

The Influence of Neck Pain on Sensorimotor Function in the Elderly This section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Arch Gerontol Geriatr. 2012 (Nov); 55 (3): 667–672 ~ FULL TEXT
Sureeporn Uthaikhup, Gwendolen Jull, Somporn Sungkarat, Julia Treleaven
Department of Physical Therapy,
Faculty of Associated Medical Sciences,
Chiang Mai University,
Thailand.
sureeporn.uthaikhup@cmu.ac.th

Greater disturbances in sensorimotor control have been demonstrated in younger to middle aged groups. However, it is unknown whether or not the impairments documented in these populations can be extrapolated to elders with neck pain. The aim of this study was to investigate the influence of neck pain on sensorimotor function in elders. Twenty elders with neck pain (12 women and 8 men) and 20 healthy elder controls (14 women and 6 men) aged 65 years and over were recruited from the general community. Tests for sensorimotor function included; cervical joint position sense (JPS); computerised rod-and-frame test (RFT); smooth pursuit neck torsion test (SPNT); standing balance (under conditions of eyes open, eyes closed on firm and soft surfaces in comfortable stance); step test and ten-meter walk test with and without head movement.
Elders with neck pain had greater deficits in the majority of sensorimotor function tests after controlling for effects of age and comorbidities. Significant differences were found in the SPNT (p<0.01), error in the RFT (frame angled at 10° and 15° anticlockwise) (p<0.05), standing balance (amplitude of sway) - eyes open on a firm surface in the medio-lateral (ML) direction (p=0.03), and total number of steps on the step test, both left and right sides (p<0.01).
Elders with neck pain have greater sensorimotor disturbances than elders without neck pain, supporting a contribution of altered afferent information originating from the cervical spine to such disturbances. The findings may inform falls prevention and management programs.
There are more articles like this @ our:
SENIOR CARE PageKEYWORDS: Balance; Falls risk; Mobility-limitation; Musculoskeletal pain; Older adults
From the FULL TEXT Article:
Introduction
The prevalence of neck pain in community dwelling elders is estimated as 40.5% in women and 36.1% in men (March et al., 1998). It is important to understand the contribution of neck pain to sensorimotor disturbances in elders as postural instability increases the risk of falling (Shumway-Cook et al., 2000; Hawk et al., 2006; Pajala et al., 2008).
Neck pain can be associated with dizziness, unsteadiness and visual disturbances and it can also affect postural stability, cervical proprioception and head and eye movement control (Treleaven, 2008a; Kristjansson and Treleaven, 2009). The vestibular and visual systems are vital to sensorimotor control but there is also evidence for the important contribution of cervical proprioception (Bolton, 1998; Treleaven, 2008a; Kristjansson and Treleaven, 2009). The deep sub-occipital muscles contain a high density of muscle spindles (Kogler et al., 2000; Rix and Bagust, 2001; Boyd- Clark et al., 2002). Bove et al. (2002) and Courtine et al. (2003) demonstrated that stimulation of the muscle spindle afferents via neck muscle vibration not only influenced balance but also walking and running in healthy individuals. In addition, a recent study of experimentally induced neck pain illustrated the destabilizing effect of neck muscle pain on standing balance (Vuillerme and Pinsault, 2009).
Increasing age is accompanied by changes in vestibular, visual and neuromuscular function (Ahmed et al., 2005). Declines in these systems are a normal consequence of aging. Greater disturbances in sensorimotor control have been demonstrated in healthy elders when compared to the middle aged in terms of larger cervical joint position errors, postural imbalance and impaired gait (Woollacott and Tang, 1997; Gill et al., 2001; Jacobson et al., 2008; Schrager et al., 2008; Vuillerme et al., 2008; Liaw et al., 2009). In relation to neck pain, increased cervical joint position error, poor eye movement control and balance disturbances have been demonstrated in younger to middle aged groups with both idiopathic and whiplash induced neck pain (Field et al., 2008; Humphreys, 2008; Treleaven, 2008a,b). These findings have informed rehabilitation programs (Jull et al., 2008). It is unknown whether or not the impairments documented in these populations can be extrapolated to elders with neck pain. One study has investigated the influence of neck pain on balance and gait parameters in community-dwelling elders, with findings suggesting that neck pain might contribute to disturbances in balance and gait over and above that which occurs with normal aging (Poole et al., 2008). A comprehensive range of sensorimotor functions is yet to be investigated specifically in the elderly with neck pain.
This study investigated eye movement control, cervical proprioception, postural stability and gait parameters in elders with neck pain to determine if there were any deficits in sensorimotor function above those which could be attributed to aging. It has been shown that fear of falling is associated with gait and balance abnormalities (Chamberlin et al., 2005) even without a history of falls (Maki, 1997). Thus fear of falling and its association with postural stability and gait were also assessed.
Subjects and methods
Participants
Forty elderly volunteers aged 65 years or older, with (n = 20) and without neck pain (n = 20) were included in the study. Participants were recruited from a metropolitan area using a method of convenience sampling and through advertising. To be eligible for the neck pain group, participants had to have neck pain as a predominant complaint, where neck pain is defined as pain and stiffness in the neck with or without radiating pain to shoulders and the upper limbs. Neck pain was to be of no less than 3 months duration with a score of at least 10 out of 100 on the Neck Disability Index (NDI) (Vernon and Mior, 1991). Participants were excluded if they had major comorbidities which could affect measures including: previous history of orthopedic surgery, a current acute musculoskeletal injury, lumbar spine or lower limb arthritis for which they had sought active management, neurological problems (e.g. stroke, Parkinson’s disease), diabetes, and cognitive impairment. Ethical approval for the study was granted by the Institutional Medical Ethics Review Committee and the study was conducted in accordance with the declaration of Helsinki. Written informed consent was provided before participation.
Questionnaires
Questionnaires were administered to collect demographic data, intensity of neck pain (VAS), patient’s self-rated neck pain and disability (NDI), (Vernon and Mior, 1991) and balance confidence in daily activities (ABC) (Powell and Myers, 1995). As many conditions which are common with aging can influence gait, balance and other measures in this study, information concerning the presence of comorbidities (not encompassed in exclusion criteria) was also collected from each participant and coded as present or not in five categories.
The categories were(1) musculoskeletal conditions affecting the lumbar spine or lower limb;
(2) headache;
(3) dizziness;
(4) previous traumatic neck injury;
(5) taking more than four medications.Cervical proprioception
Joint position error (JPE): The Fastrak system was used to measure the subjects’ ability to relocate the natural starting head position following active movements from left and right rotation and extension. The method is similar to that previously described (Treleaven et al., 2003) and adapted from Revel et al. (1991). Absolute error was calculated with a customised software program (Matlab (7.0), Mathworks Inc., USA). Three repetitions of each movement direction were undertaken and the mean value of the error used for analysis.
RFT: The RFT was used to measure the subjects’ perception of verticality (Bagust, 2005). The test was presented with a white square (the frame) and a white line (the rod) on a plain black background. The rod was positioned within the frame and rotated independently of the frame. A sequence of 12 random presentations was administered for the vertical perception test. The frame was set at 08, and at 108 and 158 in both clockwise and anticlockwise directions from the vertical. For two presentations, there was no frame. The initial position of the rod was angled at 308 clockwise and anticlockwise. Subjects wore video goggles to reduce the presence of visual cues. They used a computer mouse to rotate the rod to what he/she perceived as the vertical. Two practices were undertaken for familiarization. Subjects wore their normal corrective lenses if necessary. The absolute error values from the true vertical were calculated for each test.Head and eye movement control
SPNT: Electro-oculography was used in the SPNT to assess disturbances in eye movement control. The method has been described elsewhere in detail (Tjell and Rosenhall, 1998; Treleaven et al., 2005a). The test was performed with the subject’s head and trunk in a neutral forward-looking position and then a torsioned position (head neutral, trunk in 458 rotation to the left and right). Subjects were instructed to perform three blinks (for recognition and elimination in data analysis) and then follow the light as closely as possible with their eyes. The SPNT test value was calculated as the difference between the average gain in the neutral and torsioned positions.
Postural stability
Standing balance: Standing balance was measured using a 40 cm x 60 cm stable computerised force platform. Changes in standing balance were measured in the ML and antero-posterior (AP) directions using established methodology (Field et al., 2008; Treleaven et al., 2008). Standing balance was tested in comfortable stance on a firm surface and on a soft surface (a piece of high density 10-cm thick foam placed on the force platform) with eyes open and closed. A 30-s time period was performed for each condition.
Step test: The step test was used to assess dynamic single limb stance (Hill et al., 1996). Subjects were asked to step one foot on and then off a 7.5 cm block as quickly as possible for 15 s and the number of steps was recorded. Both left and right sides were tested.
Ten-meter walk (TMW) test without and with head movement: The TMW test was used to measure self-selected walking speed, which is proposed as a global indicator of self-perceived physical function (Cress et al., 1995). Subjects were asked to walk along a 14-m walkway at their comfortable speed under three conditions: head facing straightforward, head turning from side to side, head moving updown. Time and number of steps were recorded for the intermediate 10 m to allow for acceleration and deceleration (Poole et al., 2008).Procedure
Participants were initially screened for inclusion and exclusion criteria and those meeting the inclusion criteria entered the study. On the testing day, all eligible subjects completed the questionnaires and then performed the tests. Standing balance was tested before the step test and walking task to prevent fatigue. For all postural stability tests, the investigator stood close to or walked beside the subjects as a safety measure to prevent falls. Subjects were given standardised instructions prior to the tests and were allowed rest breaks between tests.
Statistical analysis
Independent t-test and chi-square analyses were used initially to test for any between group differences in age, gender and comorbidities. For standing balance measures, root mean square (RMS) amplitude in millimeters (Labview, National Instruments) and total energy (Wavelet analysis using Daubechie filter 6) were analysed (Treleaven et al., 2005b). RMS was chosen to demonstrate the average amplitude traveled by the center of pressure and the total energy was the amount of energy of the sway signal. Analysis was conducted for both the AP and ML traces for each condition (Field et al., 2008; Poole et al., 2008). Normality of all data was assessed using Q–Q plots and data were transformed using log transformation.
Univariate and multivariate analysis of variance (MANOVA) were used to investigate any differences in outcome variables between the neck pain and control groups. Age and comorbidity categories are known to effect sensorimotor function (Tjell and Rosenhall, 1998; della Volpe et al., 2006; Akdal et al., 2009; Salzman, 2010). To focus foremost on the contribution of the neck, age and all comorbidity categories were entered separately as covariates in all analyses, regardless of significant differences between groups, to control for possible confounding factors. Statistical analyses were performed using SPSS software and a significance level was set at p < 0.05.
Results

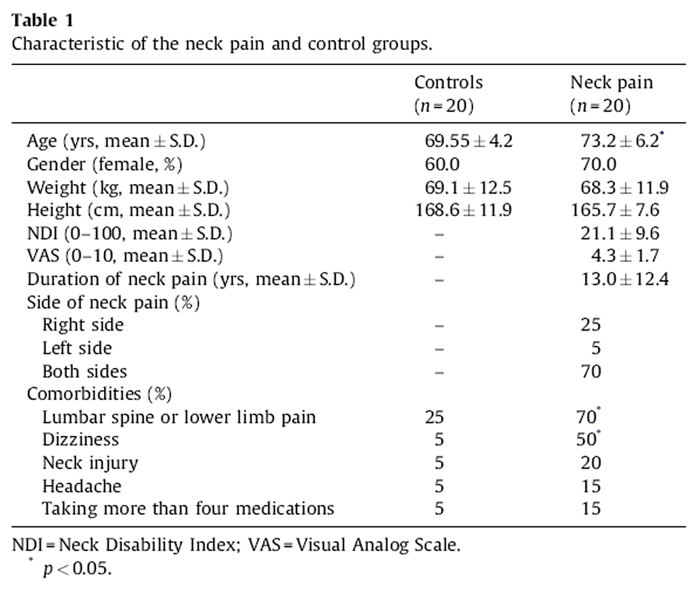
Table 1 Demographic data for the neck pain and control groups are presented in Table 1. Participants with neck pain were older and had more comorbidities than those without neck pain, reaching significance for the two categories of low back or lower limb pain and dizziness (p < 0.05).
As indicated, we considered age and every comorbidity category as covariates in analyses of all outcomes. Thus the results shown below were obtained after controlling for all potential confounding factors.
ABC scores
Table 2
Table 3
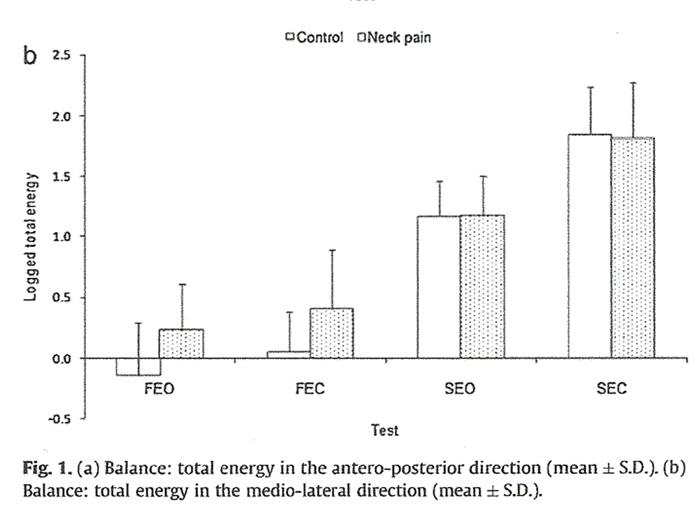
Figure 1
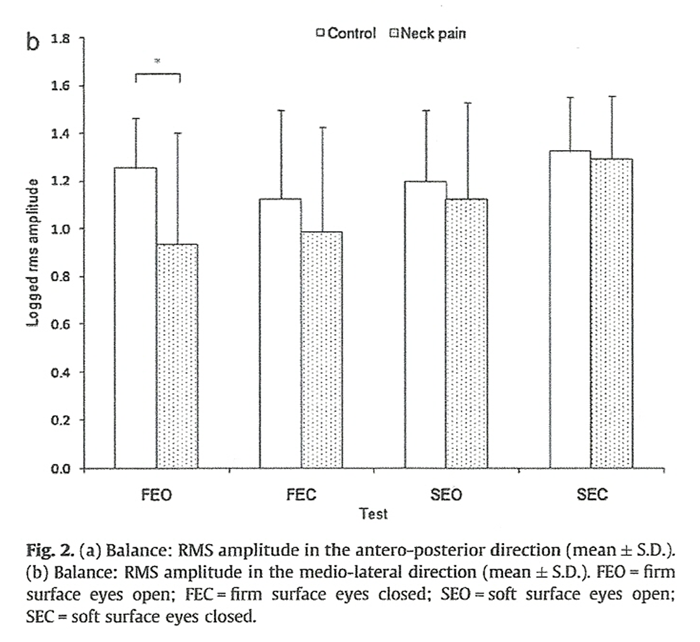
Figure 2 The mean balance confidence (ABC) scores were 86.6 ± 10.9 for the neck pain group and 97.0 ± 4.2 for the control group. There was a significant between-group difference in the ABC scores (p = 0.05).
Sensorimotor tests
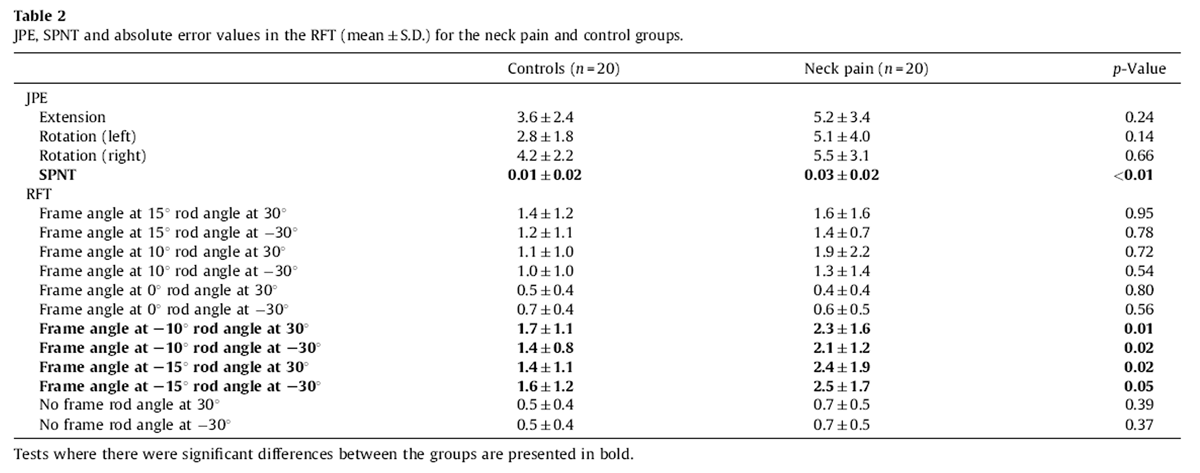
Table 2 presents the results of JPEs, SPNT and RFT between the neck pain and control groups. The neck pain group had significantly greater deficits in the SPNT and difficulty in perceiving the vertical when the frame was angled at 108 and 158 anticlockwise and the rod positioned at an angle of 308 clockwise and anticlockwise (all p ≤ 0.05). There were no significant differences between groups in JPEs (p > 0.05).
Table 3 presents total number of steps on the step test and the features measured in the TMW test for the neck pain and control groups. The neck pain group took significantly less steps than the control group on both left and right sides (p < 0.01). Deficits in gait parameters in the conditions of walking while turning the head from side to side and moving the head up-down were greater in the neck pain group compared to the control group however differences did not reach statistical significance (p > 0.05).
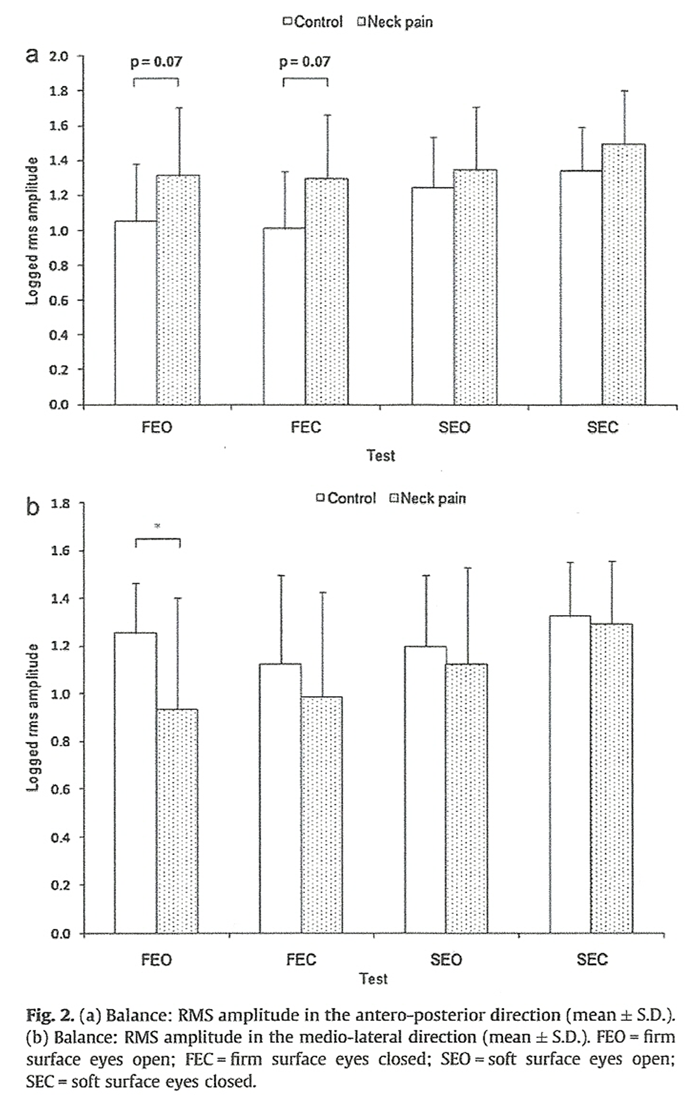
Figure 1a and b present the means, standard errors and the significant between group differences for the logged values for each condition in AP and ML directions for the total energy of the sway signal. Figure 2a and b present the values for the amplitude of sway (RMS). There were no differences between the groups in total energy of the sway signal over all tests (p > 0.05). The RMS amplitude values were significantly less in the neck pain group in the tests of eyes open on the firm surface in the ML direction (p = 0.03). There were also trends for greater RMS amplitude values in the tests of eyes open (p = 0.07) and closed (p = 0.07) on the firm surface in the AP direction.
Discussion
This study revealed that elders with neck pain demonstrated greater deficits in eye movement control, perception of verticality and balance when compared to healthy elders even after controlling for all potential confounding factors (age and comorbidities) that may have influences on the outcome measures. Additionally, they also had significantly lower levels of selfconfidence in performing activities. The greater deficits in elders with neck pain, beyond those occurring with normal aging, support the premise of cervical afferent dysfunction as a contributor to sensorimotor disturbances (Treleaven, 2008a; Kristjansson and Treleaven, 2009).
Deficits in eye movement control were greater in elders with neck pain, in accordance with previous findings that patients with neck disorders may have smooth pursuit eye movement disturbances (Tjell and Rosenhall, 1998; Tjell et al., 2002; Treleaven et al., 2005a; Storaci et al., 2006). The receptors in the cervical region have central and reflex connections to the visual, vestibular and central nervous systems (Treleaven, 2008a; Kristjansson and Treleaven, 2009). An increase in cervico-ocular reflex (COR) gain is thought to compensate for any natural decline in vestibuloocular reflex (VOR) function in the healthy and elderly (Kelders et al., 2003; Montfoort et al., 2008). However, Montfoort et al. (2008) found that this compensation did not occur in patients with cervical injury (whiplash) and reasoned that these subjects were possibly unable to modify both the COR and VOR eye movement responses. They suggested that adaptive processes of the COR and VOR may take a longer time to operate adequately and there may be an imbalance between the reflexes caused by abnormal cervical afferent input. Thus it is possible that disturbances of smooth pursuit eye movements identified in elders with neck pain are more related to altered afferent information from the neck.
Our results indicate that the RFT of vertical perception may be useful in testing an aspect of spatial orientation dysfunction in patients with neck pain. There was a trend for greater errors in the perception of verticality in elders with neck pain than those without neck pain. The pattern of errors showed maximal effect at frame tilts of 108 to 158 with smaller errors at 08 frame tilt and with no frame, in agreement with previous studies (Grod and Diakow, 2002; Bagust, 2005). Perception of verticality requires visual information (external cues) to be integrated with sensory inputs from the vestibular system and neck proprioceptors (internal cues). Altered proprioceptive afferent input originating from the cervical region may result in difficulty in perceiving the vertical orientation. There is, however, an argument that disturbances of spatial orientation may be affected by perceptual style (i.e. field dependence and independence) (Storaci et al., 2006). As yet, this has not been determined in any studies of neck pain. Further research is needed into perceptual style, although this is an unlikely cause of vertical perception difficulty in patients with neck pain.
There was a trend toward greater deficits in balance responses in elders with neck pain than healthy elders. Significant deficits were evident in amplitude of sway, greater in the AP than ML direction, which supports the preliminary findings by Poole et al. (2008). Decreased amplitude of sway was observed with eyes open on a firm surface in the ML direction and a tendency for increased amplitude of sway was observed with eyes open and closed on a firm surface in the AP direction (p = 0.07). No differences in sway energy were found between the groups, although there was a tendency for increased energy of sway in the ML direction on a firm surface in the neck pain group. These results suggest that our elders with neck pain may have a decreased awareness of postural stability (Field et al., 2008; Poole et al., 2008).
The balance deficits were more clearly demonstrated on the firm surface rather than the soft surface which may indicate that tests on soft surfaces were challenging for all elders in our study. This is not surprising given that a significant decline in ability to balance has been demonstrated from the six decade when a soft surface is introduced (with and without vision removed) (Choy et al., 2003). The detrimental changes in the other sensory systems (vestibular/visual) with age may have more influence on postural stability than the role of cervical pain when standing on a softer surface. Nevertheless, further research is required to confirm and explore these findings in elderly populations from mechanistic and best test viewpoints.
Elders with neck pain performed lesser steps in the step test, suggesting disturbances in dynamic standing balance. Reference values for the step test in healthy elderly are 17.4 steps on the left side and 17.7 steps on the right side in 15 s (Hill et al., 1996). Our elders in the neck pain group took 12.7 steps on the left side and 12.3 steps on the right side, which is considerably less than reference values. In addition, the relatively decreased gait speed and cadence while turning the head from side to side and moving the head up-down were observed in elders with neck pain compared to the control group, but significant differences were not found. The gait parameter results do not strongly support Poole et al.’s study demonstrating that elders with neck pain had a slower gait speed and cadence in the head turn condition (Poole et al., 2008).
However, there were differences in how comorbidities were approached between Poole et al’s and this study. Cesari et al. (2005) suggested that older persons with usual gait speed lower than 100 cm/s were at high risk of adverse health-related outcomes. In Bohannon’s study (1997), mean comfortable gait speed ranged from 127.2 cm/s for women to 133.0 cm/s for men, aged in their seventies. Given slight differences in gait measurements between studies, the average gait speed of elders with neck pain in this study (108.2–136.8 cm/s) may not be associated with functional disturbances. Conversely, the decrease in the gait parameters might be a consequence of the challenges inherent in performing dual tasks. There is a need for better understanding of the cause of gait disturbances during challenging walking conditions in elders with neck pain.
Fear of falling as reflected by the mean ABC score was significantly lower in elders with neck pain than those without neck pain. Nevertheless, the ABC score reported by elders with neck pain was still relatively good, suggesting that fear of falling may not be strongly related to fall risk and self-induced restriction of activities (Hatch et al., 2003). Further research is required to explore the clinical significance between changes in balance confidence and postural instability in elders with neck pain.
Limitation
The sample size in this study was small. The statistical power levels of the non significant results were less than 0.8, indicating inadequate power to detect statistical significance. It was difficult to recruit elders with neck pain without major comorbidities. Nevertheless, age and the comorbidities remaining after exclusion of major comorbidities, were entered as covariates to control for any potential confounding factors in the analyses of all outcomes. Dizziness could have been a consequence of the neck pain but was included as a covariate and thus may have led to an underestimation of the results. This adds strength to our findings that altered cervical afferent input contributes to disturbances in sensorimotor function in elders with neck pain. However, further research in this area is still required.
Conclusion
The study has determined that overall, sensorimotor disturbances were greater in elders with neck pain than without neck pain after controlling for age and comorbidities. Elders with neck pain have greater deficits in eye movement control, vertical perception and balance, which supports the notion that altered cervical afferent input may contribute to sensorimotor disturbances. Assessment of disturbed sensorimotor function is indicated in elders with neck pain as is assessment of neck disorders in those with falls risk.
Conflict of interest
None.
Funding
This work has been funded by Chiang Mai University.
References:
Ahmed, M.S., Matsumura, B., Cristian, A., 2005.
Age-related changes in muscles and joints.
Phys. Med. Rehabil. Clin. N. Am. 16, 19–39.Akdal, G., Donmez, B., Ozturk, V., Angin, S., 2009.
Is balance normal in migraineurs without history of vertigo?
Headache 49, 419–425.Bagust, J., 2005.
Assessment of verticality perception by a rod-and-frame test: preliminary observations on the use
of a computer monitor and video eye glasses.
Arch. Phys. Med. Rehabil. 86, 1062–1064Bohannon, R.W., 1997.
Comfortable and maximum walking speed of adults aged 20–79 years: reference values and determinants.
Age Ageing 26, 15–19Bolton, P.S., 1998.
The Somatosensory System of the Neck and its Effects on the Central Nervous System
J Manipulative Physiol Ther. 1998 (Oct); 21 (8): 553–563Bove, M., Courtine, G., Schieppati, M., 2002.
Neck muscle vibration and spatial orientation during stepping in place in humans.
J. Neurophysiol. 88, 2232–2241Boyd-Clark, L.C., Briggs, C.A., Galea, M.P., 2002.
Muscle spindle distribution, morphology, and density in longus colli and multifidus muscles
of the cervical spine.
Spine 27, 694–701Cesari, M., Kritchevsky, S.B., Penninx, B.W., Nicklas, B.J., Simonsick, E.M., 2005.
Prognostic value of usual gait speed in wellfunctioning older people—results from the Health,
Aging and Body Composition Study.
J. Am. Geriatr. Soc. 53, 1675–1680Chamberlin, M.E., Fulwider, B.D., Sanders, S.L., Medeiros, J.M., 2005.
Does fear of falling influence spatial and temporal gait parameters in elderly persons beyond changes
associated with normal aging?
J. Gerontol. A: Biol. Sci. Med. Sci. 60, 1163–1167Choy, N.L., Brauer, S., Nitz, J., 2003.
Changes in postural stability in women aged 20 to 80 years.
J. Gerontol. A: Biol. Sci. Med. Sci. 58, 525–530Courtine, G., Papaxanthis, C., Laroche, D., Pozzo, T., 2003.
Gait-dependent integration of neck muscle afferent input.
Neuroreport 14, 2365–2368Cress, M.E., Schechtman, K.B., Mulrow, C.D., Fiatarone, M.A., Gerety, M.B. 1995.
Relationship between physical performance and self-perceived physical function.
J. Am. Geriatr. Soc. 43, 93–101della Volpe, R., Popa, T., Ginanneschi, F., Spidalieri, R., 2006.
Changes in coordination of postural control during dynamic stance in chronic low back pain patients.
Gait Posture 24, 349–355Field, S., Treleaven, J., Jull, G., 2008.
Standing balance: a comparison between idiopathic and whiplash-induced neck pain.
Man Ther. 13, 183–191Gill, J., Allum, J.H., Carpenter, M.G., Held-Ziolkowska, M., Adkin, A.L., Honegger, F. 2001.
Trunk sway measures of postural stability during clinical balance tests: effects of age.
J. Gerontol. A: Biol. Sci. Med. Sci. 56, M438–M447Grod, J.P., Diakow, P.R., 2002.
Effect of neck pain on verticality perception: a cohort study.
Arch. Phys. Med. Rehabil. 83, 412–415Hatch, J., Gill-Body, K.M., Portney, L.G., 2003.
Determinants of balance confidence in community-dwelling elderly people.
Phys. Ther. 83, 1072–1079Hawk, C., Hyland, J.K., Rupert, R., Colonvega, M., Hall, S., 2006.
Assessment of balance and risk for falls in a sample of community-dwelling adults aged 65 and older.
Chiropr. Osteopat. 14, 3Hill, K.D., Bernhardt, J., McGann, A.M., Maltese, D., Berkovits, D., 1996.
A new test of dynamic standing balance for stroke patients: reliability, validity,
and comparison with healthy elderly.
Physiother. Can. 48, 257–262Humphreys, B.K., 2008.
Cervical outcome measures: testing for postural stability and balance.
J. Manipulative Physiol. Ther. 31, 540–546Jacobson, G.P., McCaslin, D.L., Grantham, S.L., Piker, E.G., 2008.
Significant vestibular system impairment is common in a cohort of elderly patients
referred for assessment of falls risk.
J. Am. Acad. Audiol. 19, 799–807Jull, G., Sterling, M., Treleaven, J., O’Leary, S., 2008.
Whiplash, Headache and Neck Pain.
Churchill Livingstone, EdinburghKelders, W.P., Kleinrensink, G.J., van der Geest, J.N., Feenstra, L., 2003.
Compensatory increase of the cervico-ocular reflex with age in healthy humans.
J. Physiol. 553, 311–317Kogler, A., Lindfors, J., Odkvist, L.M., Ledin, T., 2000.
Postural stability using different neck positions in normal subjects and patients with neck trauma.
Acta Otolaryngol. 120, 151–155Kristjansson E, Treleaven J.
Sensorimotor Function and Dizziness in Neck Pain: Implications for Assessment and Management
J Orthopaedic Sports Physical Therapy 2009 (May); 39 (5): 364–377Liaw, M.Y., Chen, C.L., Pei, Y.C., Leong, C.P., Lau, Y.C., 2009.
Comparison of the static and dynamic balance performance in young, middle-aged, and elderly healthy people.
Chang Gung Med. J. 32, 297–304Maki, B.E., 1997.
Gait changes in older adults: predictors of falls or indicators of fear.
J. Am. Geriatr. Soc. 45, 313–320March, L.M., Brnabic, A.J., Skinner, J.C., Schwarz, J.M., Finnegan, T., Druce, J 1998.
Musculoskeletal disability among elderly people in the community.
Med. J. Aust. 168, 439–442Montfoort, I., Van Der Geest, J.N., Slijper, H.P., De Zeeuw, C.I., Frens, M.A., 2008.
Adaptation of the cervico- and vestibulo-ocular reflex in whiplash injury patients.
J. Neurotrauma 25, 687–693Pajala, S., Era, P., Koskenvuo, M., Kaprio, J., Tormakangas, T., Rantanen, T., 2008.
Force platform balance measures as predictors of indoor and outdoor falls in community-dwelling
women aged 63–76 years.
J. Gerontol. A: Biol. Sci. Med. Sci. 63, 171–178Poole, E., Treleaven, J., Jull, G., 2008.
The influence of neck pain on balance and gait parameters in community-dwelling elders.
Man Ther. 13, 317–324Powell, L.E., Myers, A.M., 1995.
The Activities-specific Balance Confidence (ABC) Scale.
J. Gerontol. A: Biol. Sci. Med. Sci. 50A, M28–M34Revel, M., Andre-Deshays, C., Minguet, M., 1991.
Cervicocephalic kinesthetic sensibility in patients with cervical pain.
Arch. Phys. Med. Rehabil. 72, 288–291Rix, G.D., Bagust, J., 2001.
Cervicocephalic kinesthetic sensibility in patients with chronic, nontraumatic cervical spine pain.
Arch. Phys. Med. Rehabil. 82, 911–919Salzman, B., 2010.
Gait and balance disorders in older adults.
Am. Fam. Phys. 82, 61–68.Schrager, M.A., Kelly, V.E., Price, R., Ferrucci, L., Shumway-Cook, A., 2008.
The effects of age on medio-lateral stability during normal and narrow base walking.
Gait Posture 28, 466–471Shumway-Cook, A., Brauer, S., Woollacott, M., 2000.
Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test.
Phys. Ther. 80, 896–903Storaci, R., Manelli, A., Schiavone, N., Mangia, L., Prigione, G., Sangiorgi, S., 2006.
Whiplash injury and oculomotor dysfunctions: clinical-posturographic correlations.
Eur. Spine J. 15, 1811–1816Tjell, C., Rosenhall, U., 1998.
Smooth pursuit neck torsion test: a specific test for cervical dizziness.
Am. J. Otol. 19, 76–81Tjell, C., Tenenbaum, A., Sandstorm, S., 2002.
Smooth pursuit neck torsion test: a specific test for whiplash associated disorders?
J. Whiplash Associated Disorders 1, 9–24Treleaven, J., 2008a.
Sensorimotor disturbances in neck disorders affecting postural stability, head and eye movement control.
Man Ther. 13, 2–11Treleaven, J., 2008b.
Sensorimotor disturbances in neck disorders affecting postural stability, head and eye movement
control—Part 2. Case studies.
Man Ther. 13, 266–275Treleaven, J., Jull, G., LowChoy, N., 2005a.
Smooth pursuit neck torsion test in whiplash-associated disorders: relationship to self-reports
of neck pain and disability, dizziness and anxiety.
J. Rehabil. Med. 37, 219–223Treleaven, J., Jull, G., Sterling, M., 2003.
Dizziness and Unsteadiness Following Whiplash Injury: Characteristic Features and Relationship
With Cervical Joint Position Error
J Rehabil Med 2003 (Jan); 35 (1): 36–43Treleaven, J., LowChoy, N., Darnell, R., Panizza, B., Brown-Rothwell, D., Jull, G., 2008.
Comparison of sensorimotor disturbance between subjects with persistent whiplash-associated disorder
and subjects with vestibular pathology associated with acoustic neuroma.
Arch. Phys. Med. Rehabil. 89, 522–530Treleaven, J., Murison, R., Jull, G., LowChoy, N., Brauer, S., 2005b.
Is the method of signal analysis and test selection important for measuring standing balance in
subjects with persistent whiplash?
Gait Posture 21, 395–402Vernon, H., Mior, S., 1991.
The Neck Disability Index: A Study of Reliability and Validity
J Manipulative Physiol Ther 1991 (Sep); 14 (7): 409–415Vuillerme, N., Pinsault, N., 2009.
Experimental neck muscle pain impairs standing balance in humans.
Exp. Brain Res. 192, 723–729Vuillerme, N., Pinsault, N., Bouvier, B., 2008.
Cervical joint position sense is impaired in older adults.
Aging Clin. Exp. Res. 20, 355–358Woollacott, M.H., Tang, P.F., 1997.
Balance control during walking in the older adult: research and its implications.
Phys. Ther. 77, 646–660.
Return to SENIOR CARE
Since 1-25-2019


| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |