

Geriatric Chiropractic Care as a Health Promotion
and Disease Prevention Initiative:
Focus on Fall PreventionThis section was compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Topics in Integrative Health Care 2010 (Dec 30); 1 (2) ~ FULL TEXT
OPEN ACCESS Brian J. Gleberzon DC, MHSc
Canadian Memorial Chiropractic College
Toronto, Ontario, CanadaThe chiropractic profession is well positioned to align itself with the principles of health promotion and disease prevention championed by the World Health Organization. As a means to explain how chiropractic practice models and the WHO position statements can converge, this article will use the example of fall prevention. This article will discuss the epidemiology, risk factors, patient assessment tools and preventive strategies of falls prevention for older patients.
From the FULL TEXT Article
Introduction
Various professional advocacy groups tend to support one of two different positions for the chiropractic profession in health care. One group tends to advocate for a spinal care specialty model, [1] principally focusing on neuromusculoskeletal conditions, whereas opposing groups advocate for a broader, wellness paradigm. [2, 3] However, members from all points on the ideological compass can agree that chiropractic care, particularly for older adults, must go beyond the immediate clinical encounter and incorporate the principles of health promotion and disease prevention. This is due to the fact that study after study confirms that chronic diseases that target older patients drastically imperil their health, life expectancy and ability to live independently. These include diabetes, hypertension, osteoarthritis, osteoporosis, asthma, stroke, cognitive impairment and depression, and it is imperative to consider that these diseases can be ameliorated by practitioners who adopt the principles of health promotion and prevention promulgated by the World Health Organization (WHO). By practicing these principles, the chiropractic profession can make important contributions to many contemporary health issues; not only the diseases listed above, but also an area of healthcare of particular relevance to the elderly: fall prevention.

Table 1 WHO has defined health as “a state of complete physical, social and mental wellbeing and not merely the absence of disease or infirmity.” [4] This aligns easily with conventional chiropractic principles [5, 6] since both emphasize a holistic, biopsychosocial approach to health care that encourages patients to adopt healthful life style activities, ranging from not smoking to eating well to engaging in physical activity. [1, 7] (Table 1) These healthful lifestyle behaviors are particularly important among older patients. This matches the compression of morbidity witnessed in many seniors, wherein chronic debilitating diseases are condensed towards the end of a person’s life. [8]
Along the same lines, the WHO defines health promotion as “the process of enabling people to increase control over, and to improve, their health.” [9] Consistent with this process, chiropractors often encourage their patients to be active participants in their health care planning, thus de-emphasizing the traditional patriarchal role of health care providers; this is also consistent with the principle of evidence-based medicine, that patient preferences be included in clinical decision-making. [10–14]
Lastly, disease prevention has been defined by WHO as “measures not only to prevent the occurrence of disease, such as risk factor reduction, but also to arrest the progress and reduce its consequences once established.” [4] As mentioned above, healthful lifestyle approaches championed by private practitioners meet this goal, with weight bearing exercise and nutrition being particularly useful to either thwart the development or prevent the worsening of conditions such as diabetes, heart disease, chronic obstructive pulmonary disease (COPD), osteoporosis or osteoarthritis. [1, 7, 15] In addition, chiropractors have long posited that joint motion preservation (provided by mobilization or spinal adjusting) can prevent, limit or perhaps even reverse osteoarthritis, although there is as yet little definitive support for this hypothesis. [16, 17]
Chiropractic can play a vital role in another important area of prevention: falls prevention. The balance of this article will describe the epidemiology, risk factors, preventive strategies and the role chiropractic care can play to prevent falls among seniors.
Epidemiology of Falls among Seniors
The recently published Report on Seniors’ Falls in Canada by the Public Health Agency of Canada (PHAC) defined a fall as, “a sudden and unintentional change in position resulting in an individual landing at a lower level such as on an object, the floor, or the ground, with or without injury.” [18] Rubinstein asserted that unintentional injuries are the fifth leading cause of death in older adults, and falls constitute two-thirds of these deaths. [19] By age 65 years, roughly one out of three community-dwelling seniors falls annually; this number approaches 50% for institutionalized seniors or seniors over the age of 85 years. [18, 19] Unlike when a child or athlete falls, an older person who falls tends to suffer significant injuries because of an increased susceptibility due to a high prevalence of clinical diseases (most notably osteoporosis) and age-related physiological changes (such as slower protective reflexes). [19] One author calculated that seniors who fall are fall are 10 times more likely to be hospitalized and 8 times more likely to die than are children who fall. [20] In addition, recovery from a fall-related injury is often prolonged or incomplete, which in turn leads to a worsening of fall-related risk factors such as de-conditioning due to being sedentary. From another perspective, although only 1 of every 40 community-dwelling seniors who falls will be hospitalized, of those hospitalized, only half will be alive a year later. [19] Even among longer-term survivors, many will be institutionalized. Tinetti asserted that 1 in 10 falls results in serious injury, including hip fracture, subdural hematoma and head injury. Falls account for 10% of visits to emergency departments and 6% of urgent hospitalizations among seniors, representing a significant economic burden to the health care delivery system. [21]
The most devastating result of a fall is fracture. Among younger seniors, wrist fractures are more common than hip fracture since they are more capable of bracing themselves by falling on an outstretched hand (FOOSH). [19] However, older adults (over the age of 75 years) are more likely to suffer a hip fracture, which often results in permanent disability, infirmity or death.
Risk Factors
Among seniors, the group most at-risk of falling are women who live alone (separated, divorced, widowed); who have a higher level of education but lower income; and are aged 80 years or older; the risk of falling increases with age. [18] Tinetti states that seniors who are depressed, arthritic, orthostatic, suffer from impaired vision, hearing, balance or gait or who have been prescribed more than four medications are at greatest risk of falling. [21]
There are two broad methods used to delineate risk factors of falling among seniors. One method divides risk factors into “internal” factors (essentially biological factors) and “external” factors (i.e., environmental factors). The other method used in the Canadian Senior’s Report, is to divide risk factors into three broad categories:1) medical/biological,
2) environmental and;
3) behavioral. [18]Medical or biological risk factors. These include visual impairment, problems with gait and balance, osteoporosis, orthostatic hypotension, muscle weakness (loss of strength, flexibility), cognitive impairment, peripheral neuropathies (especially loss of sensation in the feet associated with diabetes), cardiopulmonary disease (asthma, COPD), cardiovascular disease (especially transient ischemic attacks), upper motor neuron diseases (Parkinson’s disease, multiple sclerosis) and depression. [18, 22, 23] Depression is related to falls since depression may contribute to inattentiveness, risk-taking behavior, use of psychotropic drugs, and disuse atrophy or muscle weakness from being sedentary. Depressed patients may also have an increased fear of falling. [24] People with Parkinson’s disease often display a rather unique phenomenon called the “freezing of gait,” during which a person comes to an abrupt halt when walking, especially as they reach a doorframe. [25] Orthostatic hypotension may also contribute to falls. Orthostatic hypotension is often more pronounced in the morning, due to diminished baroreceptor responsiveness from prolonged recumbency or self-restriction of fluids due to issues of incontinence. [22]
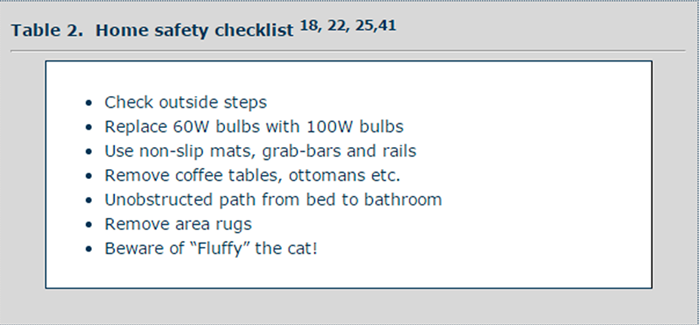
Table 2 Environmental risk factors. These encompass factors within and outside the home. Common environmental risk factors found in a person’s home include loose area rugs; ottomans; poorly maintained stairs; dark rooms (i.e. basements); lack of handrails by stairs, sinks, toilets or bathtubs; exposed electrical cords; and tripping over the family pet. [18, 22, 26] (See Table 2) Risk factors outside of the home include poorly maintained stairs or rails; poorly maintained sidewalks; uncleared walkways (especially during winter months); slippery surfaces in shopping malls or hospitals and improperly used walking assistive devices.
Behavioral risk factors. Behavioral risk factors associated with falling include “rushing” or “hurrying” (especially on stairs); previous history of falls; polypharmacy (which includes drug/drug, drug/ nutriceutical and drug/over-the-counter medication reactions); ill-advised or high-risk climbing or other activities (such as standing on chairs to reach items out-of-reach in kitchens); excessive alcohol use and improperly fitting footwear. [18, 22, 26]
Assessment of Fallers
If a patient presents to a practitioner’s office subsequent to a fall, the doctor should ask the SPLAT questions.22 The SPLAT questions are:S: Symptoms at the time of the fall (dizzy or lightheaded, for example).
P: Prior falls. This may provide the practitioner with invaluable information to identify chronic or recurrent risk factors.
L: Location of the fall. This may point toward an environmental in-home area of risk, typically the bathroom or kitchen.
A: Activities at time of fall. As discussed previously, a number of high risk activities are associated with falling.
T: Time of day. If falling occurs in the morning, it may be related to orthostatic hypotension. Falling toward the end of a day may be related to muscle fatigue and weakness.The patient interview and physical examination are essentially the same whether or not the person has fallen before; it is especially important to inquire about current medications. Many practitioners only ask about pharmaceuticals, but it is equally important to ascertain which nutriceuticals (vitamins, minerals, botanicals or homeopathic remedies) and over-the-counter (OTC) drugs a person is consuming. Products may interact and result in a vast array of clinical symptoms; particularly relevant to falls are dizziness and acute confusion among older patients. In fact, when it comes to senior patients, an argument can be made that any presenting sign or symptom should be considered a possible adverse drug reaction until proven otherwise.
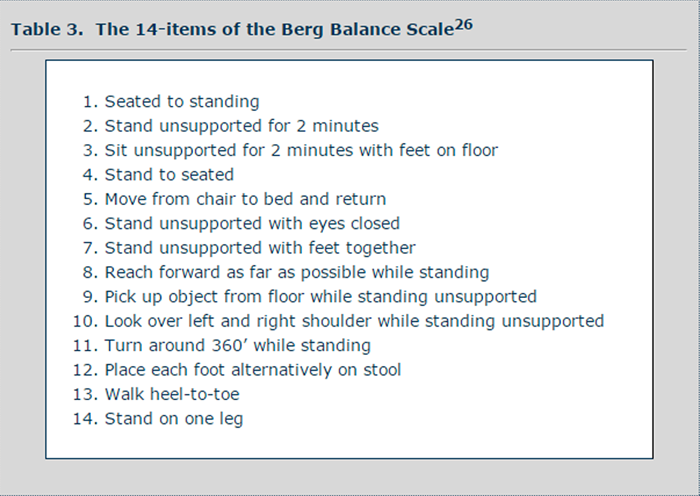
With respect to the physical examination, along with standard orthopedic and neurological testing, a practitioner can also use several simple, well-documented methods to evaluate balance. Foremost among these assessment methods are the Berg Balance Scale (BBS) [27] and the Get Up and Go Test (GUGT). [28]
Table 3
Table 4 The BBS is a 14-item test that can be performed in-office and requires no special equipment. Examples of tasks to be performed during the BBS are summarized in Table 3. Patients are scored on a scale from 0 to 4 on each task. The BBS has been shown to be a valid and reliable measure of balance; it is also used as an outcome measure in a number of investigative studies that seek to monitor a patient’s change in gait and balance post-intervention.
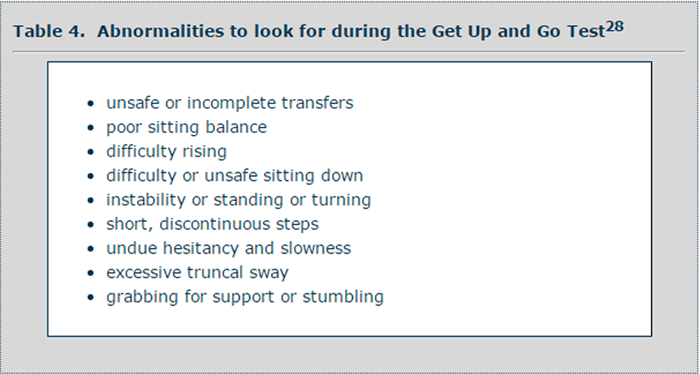
The GUGT is an even easier test to perform.28 It requires the patient to be seated in a chair with armrests, to lift him or herself into a standing position, walk 3 meters (10 feet), turn around and return to a seated position in the chair. A number of sub-skills are required to effectively perform this test and an examiner should be vigilant to observe all of them (see Table 4). This test can also be timed, and is then referred to as the “Timed Get Up and Go Test.” Similar to the BBS, this test can be used for either diagnostic purposes or as a post-intervention outcome measure of change in balance and gait.
Lastly, a prudent practitioner ought to assess a person’s global ranges of spinal motion, segmental joint function (using joint play, static or motion palpation) and the strength and length of muscles particularly important for gait and balance, such as the quadriceps, psoas and tibialis anterior (TA) muscles. The TA muscle is especially important to assess since weak dorsiflexors of the foot can cause a person to easily stumble on a relatively low environmental obstacle. [22]
Preventive Strategies
Falls often result in a downwardly spiraling decline in a person’s Activities of Daily Living (ambulation, bathing, feeding, transferring, toileting, dressing), increase in nursing home placement and loss of independence. Furthermore, some seniors greatly diminish their socialization and thus their quality of life due to heightened fear of falling. [21, 22] Bearing this in mind, the best treatment for falls is fall prevention.
The WHO Global Report of Falls Prevention in Older Adults [29] advocates a three-pronged approach:1) Awareness,
2) Assessment and
3) Intervention.It is the position of WHO that awareness-building is important since some cultures consider falls among seniors to be a natural consequence of aging, a myth that must be dispelled. Awareness-building also includes recruiting healthcare providers as well as both formal and informal caregivers in interventional initiatives, in addition to the role of government agencies and the media, who can fund, advocate and disseminate information and portray a positive image of seniors.
Assessment refers to identifying those seniors most at-risk of falling (those with advanced osteoporosis, on multiple medications, who have gait disturbances or are dizzy, for example) using the tools previously discussed. Implicit in this strategy is that assessment tools are not gender or age discriminatory, are readily accessible and are affordable. [29]
Lastly, interventional strategies that are evidence-based include home safety checklists (Table 3), medication monitoring, prescription of exercise for targeted muscles of concern, environmental changes, assessing a person’s readiness to change, providing seniors with incentives to change, providing regular and encouraging feedback, monitoring progress with respect to outcomes that are important to seniors and referring a person to the most appropriate health care provider, as circumstances dictate. [29]
For people to change, they must believe that making a healthful lifestyle change (strength training for example) is good for them, that it is something they can actually do and that they are provided sufficient guidance to achieve it. [30] For example, an older person may claim he cannot exercise because he does not have the time; if so, he can be encouraged to keep a diary of typical daily activities. A healthcare provider can then help identify times when exercise can be incorporated into the person’s life without disruption, such as performing simple muscle stretches and strengthening exercises with thera-bands while watching television. [30] Seniors should also be forewarned that minor injuries during exercise are commonplace and easily treatable, often through chiropractic care.
In order to inculcate fall prevention strategies into a person’s life, incentives can include reminding him or her of the devastating consequences of a fall and, with respect to exercise, visualization of improved body shape, lowering of blood pressure, enhanced endurance and flexibility, better glycemic control, improvements in sleep, better sexual function and the social benefits of group exercise. [7]
The Cochrane Collaboration has published two reviews on falls prevention, one in 2003 [31] and more recently in 2008. [32] In general, the authors of those reviews indicated that interventions must be population-based since it is important for the entire community to take an active role in fall prevention, [31, 32] a consistent finding since the early 1990s. [33] Specifically, strategies found to most likely result in significant reduction in falls among seniors include strength-training and balance-training programs (especially targeted towards muscles of the lower limb); home hazard assessments; withdrawal from psychotropic medication; Tai Chi; group exercise and nutritional supplementation. [31, 32]
Additionally, the best recent evidence consistently indicates that multi-dimensional approaches are more effective than implementing only one or two preventive strategies at a time. For example, a recent intervention involving healthy, mobile, community-dwelling seniors incorporated risk-abatement, cognitive behaviors and environmental changes simultaneously. [34] The percentage of seniors who fell over a four month period of time in the multi-pronged approach group was roughly half the percentage of seniors who fell in the control (no intervention) group (17% compared to 35%). An additional finding was that fewer adults in the treatment group who had fallen fell again. It also bears mentioning that, although hip protectors have previously been thought to diminish the likelihood of hip fracture among fallers, the 2010 Cochrane review indicates that they appear to have no effect on the rate of falls or fractures, and that long-term compliance with their use is, in any case, poor. [35]
With respect to exercise and dizziness, one small study by Hess et al reported that older patients under a high-intensity strength training program demonstrated improvement in their strength and diminished symptoms of dizziness as monitored by the BBS and GUGT. [36] This also manifested as a decrease in the number of falls among this group of subjects. Another study divided a group of 16 Alzheimer patients into two groups: Group 1 was entered into a 6 month exercise program and group 2 was not. [37] At the end of the trial, subjects in the exercise group did not suffer a progression of cognitive decline but they did demonstrate improvements in balance (as measured by the Mini-Mental State Exam and BBS and other balance scales respectively) as compared to the control group.
Chiropractic and Falls Prevention
Chiropractors have an important part to play with respect to fall prevention. Not only can practitioners champion many of the interventions recommended by the Cochrane Review and WHO initiatives (risk-abatement, home-safety checklists, physical activity) but some experts also suggest that chiropractic care, especially spinal manipulative therapy (SMT), might contribute to decreasing the risk of falls among seniors as well. [14, 23] Although there is at yet little evidence for such a contribution, there are a few studies which serve as examples of this important research direction.
Bracher et al38 chronicled the results of a small practice based clinical study involving 15 patients who were experiencing dizziness and who were treated with SMT. Of the 15 patients, 9 reported a complete remission of symptoms and an additional 3 more reported clinical improvement in their symptoms.
More recently, Hawk et al [39] reported the results of a clinical pilot study investigating the effects of chiropractic care on 34 older patients with dizziness, balance difficulties and back pain. Subjects were divided into three groups: The “limited schedule” group (n = 13) received SMT to the spine and peripheral joints (or low-force instrument-assisted treatment if SMT was contraindicated), soft tissue therapy and heat for 8 weeks; the “extended care” group (n = 15) received the same schedule of care but also received care for an additional 10 months once a month; and a control group of 6 patients were only given a brochure on lifestyle changes and given home exercises. Using the BBS and Pain Disability Index to measure outcomes, patients receiving SMT demonstrated greater improvement compared to the control group. No treatment-related adverse reactions were reported by participants. [39]
Larson and Bergmann recently hypothesized that it is important to identify and correct vertebral joint dysfunction, referred to within the chiropractic profession as vertebral subluxations, among seniors who fall since such joint dysfunctions, if unresolved, can result in muscle spasm around cervical joints, leading to “a decrease in large joint mechanoreceptor firing as well as increased nociceptor firing,” [24 p152]: resulting in an increased risk of falling.
Chiropractic as a whole can play an indirect role in fall prevention since a plethora of clinical trials, investigational studies and case reports, coupled with practitioner experience, has reported that manual therapies (soft tissue therapies, mobilizations and spinal adjusting) can effectively manage a number of clinical conditions, or some of the consequences of these conditions in terms of spinal pain and dysfunction, [15] that affect older patients and that are typically managed pharmaceutically. [40] Doing so might therefore contribute to indirectly decreasing the number of falls resulting from dizziness associated with poly-pharmacy, by enabling some patients to decrease their medication use. A recent narrative review of chiropractic geriatric literature [41] as well as a textbook chapter on spinal adjusting for older patients42 suggest that conditions with associated symptoms which might be ameliorated by manual procedures include asthma, back pain, depression; fibromyalgia, lumbar stenosis, multiple sclerosis, osteoarthritis, and pneumonia.
The chiropractic profession in Canada has taken a leadership role in the area of fall prevention among seniors by developing a falls prevention program targeted toward both older patients and chiropractors themselves. Called the Best Foot Forward: Don’t Let A Fall Get You Down,43 this fall prevention program was developed by this author in 2008 for the Canadian Chiropractic Association (CCA), the federal advocacy group. The Best Foot Forward Program was divided into two broad sections. The first section including epidemiological information, risk factors, a quiz a person could take to determine his or her risk of falling and a home safety checklist: This information was accessible by the public if they contacted the CCA by phone or internet. The second section included information to enhance a field practitioner’s clinical acumen by providing him or her with suggestions to enhance a patient’s interview and physical assessment subsequent to a fall. The information was formatted on DVD and mailed to all members of the CCA at no cost during 2008. The Program did garner positive media attention, with this author being interviewed on Canada AM in March 2008;44 the program was also noticed by the federal government and meetings were held with members of the Canadian parliament and PHAC.
Summary
This article has now come full circle. Initially it began with a plea for the chiropractic profession to champion the doctrines of health promotion and disease prevention developed by the World Health Organization. An argument was subsequently made for chiropractic to pursue this agenda by focusing on falls prevention. By doing so, the chiropractic profession can continue to make important contributions to one of the most important health initiatives of the 21th century.
Addendum: As this manuscript was being prepared for on-line publication, a systematic review for the United States Preventive Services Task Force (USPSTF) on the topic of falls prevention was retrieved. [45] Michael and her colleagues reported that 'primary care-relevant interventions' exist that can reduce falls among community-dwelling seniors (studies involving institutionalized or hospitalized patients were excluded). Specifically, subsequent to reviewing 61 articles germane to falls prevention, these researchers reported there was evidence that both exercise/physical activity and vitamin D supplementation reduces the risk of falls among seniors. They also determined that multifactorial interventions that assessed primary risk factors of falls (medication use, visual acuity, home environment, gait and balance) seemed to reduce falls, although pooled data were not statistically significant. It bears mentioning that the researchers also noted that the evidence suggested that serious clinical harms were no more common for older adults in intervention groups than for those in control groups.
References
Nelson, C., Lawrence, D., Triano, J., Bronfort, G., Perle, S., Metz, R. D., et al.
Chiropractic As Spine Care: A Model For The Profession
Chiropractic & Osteopathy 2005 (Jul 6); 13: 9Hawk C.
Should chiropractic be a ‘wellness’ profession?
Top Clin Chiropr 2000;7(1):23-26.Cooperstein R, Gleberzon BJ.
Towards a taxonomy of subluxation-equivalents.
Top Clin Chiropr 2000;8(1):49-60.World Health Organization:
Health Promotion Glossary (1998)Coulter, I.
Chiropractic: A Philosophy for Alternative Health Care.
Oxford, UK: Butterworth-Heinemann, 1999.Meeker, W., & Haldeman, S. (2002).
Chiropractic: A Profession at the Crossroads of Mainstream and Alternative Medicine
Annals of Internal Medicine 2002 (Feb 5); 136 (3): 216–227Gleberzon BJ, Gengenbach MS, Montgomery P.
Physical activity and the older person.
In: Hyde TE, Genegenbach MS, editors.
Conservative Management of Sports Injuries, 2nd Ed.
Sudbury, MA: Jones and Bartlett Publishers; 2007:953-969.Fries JF.
Aging, natural death and compression of morbidity.
N Engl J Med 1980;303:130-5.World Health Organization.
The Ottawa Charter for Health Promotion (1986)Bolton JE.
The evidence of evidence-based practice. What counts and what doesn’t count?
J Manipulative Physiol Ther 2001;24(5):362-6.Haynes B et al.
Clinical expertise in the era of evidence-based medicine and patient choice.
ACP Journal Club 2002;Mar-Apr:136-A11.Triano, JJ.
What Constitutes Evidence For Best Practice?
J Manipulative Physiol Ther. 2008 (Nov); 31 (9): 637–643Sackett DL.
Evidence-based medicine.
Spine 1999;23(10):1085-1086.Hawk C, Schneider M, Dougherty P, Gleberzon B, Killinger LZ.
Best Practices Recommendations for Chiropractic Care
for Older Adults: Results of a Consensus Process
J Manipulative Physiol Ther 2010 (Jul); 33 (6): 464-473Gleberzon BJ, Killinger LZ.
Management considerations for patients with osteoarthritis and osteoporosis:
A chiropractic perspective on what's working.
Top Clin Chiropr 2002 March;9(1):48-61.Cramer GD, Henderson CNR, Little JW et al.
Zygapophyseal Joint Adhesions After Induced Hypomobility
J Manipulative Physiol Ther. 2010 (Sep); 33 (7): 508–518Cramer G.D., Fournier J.T., Henderson C.N., Wolcott C.C.
Degenerative Changes Following Spinal Fixation in a Small Animal Model
J Manipulative Physiol Ther 2004 (Mar); 27 (3): 141–154Report on Senior’s falls in Canada.
Public Health Agency of CanadaRubinstein LZ.
Falls in older people: epidemiology, risk factors and strategies for prevention.
Age Ageing 2006;35-S2:37-41.Tibbits M.
Patients who fall: how to predict and prevent injuries.
Geriatrics 1996;51(9):24-31.Tinetti ME.
Preventing falls in elderly patients.
N Engl J Med 2003;348(1):42-49.Gleberzon BJ,
Instability, falls, fractures and disorders of gait and proprioception.
In: Chiropractic Care of the Older Patient. Gleberzon BJ (ed).
Butterworth-Heinemann (Elsevier). Oxford, UK. 2001:201-2121.Larson L, Bergmann TF.
Taking on the fall: the etiology and prevention of falls in the elderly.
Clin Chiropr 2008;11(3):148-154.Rubinstein LZ, Rubinstein KR.
Falls and their prevention in elderly people: What does the evidence show?
Med Clin in North Amer 2006;90(5):Bloem BR, Hausdorff JR, Visser JE et al.
Falls and freezing of gait in Parkinson’s disease: a review of two interconnected,
episodic phenomena.
Movement Disorders 2004;19(8):871-884.Public Health Agency of Canada.
The Safe Living Guide- a Guide to Home Safety for Seniors 2005Berg KO, Maki BE, Williams JJ et al.
Clinical and laboratory measures of postural balance in the elderly population.
Arch Phys Med Rehabil 1992;73:1073-1080.Messinger-Rapport BJ et al.
Prevention for the older women. Mobility: A practical guide to
managing osteoarthritis and falls.
Geriatrics 2003; 58(7):22-29.WHO Global Report on Falls Prevention in Older Age.
WHO 2007 Accessed Sept 11, 2008Gleberzon BJ, Gengenbach MS, Montgomery P.
Physical activity and the older patient.
In: Conservative Management of Sports Injuries. Hyde T (Ed).
Sudbury, MA: Jones and Bartlet Pub.Gillespie LD, Gillespie WJ, Robertson MC et al.
Interventions for preventing falls in elderly people (review).
Cochrane Database of Systematic Reviews 2003, Issue 4.McClure R, Turner C, Peel N et al.
Population-based interventions for the prevention of fall-related injuries
in older people (review).
The Cochrane Collaboration, 2008;Issue 3:2-3.Tinetti M, Baker DJ, McAvay C et al.
A multifactorial intervention to reduce the risk of falling among elderly people
living in the community.
N Engl J Med 1994;331:821-7.Edwards N, Gallagher E, Lockett D.
Steady As You Go (SAYGO): A falls-prevention program for seniors living in the community.
Can J Aging 2003;22(2):207-16.Gillespie WJ, Gillespie LD, Parker MJ.
Hip protectors for preventing hip fractures in older people (review).
Cochrane Database of Systematic Reviews 2010, Issue 10.Hess JA, Woollacott.
Effect of high-intensity strength-training on functional measures of balance
ability in balance-impaired older adults.
J Manipulative Physiol Ther 2005;28:582-590.Hernandez SSS, Coelho FGM et al.
Effects of physical activity on cognitive functions, balance and risk of falls
in elderly patients with Alzheimer’s disease.
Rev Bras Fisioter 2010;14(1):68-74.Bracher ES, Almeida CI, Almeida RR, Duprat AC, Bracher CB.
A Combined Approach for the Treatment of Cervical Vertigo
J Manipulative Physiol Ther. 2000 (Feb); 23 (2): 96–100Hawk C, Cambron JA, Pfefer MT.
Pilot Study of the Effect of a Limited and Extended Course of Chiropractic Care
on Balance, Chronic Pain, and Dizziness in Older Adults
J Manipulative Physiol Ther. 2009 (Jul); 32(6): 438–447McHenry MC.
Complementary and alternative medicine practices to alleviate pain in the elderly.
The Consultant Pharmacist 2010;25(5):284-290.Gleberzon BJ.
A narrative review of the published literature regarding older patients from 2001-2010.
J Can Chiropr Assoc 2011 (Jun); 55 (2): 76-95.Gleberzon BJ, Byfield D, Barber M.
Spinal adjusting for older patients.
In: Technique Skills in Chiropractic. Byfield D (ed).
Oxford, UK: Elsevier.Best Foot Forward: Don’t Let a Fall Get You Down
http://esi.ctv.ca/datafeed/urlgen2.aspx?vid=38837
Michael YL, Whitlock EP, Lin JS et al.
Primary-care relevant interventions to prevent falling in older adults:
A systematic evidence review for the U.S. Preventive Services Task Force.
Ann Intern Med 2010;153:815-825
Return to SENIOR CARE
Return to VERTIGO and BALANCE Page
Since 4-20-2016

| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |