

The Role of Vitamins and Minerals
in Energy Metabolism and Well-beingThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J International Medical Research 2007 (May); 35 (3): 277–289 ~ FULL TEXT
Huskisson E, Maggini S, Ruf M.
King Edward VII Hospital,
London, UK.
Physicians are frequently confronted with patients complaining of fatigue, tiredness and low energy levels. In the absence of underlying disease, these symptoms could be caused by a lack of vitamins and minerals. Certain risk groups like the elderly and pregnant women are well-recognized. Our aim was, therefore, to find out if other, less well-established groups might also be at risk.
Thus, the objectives of this review are: to describe the inter-relationship between micronutrients, energy metabolism and well-being; identify risk groups for inadequate micronutrient intake; and explore the role of micronutrient supplementation in these groups. A review of the literature identified an important group at risk of inadequate micronutrient intake: young adults, often women, with a demanding lifestyle who are physically active and whose dietary behaviour is characterized by poor choices and/or regular dieting. Micronutrient supplementation can alleviate deficiencies, but supplements must be taken for an adequate period of time.
From the FULL TEXT Article:
Introduction
Every doctor is familior wi1b the patient who presents complaining of a lack of energy. tiredness and exhaustion, and for whom thorough examination and even routine laboratory tests do not provide a satisfactory explanation for their symptoms. Without any underlying diseases, might these symptoms be caused by a lack of vitamins and minerals?
There are more articles like this in our:
Nutrition SectionResearch in the latter half of the 20th century has dramatically increased our understanding of the biochemical processes of cellular energy generation and demonstroted the fundamental role of a large number of vitamins and minerals as coenzymes and cofactors in these processes. This paper is based on the recognition that a lack of micronutrients may impair cellular energy production, resulting in symptoms of tiredness and lack of energy. In the first part of the paper, we summarize the current understanding of the role of micronutrients in energy generation and discuss the implications of micronutrient deficiency for energy and well-being. In the second pent of the paper, we discuss the potential role of micronutrient supplements in improving the well-being of patients complaining of lack of energy and whether doctors should recommend such supplements.
This review focuses on 'healthy' adults with active and demanding lives. It refers only briefly to athletes and sports performance, because comprehensive reviews about these groups and their specific needs can be found easily in the literature. For the same reason, we will also exdude very well-known risk groups. such as the elderly and those with vitnmin B12 and iron deficiency.
Energy metabolism in the body
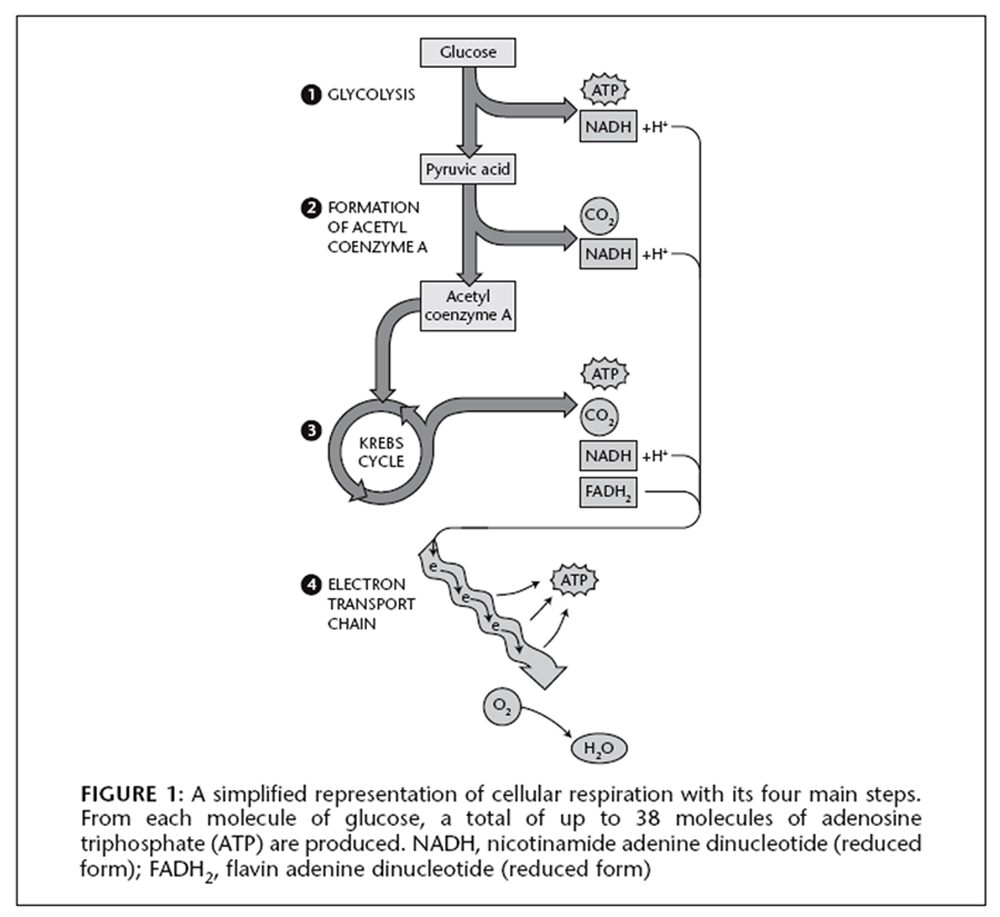
Figure 1 Energy to power the body's metabolic processes is derived from the food that we eat. Various readions in catabolic pathways release this energy, and store it in the high-energy phosphate bonds of the body's energy storage molecule, adenosine tripbosphate (ATP). The process by wbich energy is transformed into ATP is known as cellular respiration (Figure 1). The main part of this cellular respiration happens in the mitochondria, often referred to as the power plants of the cell. Glucose is the body's preferred source of energy for the production of ATP but, if necessary, other carbohydrates, fats and proteins can also be metabolized to acetyl coenzyme A (CoA). enter the citric add (Krebs) cyde and be oxidized to carbon dioxide and water.
Roles Of Micronutrients In Energy Metabolism
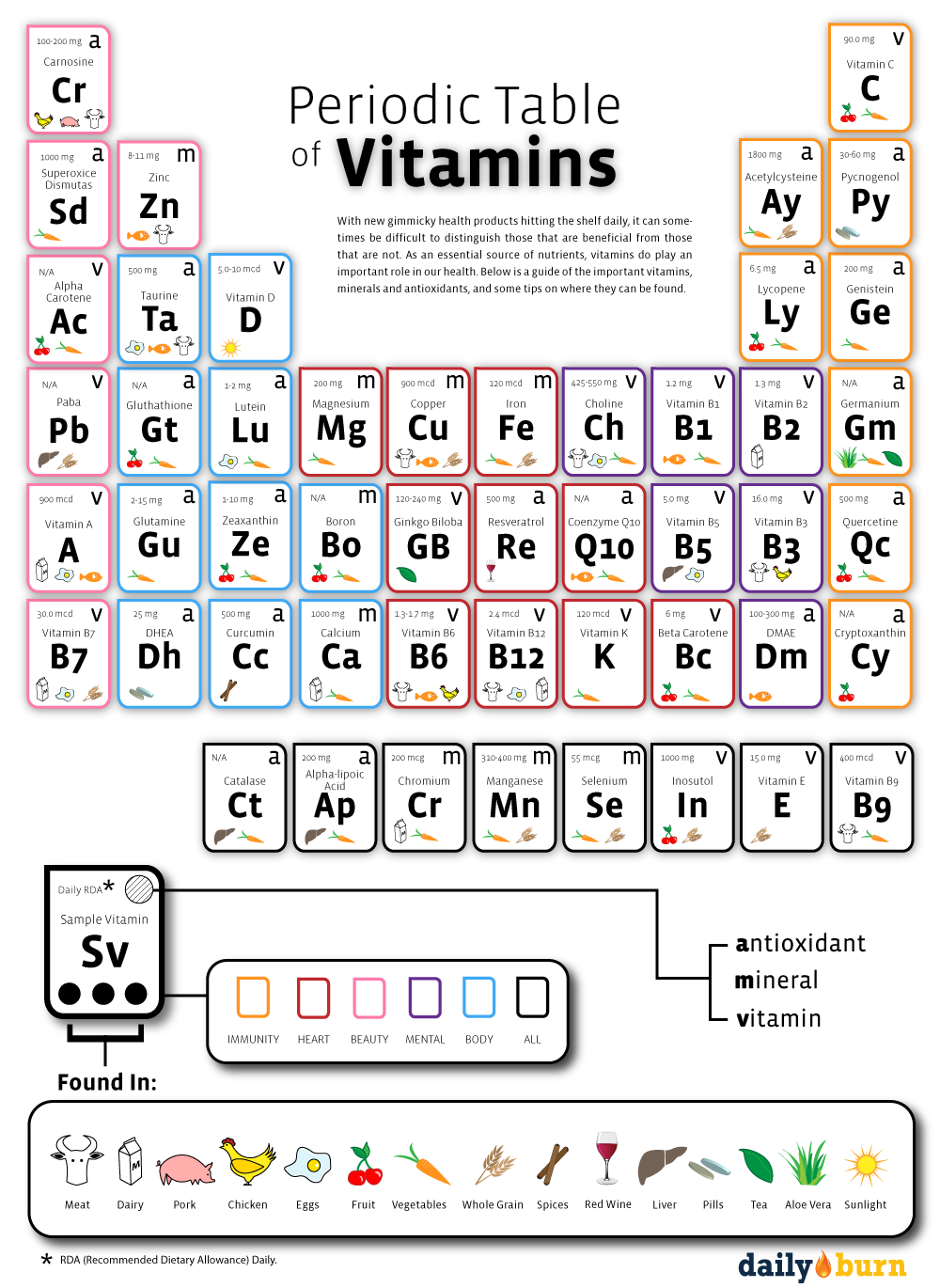
The transformation of dietary energy sources, such as carbohydmtes, fats and proteins into cellular energy in the form of ATP requires several micronutrients as coenzymes and cofactors of enzymatic reactions as structural components of enzymes and mitochondrial cytochromes, and as active electron and proton carriers in the ATP-generating respiratory chain: [1, 2](i) thiamine pyrophosphate (TPP; Vitamin B1),
CoA (containing pantothenic acid),
flavin mononucleotide (FMN; derived from Vitamin B2),
favin adenine dinudeotide (FAD; derived from Vitamin B2), and
nicotinamide adenine dinucleotide (NAD; derived from nicotinamide)
are involved in the Krebs cyde and complexes I and II of the respiratory chain;
(ii) biotin,
CoA and
FAD
are involved in haem biosynthesis, which is an essential part of the cytochromes and important for the latter part of the mitochondrial respiratory chain;
(iii) succinyl-CoA can feed into either the respiratory chain or the Krebs cycle depending on the needs of the cell.

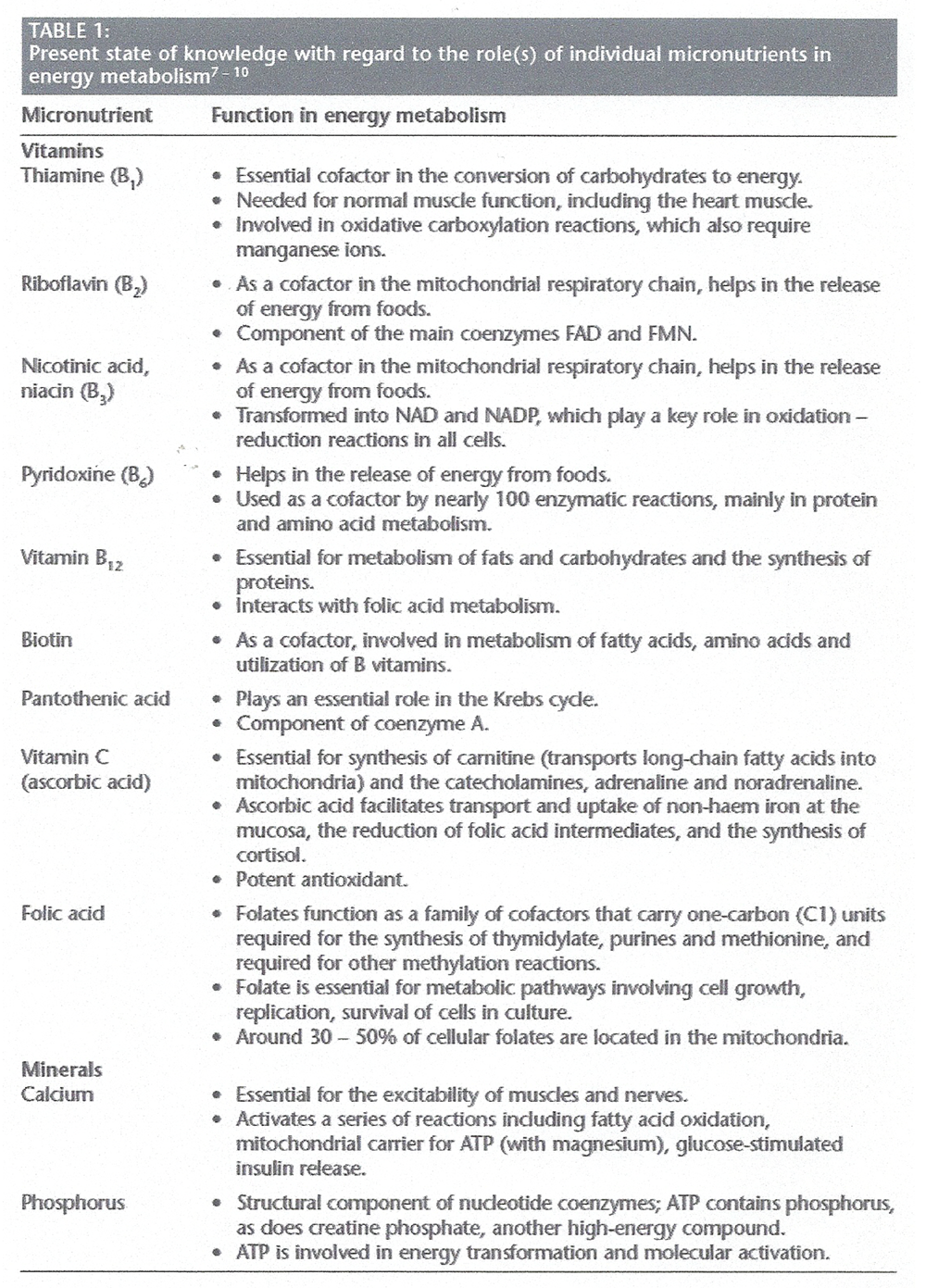
Table 1 A
Table 1 B In addition, the respiratory chain in the mitochondria also involves iron - sulphur (Fe - S) centres containing either two or four iron atoms that form an electron transfer centre within a protein.
The role of vitamins in energy metabolism continues to attract research interest. Depeint et al. confirmed the essential role of vitamins B6, B12 and folate in maintaining the mitochondrial one-carbon transfer cycles by regulating mitochondrial enzymes. The same authors also emphasized the essential role of the B vitamin family in maintaining mitochondrial energy metabolism and how mitochondria in their role as the cellular organelles responsible for energy metabolism are compromised by a deficiency of any B vitamins. [3]
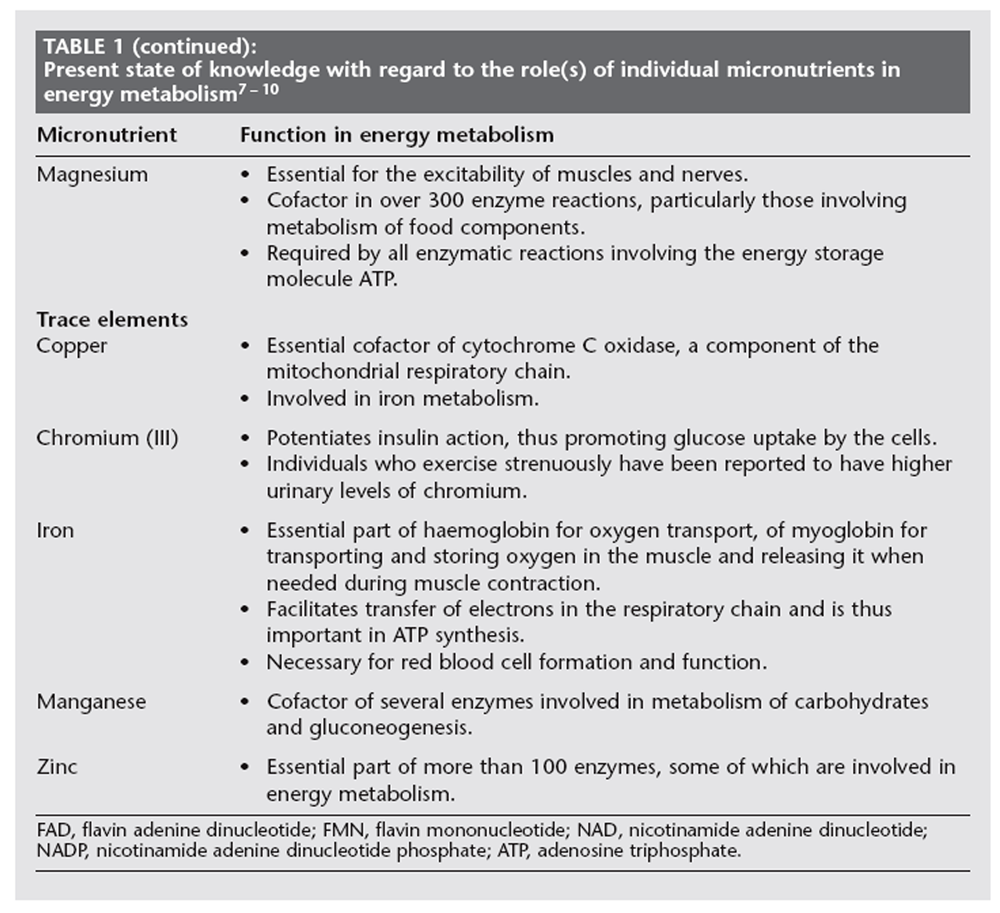
As with the B vitamins, the role of certain minerals in energy metabolism is the subject of increasing interest. For example, a recent review noted the importance of adequate amounts of magnesium, zinc and chromium to ensure the capacity for increased energy expenditure and work performance, and that supplemental magnesium and zinc apparently improve strength and muscle metabolism. [4] A subsequent paper investigated the effects of magnesium depletion on physical performance and found that it resulted in increased energy needs and an adverse effect on cardiovoscular function durtng sub-maximal work. [5] Most recently Lukaski has shown that low dietary zinc also impairs cardiorespiratory function during exercise. [6] Table 1 summarizes the present state of knowledge with regard to the role(s) of individual micronutnents in energy metabolism. [7–10]
Inadequate micronutrient intake
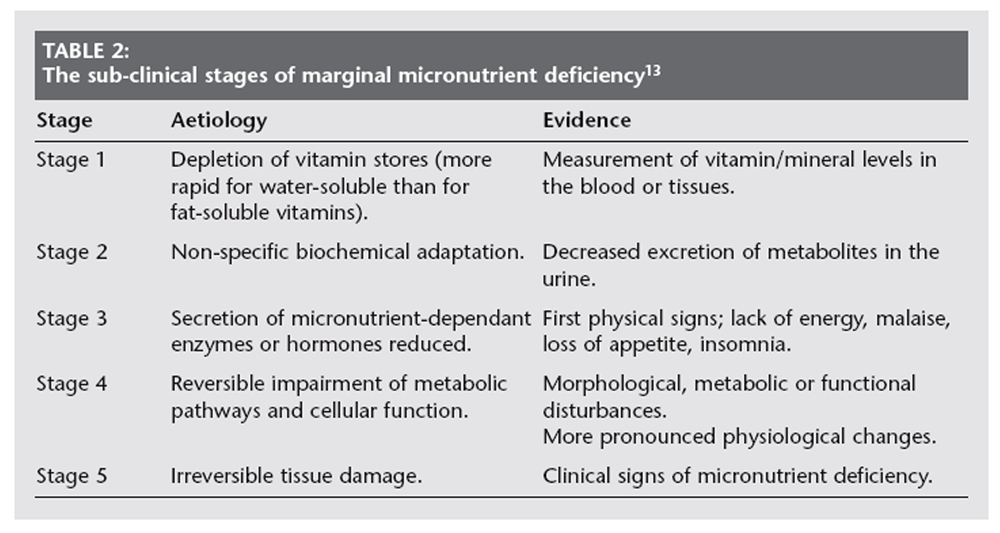
Table 2 The serious consequences of profound vitamin deficiency have been recognized for more than a century. Mainly as a result of better general nutrition and of micronutrient supplementation in at-risk groups, the deficiency diseases, such as rickets, pellagra, scurvy and beriberi, are now relatively uncommon. at least in the developed world. But, within the past two decades, a number of investigators [11, 12] have re-introduced the concept of marginal micronutrient deficiency, first proposed by Pietrzik in 1985. [13] This showed that, long before the clinical symptoms of deficiency appear, micronutrient deficiencies develop progressively through several sub-clinical stages (Table 2).
Marginal deficiencies may occur as a result of inadequate micronutrient intake, caused by poor diet, malabsorption or abnormal metabolism. Whether in the developed or the less developed world, the overwhelming majority of cases fall into stages 1–3 (Table 2) and are further referred to as an inadequate micronutrient status. Ideally, a sufficient and balanced diet should cover the overall micronutrient requirements. Unfortunately, even in developed countries, many sections of the population do not receive the essential vitamins and minemls needed from their diet Several groups in the population are at increased risk for inadequate micronutrient status, usually due to insufficient intake caused by weight-reducing diets, insufficient and/or imbalanced nutrition, eating disorders, or demanding periods such as extensive exercise or emotional and/or physiological stress. Increased requirements may also cause an inadequate vitamin and mineral status; for example, as may occur in pregnancy and lactation, during growth in the elderly, smokers and chronic alcohol abusers, and in patients with certain underlying diseases. [14–17]
Even otherwise 'healthy' individuals can be at risk due to lifestyle-related factors. The 'lifestyle' category typically indudes young to middle-aged adults with high occupational pressure or the double burden of family and work, for whom time is always in short supply. In this group, the risk for an inadequate micronutrient status is often the result of lifestyle-associated behavior; such as rushed meals, unhealthy food choices, chronic or periodical dieting, and stress- related behavior, such as smoking, exoessive alcohol and coffee consumpuon. [18]
Even mild micronutrient deficiencies can result in a lack of well-being and general fatigue, redured resistnnce to infections or impaired mental processes (e.g. memory. concentration, attention and mood). [8, 9] Recent studies have indicated that an optimal intake of cartain vitamins is also cructal for long-term health maintenance and to help prevent diseases, such as osteoporosis, coronary heart disease and cancwe. [19, 20]
The risk of developing an inadequate micronutrient status is more common in industrialized populations than is generally assumed. In the 1987–1988 Dutch National Food Consumption Survey [21] combinations of low thiamine, riboflavin, vitamin B6 and vitamin C intakes were found among adults. A double-blind study demonstrated that a state of depletion of thiamine, riboflavin, and vitamin B6 and C can be induced within 8 weeks by a diet composed of normal food products. [22]
Within 3–6 weeks, deterioration of the vitamin status was indicated by decreased vitamin concentrations in the blood, decreased erythrocyte enzyme activities, elevation of stimulation tests of these enzymes and lower vitamin excretion in the urine. [22] Although no vitamin-specific clinical signs and symptoms of deficiency were observed, tbis depletion study showed that the combined marginally deficuent status of thiamine, riboflavin, vitamin B6 and vitamin C decreased physcal performance. Marginal vitamin B6 intake is among the nutritional risks prevalent in the Netherlands. [23]
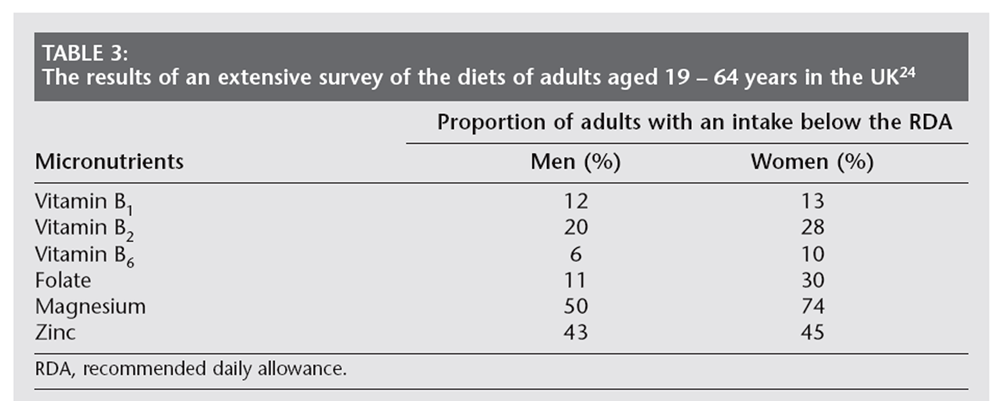
Table 3 Vitamin and mineral intnke was recently assessed in the UK in an extensive survey carried out in adults aged 19–64 years living in private households. [24]Data from more than 2,250 dietary interviews were gathered, along with more than 1,700 7–day doetary records. In general, the intake data for vitamins and minemls were satisfactory. showing an average Intake from food sources and supplements combined that met or exceeded the local recommended daily allowance (RDA) for each individual micronutnent. [24] However, when only dietary intake was considered and when looking at the stratified intake data, significant proport:ions of the population were found to have intakes below the RDA. as shown in Table 3. [24]
Data from the USA hove shown that, even in the generol population, the prevalence of low serum folate (18.4%) and of low red- blood cell folate (45.8%) was quite high. [25] This, In addition to the weIl-recognized roles of folate in human health, prompted the start of the mandatory folic acid fortification programme in 1998 in the USA. [25] Dutch data also indicated that arund 50% of a representative Dutch population sample did not meet current recommendations for folate intake. [26] Recently, it was reported that folic acid deficiency in adolesrent teenage girls in Turkey ranged between 14.7% and 20.1% in rural and urban areas, respectively. [27]
Another vitamin of concern is vitamin D; inadequate Vitamin D status is becoming more common in developed countries. Vitamin D inadequacy is found in approxbnately 36% of otherwise healthy adults oveeall, in up to 57% of patients seen in general medicine in the USA and at even higher percentages In Europe. [28]
Dietary magnesimn does not generally meet recommended intakes for adults. Results of a recent national survey in the USA, for example, indicated that a substantiol proportion of women do not consume the recommended daily intake of magnesium; with the menopause this problem increases among women over 50 years 0ld. [5] The average magnesium intake for women was found to be 228 mg/day compared with the recommendation of 320 mg/day by the US Institute of Medicine. [5] This avemge intolte amount was derived fium a l–day diet recall and, thus, may be an overestimate of actual magnesium intake.
Magnesium has also been proposed as a limiting nutrient for exercise and performonre. Surveys of physimlly active individuals indicate that magnesium intakes among certain groups of athletes do not meet recommendations for adults. [4] A few reports have indicated that magnesium supplements enhance strength and improve exercise performance. [29] However, it is unclear whether these effects are related to remediation of on existing magnesium inadequacy or a pharmacological effect. [5]
In both Europe and the USA, iron deficiency is considered to be one of the main nutritional deficiency disorders, affecting large proportions of the population, particularly cbildren, and menstuating and pregnant women. [30–33]
Low consumption of foods rich in bioavailable zinc, such as meat, particularly red meat, and a high consumption of foods rich in inhibitors of zinc absorption. such as phytate, oertain dietary fibres and calcium, impair the recommended zinc status. Inadequate zinc intake, resulting in a suboptimal zinc status, has been recognized in many population groups, both in less developed and in industrialized countries. Althougb the cause of this may be inadequate dietary intake of zinc, the most likely reason is the consumption of inhibitors of zinc absorption. [34] Women, dieters and the elderly are particularly at risk of being low in zinc. [25, 36] Surveys of physically active subjects also indicate that low dietary zinc is common, espedally among individuals who participate in aerobic activities, such as those reoommended to promote health and well-being. [6]
With respect to minerals and trace elements in general, it is well established that rigorous exertise leads to greater losses, particularly of magnesium, iron, zinc and chromium in sweat and urine. [37–40]
In condusion, the risk of an inadequate micronutrtent intake may be provoked by the following different conditions and situations:
Elevated needs due to the induced synthesis of those enzymes important to energy metabolism which, in turn, increases the requirements for micronutrient cofactors. [41]
Increased loss of minerals, such as magnesium and iron, due to sweating during exercise and in the urine. [37–40] In general, micronutrtent deficiencies caused by high physiml activity (e.g. among active individuals and athletes) are well documented: 8 vitamins, vitamin C, iron [42] vitamin B2 in young women athlletes, [43, 44] B vitamins, vitamin C; [45] and vitamin B6 following marathon running. [46]
Increased need because of dieting and/or a poor diet, especially in combination with a demanding lifestyle. This is especially true of women living an active life who frequently reduce intake of food to lose weight as well as making poor dietary choices. Such women have a paeticular risk for insuffictent B vitamin status. Lifestyle-induced micronutrient deficiency results in reduced physical performance, increased fatigue and tiredness. [47, 48]
Groups such as pregnant women or the elderly must be mentioned, although they are not further considered in this review.
Consequences of inadequate micronutrient intake for physical well-being
Given the importance of micronutrients in energy metabolism it is not surprising that mitochondrial functions are compromised by insufficient dietary intake of B vitamins and/or increased 8 vitamin needs. [3] Unfortunately, clinical data on the interactions between micronutrient metabolism and physical performamce are limited. This is mainly because study designs have not been suffictentIy comprehensive to allow reasonable conclusions to be drawn due to the complexity of cellular respiration and the body's ability to utilize alternative pathways of energy production in an emergency. Nevertheless. it has been shown that deficiencies in folate and vitamin B12 reduce endurance work performance and that an inadequate intake of minerals impairs performance. [29]
Studies of the effects of restricted diets on physical performance have not only emerged from sports medicine, but also as a 'women's health issue'. Concerns about the health effects of chronic dieting in order to reduce body weight have been regularly voiced in both the medical and the lay press. In a comprehensive review of the health consequences of dieting in active women, a 'chronic dieter' is defined as an individual who 'consistently and successfully restricts energy intake to maintain an average or below-average bodily weight'. [47] The author notes that individuals with a poor energy intake usually have poor micronutrient intakes, especially of calcium, iron, magnesium, zinc and B complex vitamins. [47]
These micronutrients are particularly important for active individuals since, 'they play an important role in energy production, hemoglobin synthesis, maintenance of bone health and strength and an adequate immune fundion'. [47] Problems may arise for the active female who chronically diets and performance may suffer in athletes involved in esthetic or 'lean-build' sports, such as dancers, long distance runners, or gymnasts. who are under pressure to maintain a lean body shape for their sport. [47] For active females, 'poor physical performance can bave a devastating psychological effect, especially if physical performance is tied to job-related expectations. [47]
Support is given to these conclusions by a Spanish study that investigated energy intake as a determinant factor of vitamin status in healthy young women. [45] In this study, the vitamin status (B1, B2, B6, retinol, beta carotene, C and E) of 56 healthy young women was analysed and related to energy intakes. A high percentage of these apparently healthy young women had deficient or marginally deficient blood levels of most of the vitamins, with adequate or optimal levels only shown for vitamins C, E and retinol. The authors concluded that young women, especially those consuming low-energy diets, are vulnerable to developing marginal vitamin deficiencies. Taken together, there is good evidence that dietary restriction does result in an inadequate micronutrient status and that this may, in turn, impair physical performance. [45, 47]
If deficiency of micronutrients can impair physical performance, conversely physical activity may deplete micronutrient status. In a metabolic study, young women were fed various amounts of riboflavin (vitamin B2) over a 10–week period and their riboflavin status was monitored. [43] When 20–50 min/day of exercise for 6 days a week was introduced, riboflavin levels declined but were restored when dietary riboflavin levels were concomitantly increased. A similar study found that, in the weeks when subjects exercised, riboflavin status declined significantly compared with the weeks in which no exercise was performed. [44]
More recently, a double-blind, randomized, crossover study investigated the effects of zinc deficiency on physical performance. [6] Fourteen young men were fed a low-zinc diet for 9 weeks and, following a 6–week washout period, they were then fed a zinc-supplemented diet for a further 9 weeks. Blood and fecal determinations of zinc status and balance, and physiological testing were performed at specific times during each dietary period. The authors concluded that low dietary zinc was associated with impaired cardiorespiratory function and impaired metabolic responses during exeecise. In establishing the 1998 dietary reference intake (DRI) for riboflavin, the US Institute of Medicine considered data from a number of membolic studies and concluded that requirements might be higher in active individuals, but the amount of existing data was not sufficient to quantify the requuirement. [8]
A number of studies have indicated that vitamin B6 is lost as a result of exercise, although the magnitude of the loss is small. Vitamin B6 is required to maintain plasma concentrations of pyridoxal 5'-phosphate (PLP). Blood studies show that PLP levels rise rapidly during exercise, indicating consumption of vitamin B6. [48] In subjects with an adequate B6 intake, the levels fall back to baseline within 30–60 minutes after exercise. [48] As an example, it was calculated that marathon runners lose about 1 mg vitamin B6 during a marathon, equivalent to the DRI for an adult. [46]
In a review of the effect of physical activity on thiamine, riboflavin and vitamin B6 requirements [48] it was concluded that, because exercise stresses metabolic pathways that depend on thiamine, riboflavin and vitamin B6, the requirements for these vitamins may be increased in active individuals. Since exercise seems to decrease nutrient status even further in those with pre-existing marginal vitamin intakes or body stores, individuals 'who restrict their energy intake or make poor dietary choices are at greater risk for poor thiamine, riboflavin and vitamin B6 status'. [48]
In 2001 Speich et al. [49] published a review of 24 studies carried out between 1994 and 2000 into the significance of levels of 16 minerals and trace elements for physical performance. They concluded that, although many of these minerals are involved in aspects of energy metabolism, for most their precise physiologiml role is still unclear. This uncertainty underlines the need for further research. A better understanding about micronutrients and energy metabolism is even more urgent because, besides the impact on physical well-being, currently the long-term health consequences for humans with marginal B vitamin deficiencies are not known. [3]
Micronutrient supplementation
It is a well-known fact that, often encouraged by their coaches; sports people and athletes are malor consumers of multivitamins/mineml supplements. As an example, Armstrong and Maresh [42] cite studies from Australia showing that 30%–100% of athletes in different sports have taken supplements. With regard to the effects of micronutrient supplementation on physical performance, the literature generally indicates that a positive effect on physical performance is only detectable when the dietary intake of these nutrients is not adequate. This is supported by the most recent review of this topic. in which the author conduded that the use of vitamin and mineral supplements did not improve measures of performance in people consuming adequate diets. [29] However, 'young girls and individuals participating in activities with weight classifications or esthetic components are prone to nutrient deficiencies because they restrict food intake and specific micronutrient-rich foods'. [29]
Do the findings in athletes also apply to 'normal' people with only moderate physical activity? Young women at risk of micronutrient deficiency because of chronic dieting have been identified [47] and, in a subsequent paper, it was shown that the risk of deficiency was greatest in physically active women with pre-existing marginal vitamin status. [48] Indeed, both Manore [48] and Lukaski [29] identified the same high risk group, but from different perspectives: Lukasld studied athletes and identified an 'at risk' subgroup of young women who restrcted their diet; [29] while Manore studied chronic dieters and identified an 'at risk' subgroup who were physically active. [48] Both authors concurred that multivitaminl mineml supplementation may be beneficial for such women.
Finally, a generally well-recognized group for inadequate micronutrient intake is the elderly. Diet, micronutrient status and the benefits of supplementation have been much studied in the elderly, however most studies have concentrated on the effects of defidency on susceptibility to infection and, more recetly, cognitive function. [18] However, lack of energy, tiredness, weakness and, paradoxically, loss of appetite are frequent complaints of older people. A recent study confirmed earlier pan-European findings that between 39% and 78% of elderly subjects had dietary intakes of vitamin A, calcium and iron below the lowest European RDA; [50] the relationship between micronutrient insufficiency and energy in this group warrants further study.
As to how long to continue supplementation, the evidence suggests that an inadequate micronutrient status may take several weeks to develop and, once it occurs, it may take an equally long time to replenish body stores. Altbough data are limited, an experimental study showed that it took around 6 weeks for daily supplementation of vitamin B6 to restore optimum blood levels. [51] Based on this and clinical data with multivitamin products, [52, 53] a treatment period of at least 40 days is usually recommended.
Uchtenstein and Russell [54] recently concluded that there are strong reasons to make recommendations for the use of dietary supplements by certain segments of the population. 'Supplements are relatively inexpensive and can be reliably used to administer nutrients in precise doses. If used consistently, supplements can ensure adequate intakes of spedfic nutrients in targeted groups that have increased needs for those nutrients because of physiologic limitations or changes'. [54]
Conclusion
An overwhelming body of physiological evidence confirms the fundamental role of vitamins and minerals in energy metabolism. In particular. the B complex vitamins are essential for mitochondrial function and a lack of just one of these vitamins may compromise an entire sequence of biochemical reactions necessary for transforming food into physiological energy. It is also clear that several minerals and trace elements are essential for energy generation, although more research is needed to elucidate their precise role.
Inadequate intake of micronutrients, or increased needs, impairs health and increases susceptibility to infection, but may also result in tiredness, lack of energy and poor concentration. Besides generally accepted risk groups like the elderly, an important group who are at risk of an inadequate micronutrient intake – especially of the B vitamins – are young to middle-aged adults. These are often women with a demanding lifestyle who are physically active and whose dietary behaviour might be characterized by poor choices and/or regular attempts to lose weight.
Given the importance of micronutrients for energy metabolism and the risk for an inadequate micronutrient status in otherwise healthy individuals, multivitamin-mineral supplementation is recommended for patients complaining of chronic lack of energy and in whom underlying disease has been exduded. Where such supplements are prescribed or recommended they should be taken for an adequate period of time, ideally not less than 6 weeks, to obtain a noticable effect on physical well-being.
Conflicts of interest
Silvia Moggini and Michael Ruf are employed by Boyer Consumer Care, a manufacturer of multivitamins.
References:
Return to NUTRITION
Since 7–05–2018

| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |