resolution of Breastfeeding and Latching Difficulty Following Subluxation Based Chiropractic Care: Case Report and review of the Literature.
J Pediatric, Maternal & Family Health 2015; July: 102-108.Neally R, Alcantara J.
Resolution of failure to Thrive in a 4-Month-Old Infant Following Adjustments of Subluxation: Case Study & Selective review of the Literature.
J Pediatric, Maternal & Family Health 2015; December 17:149-152.Fry LM.
Chiropractic and Breastfeeding Dysfunction: A Literature Review
Journal of Clinical Chiropractic Pediatrics 2014 (Mar); 14 (2): 1151-1155Bernard M, Alcantara J.
The chiropractic care of a 6 days-old neonate with Breastfeeding Difficulties and Breastfeeding Jaundice.
Chiropractic Journal of Australia 2012; 42,3,9: 108-113.Hubbard MA.
Pediatric cholelithiasis and breastfeeding difficulties: A Chiropractic report.
Journal of Clinical Chiropractic Pediatrics 2014; March: 114-1150.Tutt GM, Mesidor RG.
Resolution of torticollis, Plagiocephaly & Breastfeeding Difficulties in an Infant Following Subluxation Based Chiropractic Care.
J Pediatric, Maternal & Family Health 2014; April: 14-20.Slak L, Wilson KA.
Resolution of Breastfeeding Difficulty Following Subluxation Based Chiropractic Care.
J Pediatric, Maternal & Family Health 202013; January 17: 7-10.Stewart A.
Paediatric chiropractic and Infant Breastfeeding difficulties. A pilot Case Series Involving 19 cases.
Chirpr H Aust. 2012; 42:98-107.Lavigne V.
A Narrative Review and case report: Frenotomy Procedure in Neonate with Tongue-tie.
Journal of Clinical Chiropractic Pediatrics 2012; 2, December: 1025-32.Prechtl HFR.
Development of postural control in infancy.
In: Von Euler C, Forssberg H, Lagercrantz H, editors.
Neurobiology of Infant Behaviour 1989; Vol.5.Einspieler C, Cioni G, Paolicelli PB.
The early markers for later dyskinetic cerebral palsy and different from those for spastic cerebral palsy.
Neuropediatrics 2002; 33, (2): 73-78.Gajewska E, Sobieska M, Kaczmarek, Suwalska A, Steinborn B.
Achieving Motor development Milestones at the Age of Three Months may determine but Does Not Guarantee, proper Further development.
Scientific World Journal 2013; 354218Martiniuk AL, Vujovich-Dunn D, Park M, Yu W, Lucas BR.
Plagiocephaly and Developmental Delay. A Systematic Review.
J Dev Behav Pediatr. 2017; 38,1:67-78Mawji RN, Vollman A, Fung T, Hatfield J, McNeil D A, Sauvé R.
risk factors for positional plagiocephaly and appropriate time frames for preventing massage.
Pediatr Child Health 2014; 19,8:423-427.Leung AY, Mandrusiak A, Watter P, Gavranich J, Johnston lM.
Clinical assessment of head orientation profile development and its healthy term infants: A prospective study.
Early Hum Dev, May 2016; 96: 31-8Miller J, Newell D.
Prognostic significance of subgroups classification for infant patients with crying disorders: A prospective cohort study.
Can Chiropr Assoc. 2012; 25, (1):40-48.Miller J, Miller, L, Sulesund, A-K, Yevtushenko, A., 2009.
Contribution of Chiropractic Therapy to Resolving Suboptimal Breastfeeding:
A Case Series of 114 Infants
J Manipulative Physiol Ther 2009 (Oct); 32 (8): 670–674Tow J, Vallone, SA.
Development of an integrative relationship in the chiropractic care of breastfeeding newborn: lactation consultant and chiropractor.
J Clin Chiropr Pediat. 2009; 626-632.Vallone S.
Chiropractic Evaluation and Treatment of Musculoskeletal Dysfunction
in Infants Demonstrating Difficulty Breastfeeding
J Clinical Chiropractic Pediatrics 2004 (Dec); 6 (1): 349–366Nicolas-Schmid P, Hetlevik MA, Miller J.
Infants presentations and outcome at a chiropractic clinic in the UK: Parent report of treatment outcomes using the United Kingdom Infant Questionnaire UKIQ).
JCCP 2016; 15:1236-141.Wright C, Beard H, Coc J, Scott P, Miller J.
Parents ‘choices of non-supine sleep position for newborns: A cross-sectional study.
Journal of Health Visiting 2014; 9, 2,9:500-504.Douglas NA, Browning M, Miller J. 2016.
Chiropractic care for the Cervical Spine as a treatment for plagiocephaly.
J Clin Chiropr Pediat. December 2016; 15,3:1272-1278.Philippi H, Faldun A, Jung T, Bergman H, Bauer K, Groß D.
Patterns of infantile postural asymmetry: A standardizes video-based analysis.
Neuropediatrics 2005; 36-117. DOI: 10.1055/s-2005-868102.Lal S, Abbasi AS, Jamro S.
Responses to Primary Torticollis Physiotherapy.
Journal of Surgery Pakistan (International) 2011; 16,4:153-156.Wei JL, Schwatz KM, Weaver AL, Orvidas l.
Pseudotumor of infancy and congenital muscular torticollis.
Laryngoscope 2001; 111:688-90.Jull G, Amiri M, Bullock-Saxton J, Darnell R, Lander C.
Cervical Musculoskeletal Impairment in Frequent Intermittent Headache.
Part 1: Subjects with Single Headaches
Cephalalgia 2007 (Jul); 27 (7): 793–802Zito G, Jull G, Story I.
Clinical tests of musculoskeletal dysfunctions in the diagnosis of cervicogenic headache.
Man Ther. 2006; 11:118-154.Zwart JA.
Neck mobility in different headache disorders.
Headache 1997; 3: 6-11.Arbogast KB, Gholve PA, Fridman JE, Maltese MR, Tomasello MF, Dormans JP.
Normal cervical spine range of motion in children 3-12 years.
Spine 2007; 32: E309-E315.Lynch-Caris T, Majeske KD, Brelin-Fornari J, Nashi S.
Establishing references values for cervical spine range of motion in pre-pubescent children.
J Biomech. 2008; 41: 2714-2719.Jung M W m Landenberg M, Jung T, Lindenthal T, Philippi H.
Vojta therapy and neurodevelopment treatment in children with infantile postural asymmetry: a randomised controlled trial.
J. Phys. Ther. Sci. 2017; 29, 29:301-306Modesto IF, Avelar AFA, Pedreira MLG, Pradella-Hallinan, M, Avena MJ, Pinheiro EM.
Effect of sleeping Position on Arousals From Sleep in preterm Infant.
Journal for Specialists in Pediatric Nursing 2016; 1,8Gunn AJ, Gunn TR, Mitchell EA.
Is changing the sleep environment enough? Current recommendations for SIDS.
Sleep Med Rev. 2000; 4,(1):453-69.Holleman A, Nee J, Knaap SF.
Chiropractic management of breastfeeding difficulties: a case report.
J Chiropr. Med. 2011; 10,3:199-203Monson RM, Deitz J, Kartin D.
The relationship between awake positioning and motor performance among infants who slept supine.
Pediatrics Physical Therapy 2003; 15:196-203.Budelmann K, von Piekartz H, Hall T.
Is There a Difference in Head Posture and Cervical Spine Movement
in Children With and Without Pediatric Headache?
European Journal of Pediatrics 2013 (Oct); 172 (10): 1349–1356Hall T, Briffa K, Hopper D.
The influence of the lower cervical joint pain on range of motion and interpretation of flexion-rotation test.
J Man Manip Ther. 2010; 18, 3:126-202.Hall T, Briffa K, Hopper D, Robinson K.
The relationship between cervicogenic headache and impairment determined by flexion-rotation test.
J Orthop Sports Phys Ther. 2010; 40,4: 225-229.Hall T, Briffa K, Hopper D, Robinson K.
Long term stability and minimal detectable change of the cervical flexion-rotation test.
J Orthop Sports Phys Ther. 2010; 40,4:225-229.Hall TM, Robinson KW, Fujinawa O, Akasaka K, Pyne EA.
Intertester Reliability and Diagnostic Validity of the Cervical Flexion-Rotation Test
J Manipulative Physiol Ther 2008 (May); 31 (4): 293–300Beyer B, Sobczak S, Salem W, Feipel V, Dugailly PM.
3D motion reliability of occipital condylar glide testing: From concepts to kinematics evidence.
Manual Therapy 2015; 1-6.
Return to PEDIATRICS
Since 11-16-2017
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |