

Exploring Chiropractic Services in the Canadian Forces Health Services -
Perceptions of Facilitators and Barriers Among Key InformantsThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Military Medicine 2019 (May 1); 184 (5-6): e344–e351 ~ FULL TEXT
Silvano A. Mior, Ellen Voge, Deborah Sutton, Simon French, Pierre Côté, Margareta Nordin, Patrick Loisel, Audrey Laporte
Department of Research and Innovation,
Canadian Memorial Chiropractic College,
6100 Leslie Street, Toronto,
Ontario, Canada.
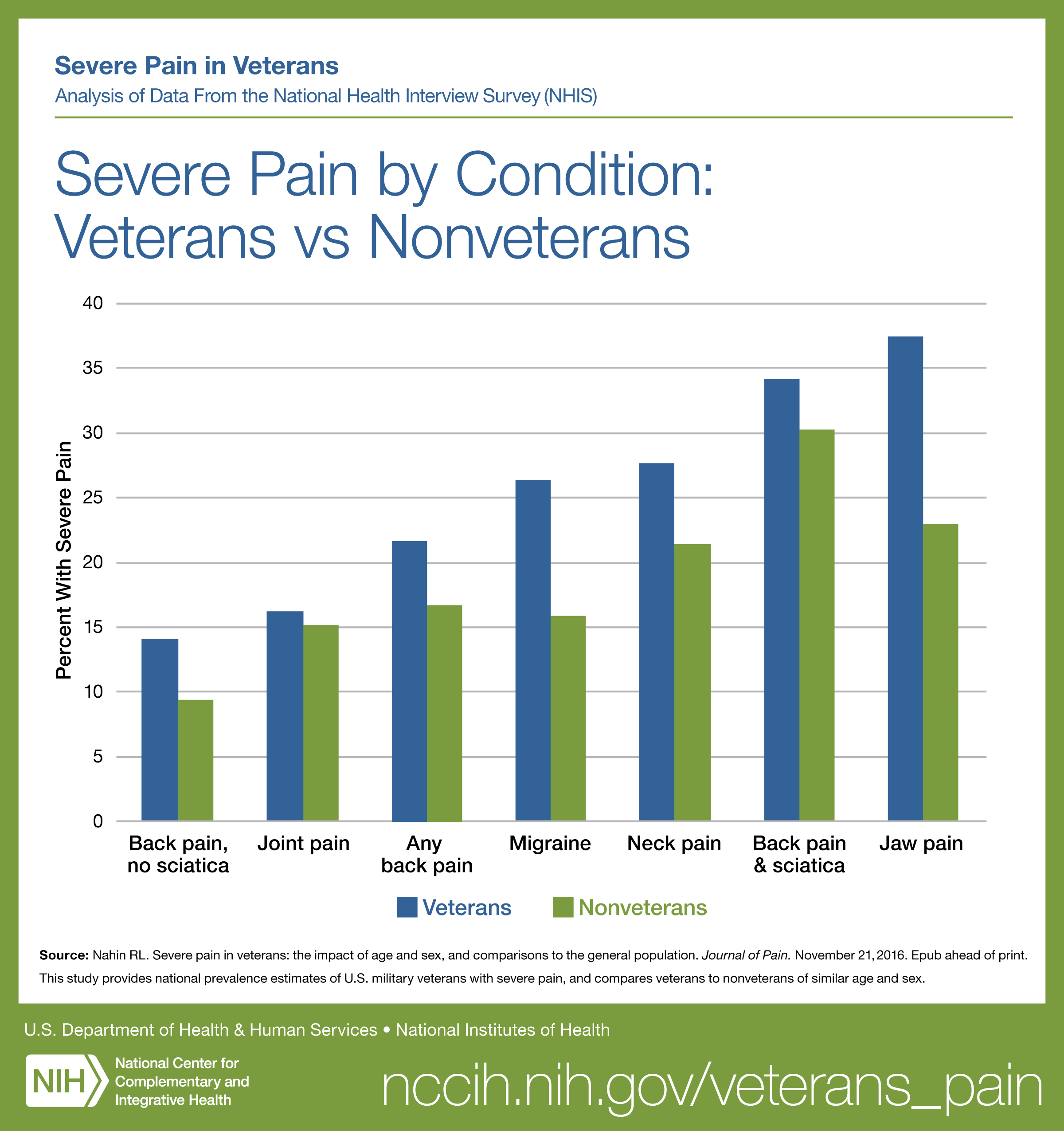
FROM: Nahin ~ Pain 2017INTRODUCTION: Musculoskeletal (MSK) conditions have a significant impact on the health and operational readiness of military members. The Canadian Forces Health Services (CFHS) provides a spectrum of health services in managing Canadian Armed Forces (CAF) personnel health care needs with on-base and off-base services provided by civilian and uniformed health care professionals, including chiropractors. Although chiropractic services are available in US DoD and VA systems, little is known about the facilitators and barriers to integrating on-base chiropractic services within the CFHS. This study explored key informants' perceptions of facilitators and barriers to the integration of on-base chiropractic services within the CFHS.
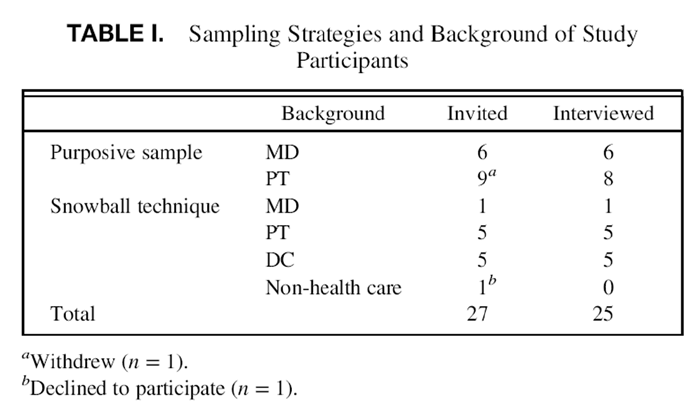
METHODS: We conducted a qualitative study to describe and understand how an integrated chiropractic service could be designed, implemented, and evaluated within the current interdisciplinary CFHS. Telephone interviews were conducted, using a semi-structured interview guide, to explore key informants' perceptions and experiences of chiropractic care within the CFHS. In total, we invited 27 individuals across Canada to participate; 15 were identified through purposeful sampling, 12 through a snowball sampling technique, and 2 declined. The 25 participants included military personnel (52%), public servants and contractors employed by the Department of Defense (24%), as well as civilian health care providers (24%). All participants were health care providers [physicians (MD) (7), physiotherapists (PT) (13), chiropractors (DC) (5)]. Interviews were audio-recorded and transcribed verbatim. Transcripts were prepared and analyzed using an interpretivist approach that explored key informants' perceptions and experiences.
RESULTS: Qualitative analysis revealed numerous facilitators and barriers to chiropractic services in the CFHS. These were categorized under three broad themes: base-to-base variations, variable gatekeeper roles, and referral processes. Barriers to integrating chiropractic services included: lack of clarity about a chiropractor's clinical knowledge and skills; CFHS team members' negative prior experiences with chiropractors (e.g., inappropriate patient-focused communication, clinical management that was not evidence-based, ignorance of military culture); suboptimal bi-directional communication between CAF personnel and DCs across bases; and wide-ranging perspectives pertaining to duplication of services offered by PTs and DCs in managing MSK conditions. Facilitators associated with the integration of chiropractic services within a collaborative and interdisciplinary CAF environment included: patient benefits associated with multiple approaches utilized by different providers; adoption of up-to-date, high-quality evidence and guidelines to standardize care and curtail "dependency" between patient and providers; and co-location of providers to strengthen existing interprofessional communication and relationships. Key informants called for patient care that is collaborative, integrated and patient-centered, rather than "patient-driven" care; civilian providers understanding and respecting military culture rather than assuming transferability of patient management processes from the public civilian sector; standardization of communication protocols and measures to evaluate outcomes of care; and the need to move slowly and respectfully within the current CAF health care system if planning the on-base implementation of chiropractic services.
There is more like this at our
CHIROPRACTIC CARE FOR VETERANS PageCONCLUSIONS: This study illuminated many opportunities and barriers, in complex and diverse domains, related to introducing collaborative chiropractic services in the Canadian Forces Health Services (CFHS) . The findings are relevant to increasing understanding and strengthening interprofessional collaborative care within the unique Canadian Armed Forces (CAF) health care delivery system.
KEYWORDS: Chiropractic; Health Services; Military Medicine; Military Personnel; Rehabilitation Services
From the FULL TEXT Article:
INTRODUCTION
Musculoskeletal (MSK) conditions have a significant impact on the health and operational readiness of Canadian Armed Forces (CAF) personnel. [1] MSK conditions are the most common reason for CAF personnel not being deployed. [2] Further, MSK injuries are responsible for 42% of all medical releases. [3] Specifically, back pain is one of the most common reasons for soldiers not being deployed and is the second most common activity-limiting acute injury. [2, 4] In 2013, 12% of CAF regular force medical releases were attributed to lumbar injuries. [3] When symptoms persist, chronic back pain may impact many aspects of a CAF service member’s life, including: physical deconditioning; excessive use of prescription drugs; marked dependence on health care providers, spouse and family; withdrawal from social context; and continued functional impairment. [5] The effective and costeffective management of back pain is an important issue for individual members and the CAF as a whole. [6]
“Caring for Canada’s Ill and Injured Military Personnel,” a report of the Standing Committee on National Defense (2014) heard evidence about chiropractic services offered to US Military Health System (MHS) personnel and its impact on keeping soldiers at work. [7] The US MHS under the Department of Defense (DoD) included chiropractic services for active duty military personnel following the completion of an initial demonstration project in 1995. [8, 9] Currently, chiropractors provide conservative care, in cooperation with various health care providers, in primary care, physical therapy, orthopedics and sports medicine. [10] Chiropractic care is provided on referral and within a set of privileges established within each system and facility. [8] Two studies suggest significant improvements in pain, function, global improvement and satisfaction with care in samples of active duty military personnel receiving chiropractic care and standard medical care as compared to those receiving standard medical care alone. [11, 12]
Currently, the Canadian Forces Health Services (CFHS) provides a spectrum of health care services, including care provided in civilian facilities when services are not provided on-base.6 Chiropractic care is an eligible CAF health practitioner benefit when prescribed by a physician, and is accessed off-base, outside the military health system. Care is authorized within a 10-visit limit per condition, after which a physician’s review is required to determine if further care is necessary (http://ww.forces.gc.ca/en/caf-community-healthservices- benefits-drug-coverage/comprehensive-medical-care. page).
Historically in the CFHS, on-site chiropractic care was available during a 6-month pilot study at a CAF Base hospital, where two chiropractors provided outpatient chiropractic care with physicians’ referrals for treatment of MSK disorders. [13] Care was available in 10-visit increments and supported with appropriate clinical documentation. Physicians referred CAF military personnel to chiropractic services for axial, MSK complaints; if the complaint was unresponsive to, or the waiting list too long, for physiotherapy; a prior positive response to chiropractic care; or if the patient requested chiropractic care. [13] Patients reported high levels of satisfaction with their chiropractic care, as well as with office accessibility, clinic hours and the chiropractor’s ability to answer questions; none reported dissatisfaction with their chiropractic care. [13] Although specific outcomes were not reported, one-third of patients indicated that they expected better results or rate of improvement. [13] Referring physicians perceived an increased demand from patients for chiropractic services and they were satisfied with the chiropractic services provided. [13]
The Standing Committee on National Defense in Canada recommended that a comprehensive MSK strategy be developed to better understand injury causes, encourage early treatment and reduce barriers for current soldiers to obtain the required care. [7] Although chiropractic services are integrated into the US DoD system, barriers to integration exist, particularly if such services are thrust upon them. [14] Dunn et al identified barriers to the integration of chiropractic care in the US MHS, including: work place isolation; lost opportunities to influence communication; policy and practice without a chiropractor in a leadership role; precarious employment and decreased integration of chiropractors within the system resulting from contractor-status, or employee of a contractor; supervision by non-chiropractors; and refusal of referral by a gatekeeper. Facilitators to integration included documentation requirements in an electronic health record to aid collaboration between providers and opportunities for clinical education.
In addition to the Standing Committee’s recommendation of a comprehensive management strategy for MSK, the federal government’s response suggested “examining whether earlier interventions by alternative health care professionals to treat MSK injuries are a workable and worthwhile approach.” [15] However, we know little about the facilitators and barriers to integrating on-base alternative health care professionals, such as chiropractors within the CFHS.
Purpose
We employed a qualitative, exploratory research design to understand and describe key informants’ perspectives on how an integrated chiropractic service could be designed, implemented, and evaluated within the current interdisciplinary CFHS.
METHODS
Approvals and Recruitment
Ethics approval was received from the Research Ethics Boards at the University of Ontario Institute of Technology (# 15-049) and the Canadian Memorial Chiropractic College (# 152019). Agreement to conduct the study was provided by the Canadian Deputy Surgeon General, CFHS (7 June 2016). All study participants provided informed consent.
Purposeful sampling16 was used to recruit participants. Inclusion criteria included: English-speaking health care professionals, military personnel, and researchers with extensive experience and in-depth understanding of health care delivery and interprofessional collaborative practice within the military setting in Canada. Additional participants with expert knowledge and/or experience in relation to the delivery of health care within the CFHS were identified using snowball sampling technique. [16]
Interview Schedule and Procedures
Telephone interviews were conducted using an interview guide with open-ended questions. [17–20] The interview guide was informed by expert opinion, as well as health, social and behavioral theories addressing barriers and facilitators to accessing chiropractic care (See Appendix A). After the first eight interviews, additional probes were developed and questions slightly revised. Interviewing continued until the research team ascertained that saturation of responses to key questions was achieved. [21, 22]
All interviews were conducted by two members of the research team, both health care professionals, who were not physicians, chiropractors nor physiotherapists, thereby mitigating potential researcher bias. [20] The interviews were conducted between September 2016 and February 2017 and were 45-to 60-minutes in duration.
Interviews were audio-recorded, exported to an encrypted USB key and transcribed verbatim. The project coordinator reviewed all transcripts for accuracy against the recorded sessions. Content errors were corrected, and names along with other potential identifying information removed from transcripts prior to coding. Each participant was invited to review and edit their transcript (member checking).
Analytic Approach
Transcripts were analyzed using an interpretivist approach that explored participants’ experiences and thoughts. [23, 24] Each transcript was examined using qualitative content analysis. [25, 26] Categories and subcategories were collapsed and interconnected to develop meaning and explanation of the patterns identified in the data.
The analysis proceeded in an iterative and inductive manner. After the first three interviews were completed and transcribed, the transcripts were sent to three research team members who independently coded each transcript. The researchers then met regularly to review and reach consensus on coding, examining and defining codes, and developing a referent codebook. The coding structure and the related transcript reference data were entered into qualitative data analysis software (NVivo Pro Version 11.4.1 for Windows, QSR International (Americas) Inc., Burlington, MA, USA).
RESULTS
Participant Characteristics

Table 1
Table 2
Table 3 Table I provides information on study participants’ professional backgrounds. Participants included military personnel (52%), public servants and contractors employed by the Canadian DoD (24%), and civilians (24%), distributed across Canada. Military participants included ranks of Chief Warrant Officer, Captain, Lieutenant, Lieutenant Colonel, and Colonel. Slightly more than half of the military participants were deployed at least once over the course of their career. Participants self-identified as medical doctors (MD), physical therapists (PT), and chiropractors (DC). The chiropractor participants, all situated off-base, had recently provided care for CAF service members. Of the 25 study participants, the majority were male (n = 76%).
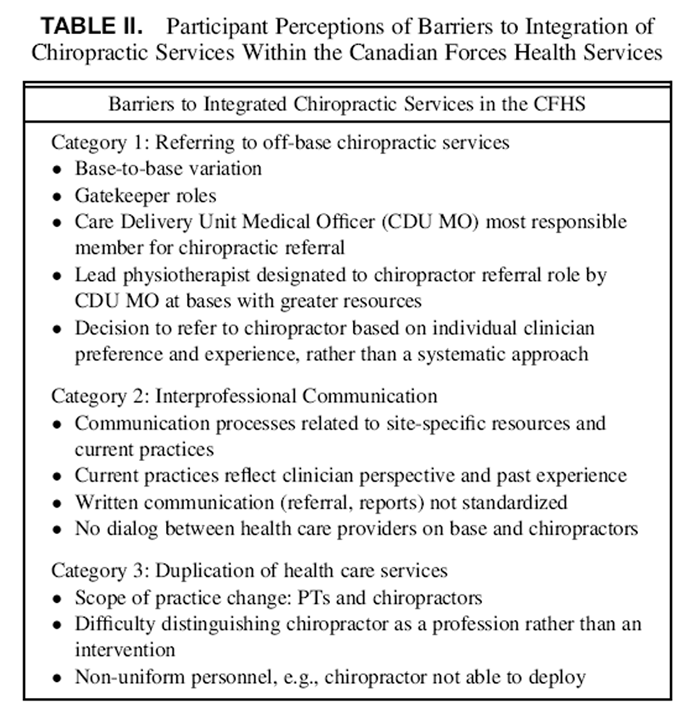
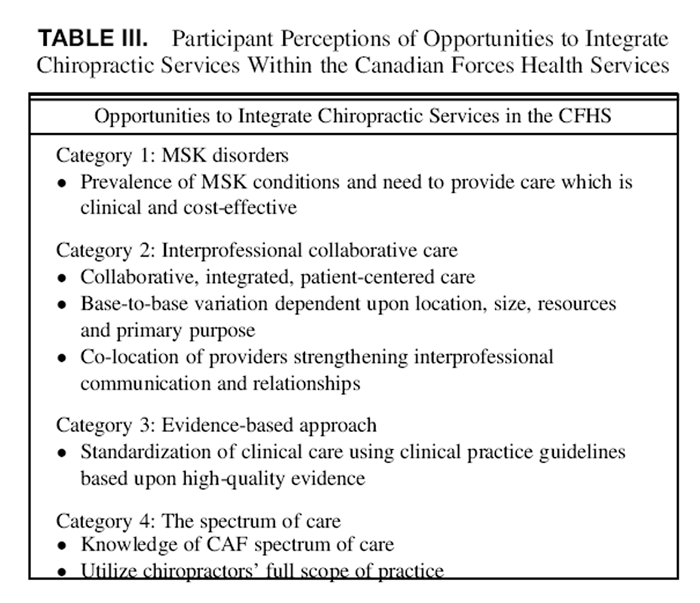
Participants identified barriers (Table II) and opportunities (Table III), with categories described within each, that could potentially serve to integrate chiropractic services within the CFHS.
Barriers to Integrated Chiropractic Services in the CFHSDuring the interviews, participants identified a range of factors and issues that could potentially act as barriers to the design, implementation and evaluation of chiropractic services within the CFHS.
Referring to Off-base Chiropractic Services:
“Referring to person, not profession.”
One emergent barrier to integration was the significant base-to-base variation with respect to referrals to chiropractic services.
Additionally, notable differences were illuminated with respect to the critical “gatekeeper” role in the Care Delivery Unit (CDU) of CAF bases.
Within the CFHS, the function of the CDU is comparable across all CAF bases; however, they differ in structure and administrative processes. Such regional variation is consistent with findings in the Auditor General of Canada report. [27] Participants noted that the triage of MSK conditions in sick parade (military medical triage system that occurs every morning for patients with acute ailments) varies between bases, but fundamentally is the responsibility of the CDU Medical Officer, who acts as the “gatekeeper” for referrals both on- and off-base. Participants’ recognized the role of medical physicians in overseeing the primary care of CAF personnel, but noted physicians’ limitations when assessing MSK injuries. Consequently, at adequately resourced bases, the “lead” physiotherapist or designate would triage MSK conditions at sick parade, overseeing the referral process when deemed necessary. A MD participant explained that within the CFHS, there is no “direct access” to a chiropractor.
Participants on larger and better-resourced bases, indicated that Medical Officers may direct uniformed physiotherapists to make decisions regarding the need for, or appropriateness of, referrals off-base.The current way that it works…is that a Medical Officer can make the recommendation to the physiotherapy department, but it is ultimately the physiotherapy department that makes the “yes” or “no” call.
(PT, K15)
So, from my experience here and at the many previous postings that I have had, we haven’t really seen a significant need for chiropractic referral to an external health care provider for the simple reason that we [physiotherapists] are able to provide every skill set and every possible intervention that a CAF member may require as part of their treatment plan… The odd case when a spinal manipulation is indicated for a particular condition such as a fixated facet joint, something of that nature, where they have a mechanical obstruction that a low amplitude high velocity mobilization may be beneficial for, we have the flexibility to refer to a chiropractor as they specialize in this technique.
(PT, K3)As a consequence of base-to-base variations in referral processes, and variable enactments of the “gatekeeper” role, the frequency and nature of referrals vary. Specifically, the decision to refer to chiropractors appears to be up to individual clinicians rather than based on a systematic approach.
Inter-professional Communication:
“Never enough information”
Another barrier focused on interprofessional communication, primarily between on-base physiotherapists and off-base service providers. Variations in communication processes were related to available site-specific resources and current practices. Current practices were influenced by past experiences and perspectives of the lead CFHS provider(s). In general, communication, particularly with respect to off-base referrals, was considered suboptimal. However, some on-base CFHS providers stated that they made an effort to share relevant clinical information with off-base providers. In these situations, a referral note may be followed by a phone call to the off-base provider. However, standardization of communication processes in the CFHS was not typical practice:There has been no effort to try and standardize care across the country, I think at every base there will be different interactions between the base and the chiropractors…
(PT, K13)
So, it is really a one-way communication. We [off-base chiropractor] get the referral and then I submit an initial assessment and a progress exam and we don’t really get a lot of feedback from the military. So, everything is written, it is by correspondence. There is really no face-to-face time, or conversations on the phone. It is all done through email or written reports that we send by mail.
(DC, K24)Similarly, the reports received by on-base CFHS health care providers from off-base chiropractors, often fell short of expectations. Participants noted that chiropractors’ reports often did not include important patient outcomes that are considered necessary to assess the effectiveness of the care delivered.
The biggest problem in the [off-base healthcare providers’] reports was they said nothing. They would often say, “Member has benefitted from treatment, recommend more treatment.” It wouldn’t say, “How has he benefitted. Is it based on his Oswestry scores? Is it based on him telling you he feels better? Is it based on he can now lift 50 lbs. versus before he could only lift 20?” I didn’t know, so there was never enough information and often when I would ask for information, I wouldn’t receive it.
(PT, K6)Currently, off-base providers cannot access health information available in service members’ CFHS electronic health records. Therefore, off-base health care providers are dependent upon information provided within the referral process and discharge notes. Participants agreed that addressing the gaps in bi-directional communication would improve quality of care and strengthen interprofessional relations.
Duplication of Healthcare Services:
“Blurring scopes of practice”
The third category addressed perceptions and experiences related to the duplication of health care services involving physiotherapists and chiropractors. Participants concurred that over the past decade, the changing scope of practice for both physiotherapists and chiropractors has significantly blurred their unique roles. This blurring of roles creates confusion among patients and health care providers, and a lack of clarity of the unique role each provider can play.Over the years, back when I first started being a physio, there seemed to be a very clear delineation between physio and chiropractic. But as the years have progressed, what we have seen is really a conversion of the two practices, where physios are taught a lot of manipulative therapy in school now and we continue that with post grad studies. And chiropractors tend to do a lot more non-manipulative type of treatment, whether it be active release therapy or acupuncture or more exercise based therapy. So, the difference that we used to see between the two professionals is now a lot more blurred, and there is a lot more shades of grey than this clear delineation between the two.
(PT, K25)Consequently, participants highlighted perceptions of duplication and/or redundancy of services as a major barrier to the integration of chiropractic services. Similar sentiment was expressed by a minority of North American orthopedic surgeons, suggesting manipulative care can be provided by physiotherapists and athletic therapists.28 If chiropractors and physiotherapists provided similar interventions, and physiotherapists were already accessible within the CFHS, sentiment was expressed that there was currently no need to provide access to chiropractors, regardless of their inclusion in the CFHS spectrum of care.
So, questions that may need to be answered is what type of conditions would be referred to a chiropractor versus a physiotherapist and look at the issue of redundancy of treatment… are there actually any additional skill sets which are not currently available within our practice.
(PT, K3)
Let’s just be clear on what it is they [chiropractors] are going to be doing because otherwise there is that perception of redundancy. The physios are telling me, “Well, why not just train more physios in manual therapy,” because those are expensive courses and because we expect our physios to be deployable and go to wherever the country asks them to go which wouldn’t be the case for the chiropractors that we employ.
(MD, K11)The preceding quote from a physician illuminates another potential barrier associated with deployment. Concerns related to deployment were raised by participants along with notions of encouraging patient dependency (i.e., perceived reliance on the health care provider and ongoing care). This barrier was particularly pertinent when considering that some contracted services, including chiropractic care, would not be available during military exercises and deployment.
Opportunities to Integrate Chiropractic Services in the CFHS
Musculoskeletal Disorders: “It’s a significant issue for us” The first category of opportunities underscored the significance of MSK conditions currently within the CAF.It is a big interest at the national level right now to explore the prevalence and the possible reasons why a proportion of the patients are referred back. There is great potential, now more than ever, to look at the present system of care for low back pain and make real, cost effective, and concrete changes to how we deliver this care.
(PT, K18)The perspectives shared by participants support the reported high prevalence of MSK conditions in the CAF. Participants noted the significance to service members and how MSK conditions negatively affect the health and wellbeing of active duty service members, in addition to being a prevalent source of CAF medical releases. These concerns are consistent with the CAF report that 43% of regular force medical releases were attributed to MSK conditions.4
Inter-professional Collaborative Care:
“See the patient from different perspectives”
The second category provided insights into opportunities to integrating chiropractic services on-base. The notion of interprofessional collaborative care was considered important by the majority of participants. Participants thoughtfully reflected that collaborative care delivered in a team-based approach provided an opportunity for multiple providers to contribute to patient care through their unique professional “lens.” Hence, viewed from this perspective, different professions could be considered not only for the interventions they provide but also by their approach to clinical care.29So, the beauty of collaborative care is that you can hopefully see the patient from various different perspectives… a more complete picture, than if just one person sees them, through the lens of what they tend to do.
(MD, K11)Participants shared their perspectives and experiences with various aspects of care delivery, particularly when involving chiropractors. The richness of the data and diverse experiences of the participants provided divergent perspectives of strategies used to manage back pain. This partly reflects baseto- base variations, including location, size, resources and primary purpose. This is highlighted as follows:
Now in [base] I used them [chiropractors] a lot because we didn’t have a lot of resources. We didn’t have a lot of physiotherapists, a lot of experienced physiotherapists. I found the chiropractic very similar to what I do, very active, not modality based. So, I trusted them, I trusted their clinical judgment, and so I used them for that and I used them for manipulation. So, I think it depends on the base and the resources available at the base, if that helps”.
(PT, K22)Although considered a challenge, such variation also provides opportunities to implement chiropractic services and compare health care programs on a national level. For example, a recent U.S. study reported significant improvements in pain, function, and satisfaction with care in the group of active duty military receiving chiropractic care and standard medical care compared to standard medical care alone.11,12
Evidence-based Approach:
“Very important”
The third category of opportunities underscored participants’ emphasis on service providers using an evidencebased approach in determining which interventions should be included within a program of care. Without exception, participants advocated for the use of evidence-based interventions, including use of evidenced-based clinical practice guidelines. A participant stated:“Obviously, evidence-based medicine is very important and there is a whole host of different I suppose guidelines as such in regards to how you approach back pain…”
(MD, K14)However, some participants could not differentiate between evidence for an intervention (e.g., manipulation) and the profession delivering the intervention.
I would say there is a specific need for evidence-based management of musculoskeletal conditions… Because that is what the Surgeon General expects…. there is nothing that chiro offers that is both unique and evidence-based, so for me it is about providing access to evidence-based care for MSK issues.
(PT, K6)
The Spectrum of Care:
“Chiropractic care, we think primarily spine”
The fourth category addressed participants’ knowledge and experiences pertaining to the “spectrum of care” in the CAF and the tendency to equate chiropractic care with spine care. There was consistency among most participants that access to services within the spectrum of care is for a specific intervention, rather than for the profession’s full scope of practice. Similar to other studies, consideration for referral for chiropractic services was made primarily for spinal manipulation to treat a spinal disorder, most commonly chronic low back pain.So, I think what we recognize chiropractors for the most are their skill sets in spinal manipulation.
(PT, K13)Participants’ perspectives of conditions managed by chiropractors are similar to that provided in a pilot study conducted with on-base chiropractors. In this study, almost 97% of military personnel were referred for spine-related conditions, of which almost 52% involved the low back.8 A minority of participants, particularly physicians who had established both personal and professional relationships with a chiropractor, considered also accessing chiropractors for their expert clinical opinion.
“Who ultimately is the spine care specialist?”, because we lump all kinds of people in that domain. I think given the nature of the specialty, and how much time chiropractors spend on the spine, I would have to agree that…chiropractors,…come closest to a spine care specialist.
(MD, K11)
I think that in general when we think of chiropractic care, we think of primarily spine, spinal, trunk and sort of mid thoracic trunk problems, and we tend to think less of them for extremity types of MSK complaints.
(MD, K12)The majority of participants called for a delivery approach involving chiropractors within an integrated team and founded on a patient-centered spine care model. In this model, providers are respected and distinguished for their uniqueness but the care is provided together with others and not in isolation. Hence, providers do not become the intervention, but rather health care professionals providing assessment and treatment, while respecting their scopes of practices and expertise.
DISCUSSION
Currently, CAF members have access to chiropractic services within the spectrum of care and at the discretion of the referring CFHS providers. Within this context, our study results inform processes that could address existing challenges to effective referrals and improve quality of care. CFHS team members’ lack of clarity about a chiropractor’s clinical skills and knowledge was a major challenge emerging from our data. Thus, one recommendation emanating from key informants’ comments would be establishing personal relationships (i.e., one-on-one professional contacts with chiropractors), rather than adopting a broader profession-based approach, with the goal of enhancing understandings regarding the knowledge-base and skill set of chiropractors.
This call for a more personal or idiosyncratic approach, as opposed to relying solely on objective data, was often used to inform referral practices. In this study, key informants’ experiences influenced opinions about the value and role of the chiropractor in managing specific MSK conditions. The reliance on personal relationships for referral is consistent with previous research suggesting that despite positive views of chiropractor’s providing helpful care for MSK conditions, the diversity within the profession limits referrals and creates barriers to interprofessional collaboration.28
In our study, the majority of participants appeared to view chiropractors more as a therapy, specifically manipulation, rather than as a profession providing comprehensive management and multiple treatment approaches. This perspective potentially limited access and timeliness of referrals for care. A minority of participants, based on personal experience, did appreciate the chiropractor’s assessment and therapeutic skills. These differing views of the role of the chiropractor in health care are consistent with a report by Herman and Coulter29, highlighting how health policies that define complementary and alternative professions as individual therapies rather than as a profession with a wider scope of practice, impacts patient access and care. A second recommendation emerging from this study is to explicate the role and responsibilities of the chiropractor in a collaborative CFHS environment based upon their professional scope of practice.
Our findings also suggest that the bi-directional communication between CFHS health care providers and chiropractors varies between bases but in general is considered “suboptimal.” Rather than a standardized format for written and verbal reports, report formats appeared to be individually developed and base-specific. Negative experiences (e.g., inappropriate communication, nonevidenced based clinical management, ignorance of military culture) may create professional tensions and biases that are then generalized beyond one-on-one encounters. Such experiences have been reported in other studies examining the integration of chiropractors within the US military30 and Canadian primary care.31 A third recommendation is to standardize and enhance the level of interprofessional communication to further continuity of patient care and improve quality care. In addition, educating non-military personnel about the uniqueness of the military culture would encourage the development and implementation of appropriate treatment plans.
Another barrier to integration of chiropractic services is the perceived certainty of duplication of services, based upon the “blurring of scopes of practice” between PTs and chiropractors. Perceived duplication and redundant services were previously reported as barriers for inclusion of chiropractors in health care teams (e.g., in sports medicine32,33). Others attribute such barriers to social constructs related to professionalization34 and the marginalization of professions,35 which impact boundary disputes and negatively influence collaboration. Fostering collaborative relationships between chiropractors and CFHS health care providers, within a patient-centered model of care, will assist in addressing these barriers.
Limitations
Our study sample consisted of military personnel, public servants and contractors of the Canadian Department of National Defense and civilians. Participants were from different CAF bases, health care services, and geographic regions across Canada. Military personnel were of different ranks and military experience. Nonetheless, individuals who were not invited to participate may have expressed different views. We also did not explore patients’ perspectives of care delivered within the CFHS nor their experiences when requesting or being referred for chiropractic services. Such experiences can significantly impact the inclusion of a health profession within a health care team.33
CONCLUSIONS
This study provided the first qualitative analysis of barriers and opportunities related to the integration of chiropractic services within the current CFHS environment. Our findings and recommendations provide an opportunity to address the current challenges identified by key informants for the participation or integration of chiropractors within the unique health care delivery system of the Canadian Armed Forces (CAF). Further, the findings provide important information to inform the potential design of an implementation study to assess the feasibility of integrating chiropractic services in the Canadian Forces Health Services (CFHS), while strengthening referral processes to chiropractors within the spectrum of care.
ACKNOWLEDGMENTS
We thank the men and women of the Canadian Forces Health Services for their contributions to this paper.
FUNDING
This study was funded by a grant from the Canadian Chiropractic Association and the Ontario Chiropractic Association. The funders did not have a role in study design, analysis, or preparation of this paper.
References:
Rowe P, Hébert LJ:
The impact of musculoskeletal conditions on the Canadian Forces.
In: Shaping the Future: Military and Veteran Health Research, pp 377–391.
Edited by Aiken A, Bélanger S Kingston, Canadian Defense Academy Press, 2011.Born J, Hawes R, Whitehead J:
Results from Health and Lifestyle Information Survey of Canadian Forces personnel 2008/2009:
Regular Force Version: Your Health Speaks Volumes.
Ottawa, Government of Canada, 2010.Canadian Forces Health Services Group:
Surgeon General’s Report 2014: Consolidation, Innovation, Readiness.
Ottawa, Government of Canada, Department of National Defence, 2014.Directorate of Force Health Protection:
Canadian Forces Health and Lifestyle Information Survey – 2008/2009.
Ottawa, Department of National Defence, 2010.Manchikanti L, Singh V, Datta S, Cohen SP, Hirsch JA:
Comprehensive review of epidemiology, scope, and impact of spinal pain.
Pain Physician 2009; 12(4): E35–70.Canada, Department of National Defence.
Caring for Our Own: A comprehensive approach for the care of CF ill and injured members and their families.
Ottawa, 2012.Canada Parliament House of Commons:
Caring for Canada’s Ill and Injured Military Personnel (June 2014) 41st Parliament, 2nd Session, pp 1–93.
Edited by Standing Committee on National Defence Ottawa, Government of Canada, 2014.Green BN, Johnson CD, Daniels CJ, Napuli JG, Gliedt JA, Paris DJ.
Integration of Chiropractic Services in Military and Veteran Health Care Facilities:
A Systematic Review of the Literature
J Evid Based Complementary Altern Med. 2016 (Apr); 21 (2): 115–130Dunn AS, Green BN, Gilford S.
An Analysis of the Integration of Chiropractic Services Within
the United States Military and Veterans' Health Care Systems
J Manipulative Physiol Ther. 2009 (Nov); 32 (9): 749–757Green BN, Johnson CD, Lisi AJ.
Chiropractic in U.S. Military and Veterans’ Health Care
Military Medicine 2009 (Jun); 174 (6): vi–viiGoertz CM, Long CR, Hondras MA, Petri R, Delgado R, Lawrence DJ, et al.
Adding Chiropractic Manipulative Therapy to Standard Medical Care
for Patients with Acute Low Back Pain: Results of a Pragmatic
Randomized Comparative Effectiveness Study
Spine (Phila Pa 1976). 2013 (Apr 15); 38 (8): 627–634Goertz CM, Long CR, Vining RD, Pohlman KA, Walter J, Coulter I.
Effect of Usual Medical Care Plus Chiropractic Care vs Usual Medical Care
Alone on Pain and Disability Among US Service Members With
Low Back Pain. A Comparative Effectiveness Clinical Trial
JAMA Network Open. 2018 (May 18); 1 (1): e180105 NCT01692275Boudreau LA, Busse JW, McBride G.
Chiropractic Services in the Canadian Armed Forces: A Pilot Project
Military Medicine 2006 (Jun); 171 (6): 572–576Green BN, Johnson CD, Lisi AJ, Tucker J.
Chiropractic Practice in Military and Veterans Health Care:
The State of the Literature
J Can Chiropr Assoc. 2009 (Aug); 53 (3): 194–204Canada Parliament House of Commons.
Government Response to the Standing Committee’s Report on “Caring for Canada’s Ill and Injured Military Personnel”.
Ottawa; 2014.Robinson OC:
Sampling in interview-based qualiitative research: a theoretical and practical guide.
Qual Res Psychol 2014; 11: 25–41.Way D, Jones L, Busing N:
Implementation Strategies: Collaboration in Primary Care-Family Doctors & Nurse Practitioners Delivering Shared Care.
Toronto, The Ontario College of Family Physicians, 2000.Christine M. Goertz, Cynthia R. Long, Robert D. Vining, Katherine A. Pohlman,
Bridget Kane, Lance Corber, Joan Walter, and Ian Coulter
Assessment of Chiropractic Treatment for Active Duty, U.S. Military Personnel
with Low Back Pain: Study Protocol for a Randomized Controlled Trial
Trials. 2016 (Feb 9); 17 (1): 70Dorflinger L, Moore B, Goulet J, et al:
A partnered approach to opioid management, guideline concordant care and the stepped care model of pain management.
J Gen Intern Med 2014; 29(Suppl 4): 870–6.Pope C, Mays N:
Qualitative Research in Health Care, 3rd ed.,
Hoboken: NJ, Blackwell, 2007.Glaser B, Strauss A:
The Discovery of Grounded Theory. Strategies for Qualitative Research.
Chicago, IL, Aldine Publishing, 1967.Strauss A, Corbin J: Basics of Qualitative Research:
Techniques and Procedures for Developing Grounded Theory.
Thousand Oaks, CA, Sage, 1998.Morgan DL:
The Focus Group Guidebook.
Thousand Oaks, SAGE Publications, 1998.Verhoef MJ, Mulkins A, Boon H:
Integrative health care: how can we determine whether patients benefit?
J Altern Complement Med 2005; 11(Suppl 1): S57–65.Morse JM, Field PA:
Qualitative Research Methods for Health Professionals, 2nd ed.,
Thousand Oaks, SAGE Publications, 1995.Sandelowski M:
Whatever happened to qualitative description?
Res Nurs Health 2000; 23(4): 334–40.Auditor General of Canada.
Chapter 4—Military Health Care—National Defence
in Report to the Auditor General Of Canada to the House of Commons, October, 2007.
Ottawa: Office of the Auditor General of Canada.
http://www.oag-bvg.gc.ca/internet/English/parl_oag_200710_04_e_23828.htmlBusse JW, Jim J, Jacobs C, et al:
Attitudes towards chiropractic: an analysis of written comments from a survey of North American orthopaedic surgeons.
Chiropr Man Therap 2011; 19(1): 25.Herman PM, Coulter ID:
Complementary and Alternative Medicine: Professions or Modalities?
Policy Implications for Coverage, Licensure, Scope of Practice,
Institutional Privileges, and Research.
RAND Corporation, Santa Monica, California: (2015. pp. 1–76)Lisi AJ, Khorsan R, Smith MM, Mittman BS.
Variations in the Implementation and Characteristics of Chiropractic Services in VA
Medical Care 2014 (Dec); 52 (12 Suppl 5): S97–104Mior SA, Barnsley J, Boon H, Ashbury FD, Haig R.
Designing a Framework for the Delivery of Collaborative Musculoskeletal Care
Involving Chiropractors and Physicians in Community-based Primary Care
J Interprof Care. 2010 (Nov); 24 (6): 678–689Theberge N:
“We have all the bases covered”. Constructions of professional boundaries in sport medicine.
Int Rev Sociol Sport 2009; 44(2): 265–81.Safai P:
The demise of sport medicine and science council of Canada.
Sport Hist Rev 2005; 36: 91–114.Reeves S, Lewin S, Espin S, Zwarenstein M:
Interprofessional Teamwork for Health and Social Care.
Chichester, Wiley-Blackwell, 2010.Saks M:
Inequalities, Marginality and the Professions
Current Sociology Review 2015; 63 (6): 850–868
Return to CHIROPRACTIC CARE FOR VETERANS
Since 8-10-2019
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |